
Abstract
Aim. The study aims to explore the expression levels and clinicopathological significance of BRAF V600E and mucin 6 in intrahepatic cholangiocarcinoma. Method. Immunohistochemistry for BRAF V600E and mucin 6 was performed in 110 patients with intrahepatic cholangiocarcinoma. Subsequently, a comprehensive review of medical records and clinicopathological analysis was undertaken. Results. BRAF V600E expression was detected in 11 patients (10%); mucin 6 expression was observed in 19 intrahepatic cholangiocarcinoma specimens (17%). Thereafter, Cox regression models indicated that positive expression of either MUC6 positive (hazard ratio = 0.091, 95% confidence interval = 0.034-0.247, P < .001) and BRAF V600E positive (hazard ratio =0.150, 95% confidence interval = 0.058-0.388, P < .001) was significantly linked with longer overall survival for intrahepatic cholangiocarcinoma patients. Conclusion. The study concludes that positive expression of BRAF V600E and mucin 6 could potentially implied significant survival benefits for patients diagnosed with intrahepatic cholangiocarcinoma.
Introduction
Intrahepatic cholangiocarcinoma, originating from the epithelial lining of the intrahepatic bile duct beyond the second-order biliary system, accounts for about 10% to 20% of primary liver cancers.1,2 Based on its anatomical location, intrahepatic cholangiocarcinoma falls under one of the three cholangiocarcinoma categories: intrahepatic, hilar, and extrahepatic. As a poorly understood variant of cholangiocarcinoma, intrahepatic cholangiocarcinoma was histologically considered to be the least common category of the above three. 3 Over the past three decades, there has been a global rise in the incidence and mortality of intrahepatic cholangiocarcinoma, whereas the incidence of all other cholangiocarcinoma forms has either remained stable or declined.4–8 The rarity of intrahepatic cholangiocarcinoma presents significant challenges to both the understanding of disease pathogenesis and the development of effective treatment strategies. Surgery has been established as the mainstay of therapy and offered the hope of prolonged survival for patients with intrahepatic cholangiocarcinoma. However, postoperative long-term outcome stays unsatisfactory, with 5-year survival rate of around 30% to 35%. 9 Similarly, no significant survival advantages were demonstrated by locoregional neoadjuvant or palliative therapies.10–12
With great improvement in tumor biology, bio-molecular markers from biopsy, serum sample, or postoperative specimens may be able to further predict tumor behavior. Consequently, identifying a novel prognostic predictor for early diagnosis, preventive measures, and therapeutic regimens of intrahepatic cholangiocarcinoma is of clinical significance and urgently needed.
The BRAF (v-RAF murine sarcoma viral oncogene homolog B) gene encodes a protein that belongs to the RAF family of serine/threonine protein kinases; it is an integral component of the MAP (mitogen-activated protein) kinase cascade.13–15 BRAF is a protein kinase and part of the MAP kinase signaling cascade concerning transduction of a growth signal from the membrane to the nucleus via a chain of protein kinases and account for cellular proliferation and survival. 13 It is recognized that an activating hotspot mutation typically occurs at the V600E site, leading to constitutive MAPK signaling and uncontrolled cellular growth. 14 In-vitro test has shown that V600E mutation exhibits nearly a 500-fold greater activity than wild-type BRAF and can promote transformation.13,14 Hence, BRAF V600E might have functional roles in tumor progression and metastasis, potentially providing new therapeutic opportunities for intrahepatic cholangiocarcinoma. To date, aberrant expression of BRAF V600E is increasingly being recognized as an independent negative prognostic factor in latestage colorectal cancer and is one of the most consistent molecular markers that confer a poor outcome. 16 Similarly, BRAF V600E expressions have been demonstrated to hold prognostic value in other malignancies.14,15,17,18
Mucins are heavily glycosylated glycoproteins and play an important protective role in cells, in part serving as a barrier to the epithelial surface and to tumors cells. Mucin 6 expression has been investigated in pancreatic intraepithelial neoplasms, pancreatic adenocarcinomas, gallbladder carcinomas and their dysplastic lesions, cholangiocarcinomas, and various other carcinomas.
However, expression of BRAF V600E and mucin 6 and their prognostic significance in intrahepatic cholangiocarcinoma stay unexplored. Given this, we employed a tissue microarray approach to immunohistochemically evaluate the expression of BRAF V600E and mucin 6, and their prognostic values in intrahepatic cholangiocarcinoma. Additionally, we investigated the associations between BRAF V600E and mucin 6 expression and the clinicopathological features of the included Chinese patients with intrahepatic cholangiocarcinoma.
Materials and Methods
Patients and Tumor Samples
The study was reviewed and approved by the Ethics Committees of the Hospital. From 2005 to 2010, a total of 110 tissue samples (paraffin embedded sections) were collected from surgically resected specimens of 110 corresponding patients with pathologically confirmed intrahepatic cholangiocarcinoma at the Department of Pathology. The inclusion criteria were as follows: (1) age: 18–80 years, (2) intrahepatic cholangiocarcinoma diagnosed based on the American Association for the Study of Liver Diseases guidelines or postoperative pathological examination, (3) The patients with R0 resection confirmed by postoperative pathology examination, (4) No prior history of another cancer in the last 5 years, (5) The patients provide informed and signed consent to participate in this research.
For all the patients enrolled in the study, demographic data and preoperative presentations were collected and analyzed by reviewing the medical computerized database; the perioperative records and pathology reports were thoroughly reviewed; supplementary follow-up was carried out by telephone interviews with the patients.
Construction of Tissue Microarray
All archival formalin-fixed, paraffin-embedded sections were carefully reviewed and selected from corresponding haematoxylin and eosin stained sections to identify and mark representative tumorous areas, as previously documented.19,20 Single 0.6-mm cores of tissue taken from the above-mentioned representative tumorous area were used to assemble the arrays. The assembled array blocks were sliced into 4-mm-thick sections and mounted on glass slides. In total, all patients (n = 110) tumor samples were evaluated for staining on the array.
Immunohistochemistry
Immunohistochemical staining of the tissues was performed using the Envision two-step method. 21 Briefly, formalin-fixed, paraffin wax-embedded, and 4-µm-thick sections were prepared as previously described. 21 The slides were incubated serially (40 min each, at room temperature) with the following primary antibodies: BRAF V600E (1:100; Gene Tech, Shanghai), and mucin 6 (1:150; Dako, Denmark). Each incubation with primary antibody was followed by 40-min incubation at room temperature with horseradish peroxidase-labeled polymer. The staining was developed by incubation with diaminobenzidine substrate-chromogen for 5-10 min, and a hematoxylin counterstain was applied. Both negative and positive controls for each antibody were performed.
Evaluation of score
Staining was graded for intensity of staining (0, negative; 1, weak; 2, moderate; 3, strong) and percentage of cells stained (0, < 5%; 1, 6%-25%; 2, 26%-50%; 3, > 50%). The final score was determined by the combined staining score (extent + intensity). Score 4-6 was defined as positive expression. 22
Definition
In the present study, all 110 patients had received curative resection. Lymphatic invasion mostly referred to lymph node involvement at the site of the hepatoduodenal ligament (regional lymph nodes, N1 disease based on the eighth edition of the American Joint Committee on Cancerstaging system). According to the macroscopic appearances proposed by the WHO Classification of tumors of the Digestive system (2010), intrahepatic cholangiocarcinoma includes four morphological growth subtypes: the mass-forming subtype, the periductal infiltrating subtype, and the intraductal growth subtype, and the mixed subtype. Morphological growth subtypes were defined based on preoperative imaging and the macroscopic description in the pathological report. Tumor histological subtypes were pathologically identified according to the predominant features.
Statistical Analysis
Statistical analyses were carried out using SPSS v26.0. Long-term survival was estimated using the Kaplan-Meier method and compared by the log-rank test. Data are the mean ± standard deviation or median (range). P < .05 was considered statistically significant. The significant factors in univariate analysis were used for the performance of the multivariate Cox-regression analysis.
Results
Demographic Data and Clinicopathological Characteristics of the Patients
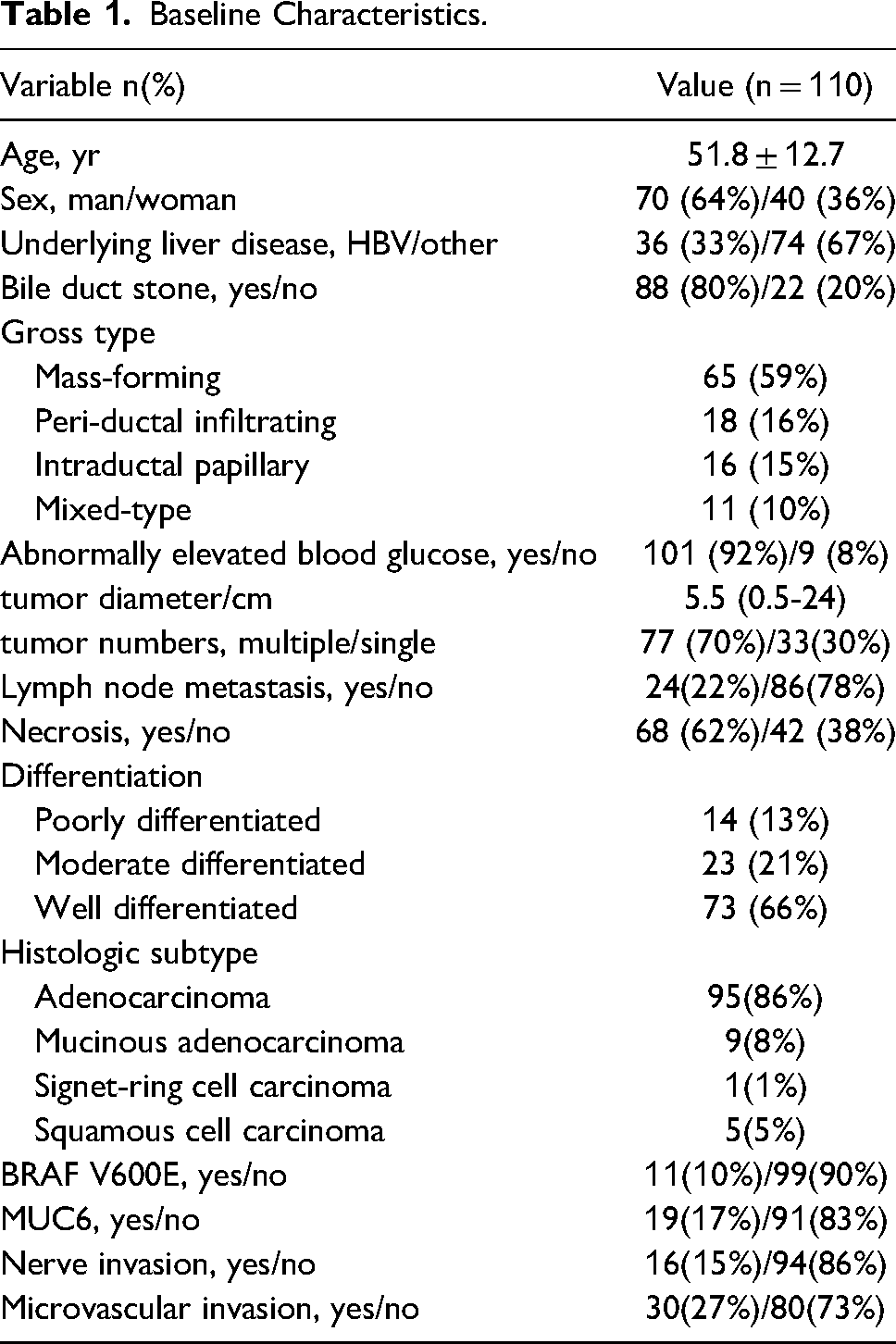
Demographic data and clinicopathological characteristics of the patients were presented in Table 1. In our survey of 110 patients of intrahepatic cholangiocarcinoma, there were 70 (64%) men and 40 (36%) women; the average age was 51.8 ± 12.7 years. The tumor size ranged from 0.5 cm to 24 cm (mean 5.5 cm). Regarding histologic subtypes, ninety-five (86%) were adenocarcinoma, 9 (8%) were mucinous adenocarcinoma, one (1%) was signet-ring cell carcinoma and 5 (5%) were squamous cell carcinoma. In regards to differentiation, fourteen (13%) were poor grade differentiation, twenty-three (21%) moderate grade differentiation and 73 (66%) well grade differentiation. The median follow-up length of the patients was 56 months.
Baseline Characteristics.
Expression of BRAF V600E and Mucin 6
Both BRAF V600E and mucin 6 staining were assessed by immunohistochemistry in all 110 intrahepatic cholangiocarcinoma specimens. As illustrated in Figures, BRAF V600E expression was detected in 11 patients (10%, Figure 1); mucin 6 staining was observed in 19 patients (17%, Figure 2).
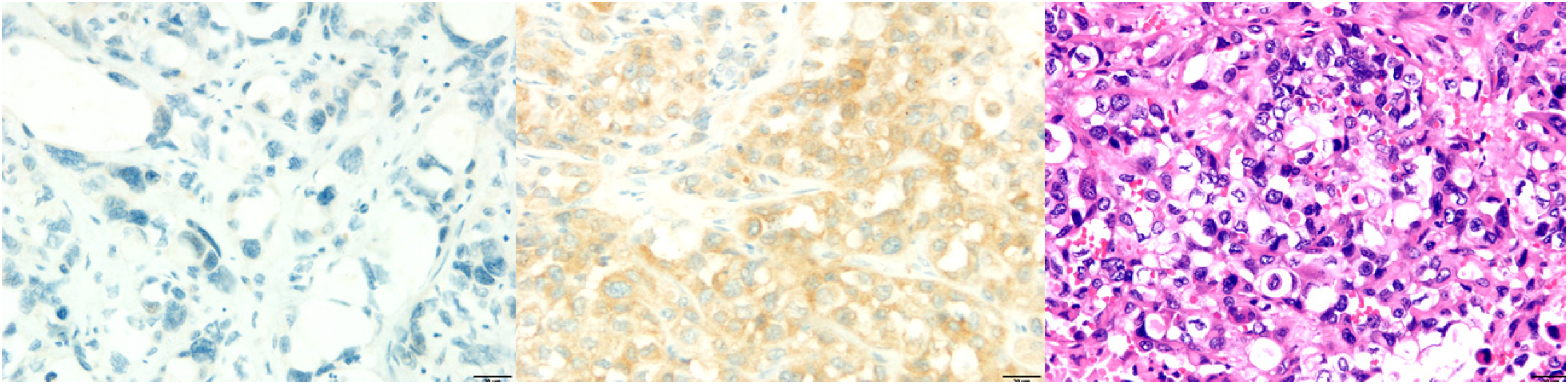
The expression of BRAF V600E in pathological tissue sections.
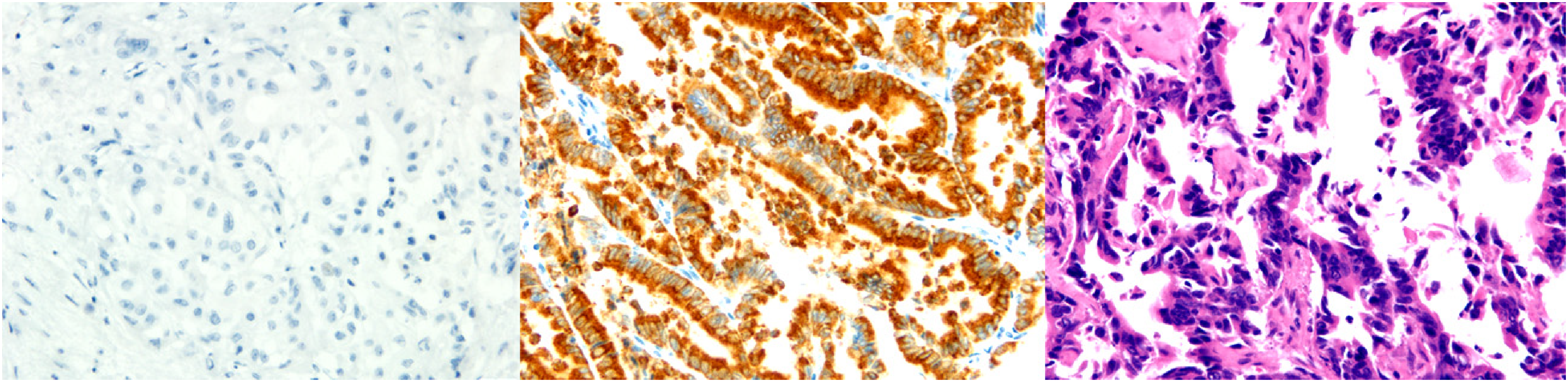
The expression of mucin 6 in pathological tissue sections.
Survival Analysis
For survival analysis, the median overall survival of the 110 patients was 16 months (Standard Deviation 2.26). The patients were categorized into positive or negative groups according to the expression of the markers of interest. The patients with positive expression of BRAF V600E had a longer median survival (46 months) than those with no expression (13 months), and the difference was statistically significant (P = .016, Figure 3). Patients with positive mucin 6 expression had not reached median survival time, whereas those in the negative group showed a median survival of a mere 13 months (P < .001, Figure 4). Differences in one-, three-, and five-year OS rates between positive BRAF V600E expression group and the negative group were also statistically significant (91% vs 53%, 59% vs 24%, and 12% vs 2%, respectively). Differences in one-, three-, and five-year OS rates between positive mucin 6 expression group and the negative group were also statistically significant (100% vs 49%, 71% vs 14%, and 13% vs 0%, respectively).
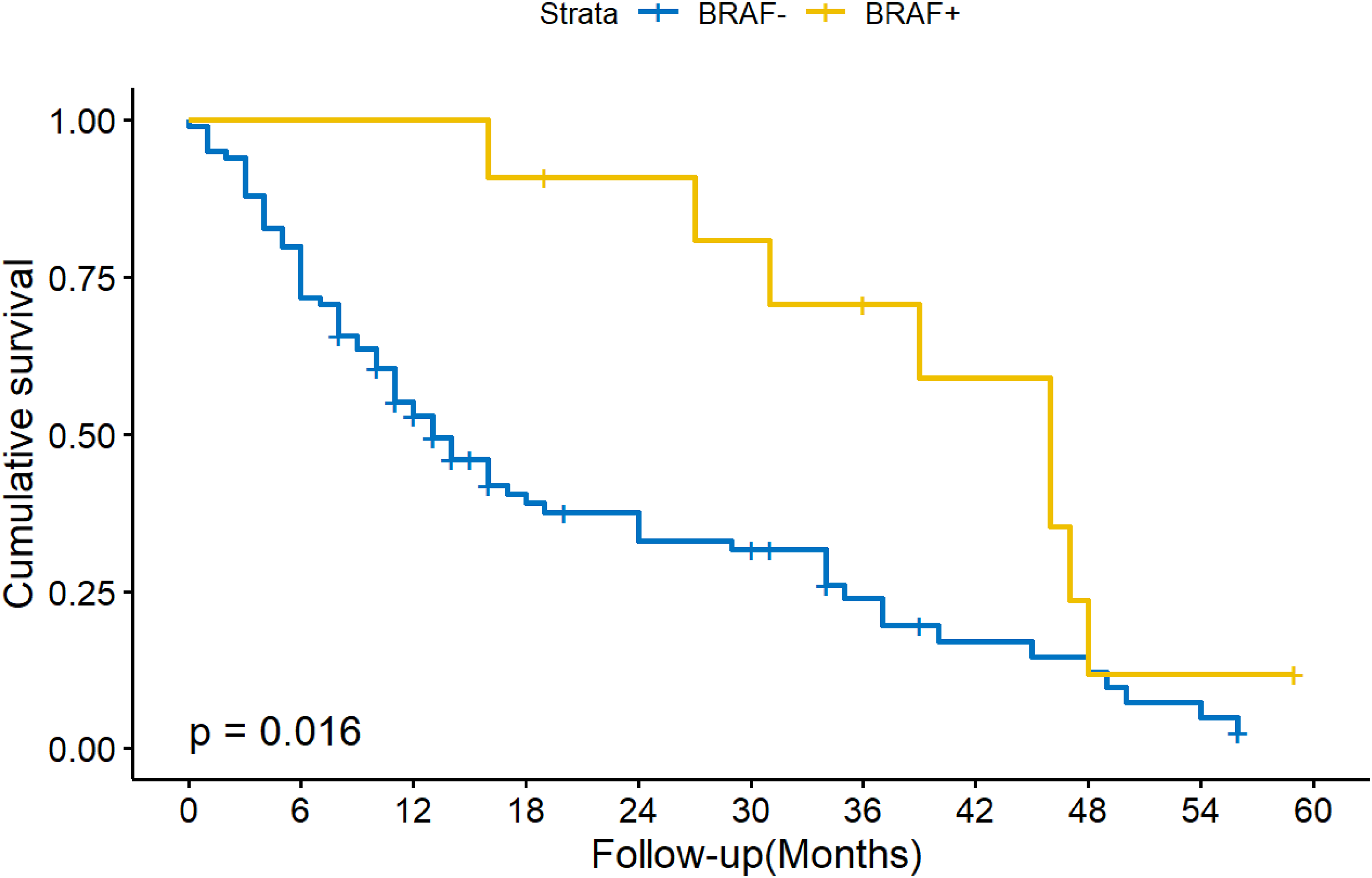
K-M curve of the OS in intrahepatic cholangiocarcinoma patients receiving surgery with positive or negative BRAF V600E.
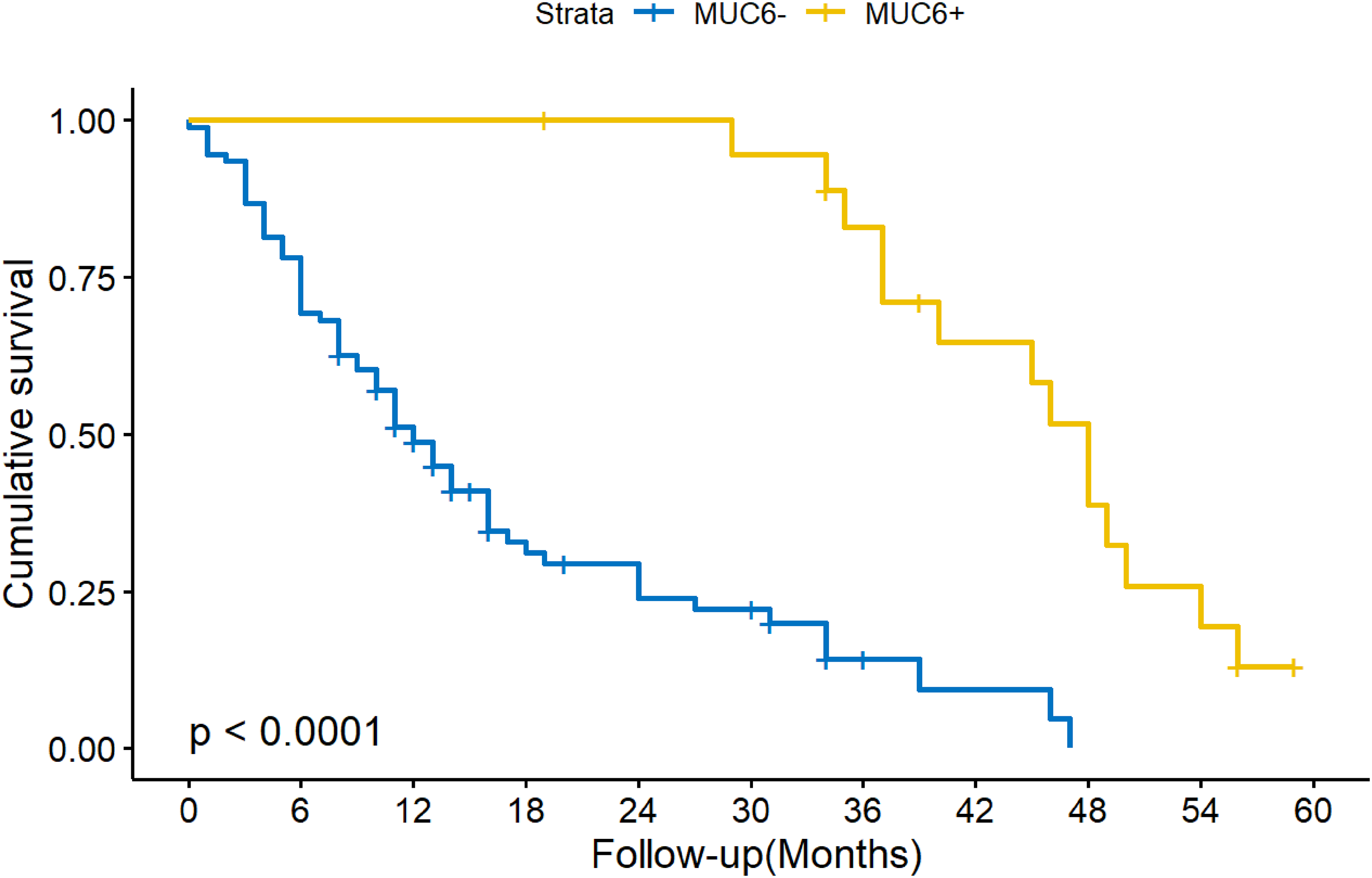
K-M curve of the OS in intrahepatic cholangiocarcinoma patients receiving surgery with positive or negative MUC6.
The Results of Cox
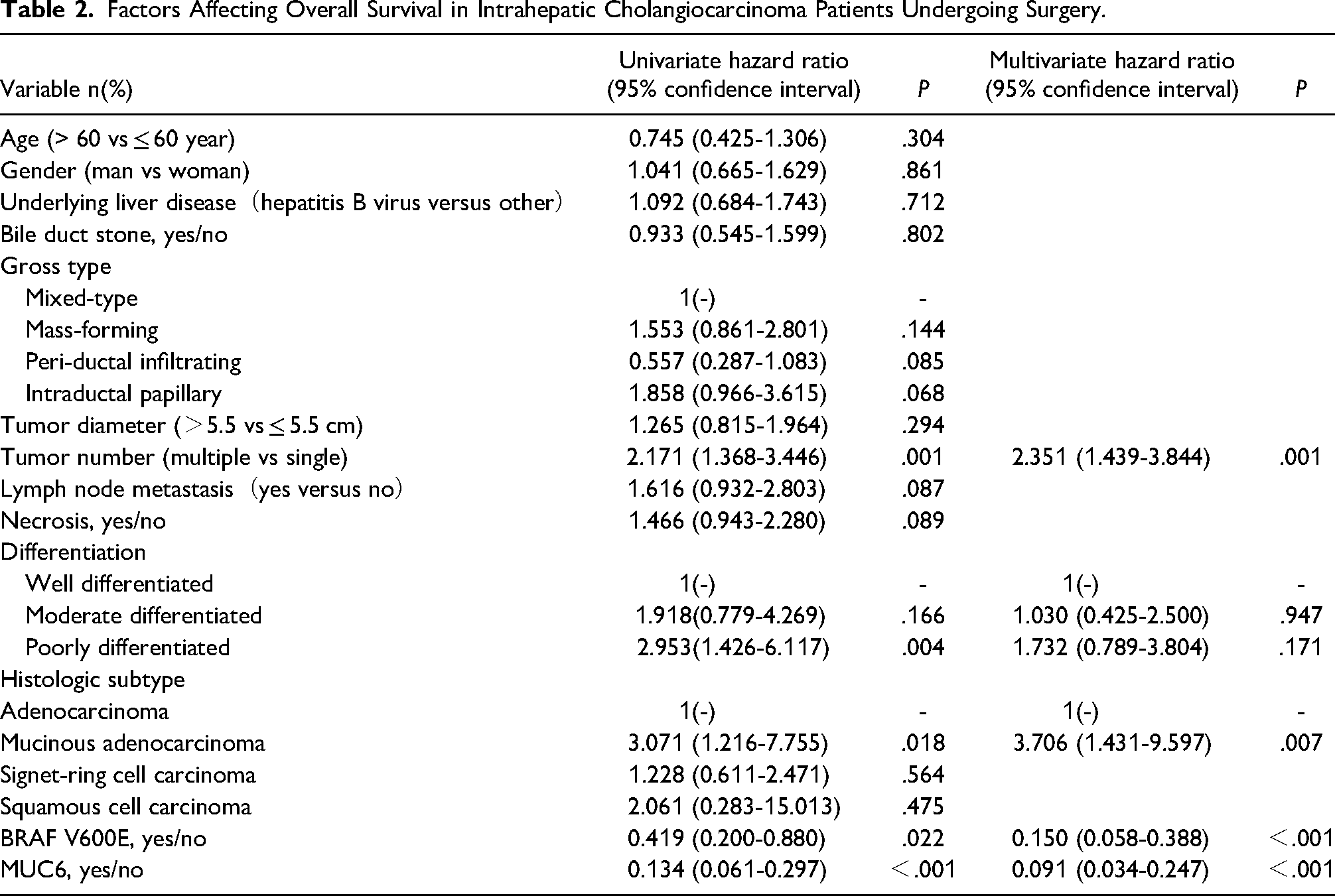
Multivariable Cox proportional hazards regression model was done on the variables strongly linked to intrahepatic cholangiocarcinoma-related deaths. Four factors were identified as significant factors related to intrahepatic cholangiocarcinoma recurrence: MUC6 positive (hazard ratio = 0.091, 95% confidence interval = 0.034-0.247, P < .001), BRAF V600E positive (hazard ratio =0.150, 95% confidence interval = 0.058-0.388, P < .001), mucinous adenocarcinoma compared to adenocarcinoma (hazard ratio =3.706, 95% confidence interval = 1.431-9.597, P = .007) and multiple tumors (hazard ratio = 2.351, 95% confidence interval = 1.439-3.844, P = 0.001) (Table 2).
Factors Affecting Overall Survival in Intrahepatic Cholangiocarcinoma Patients Undergoing Surgery.
BRAF V600E*Mucin 6 Cross-Tabulation.
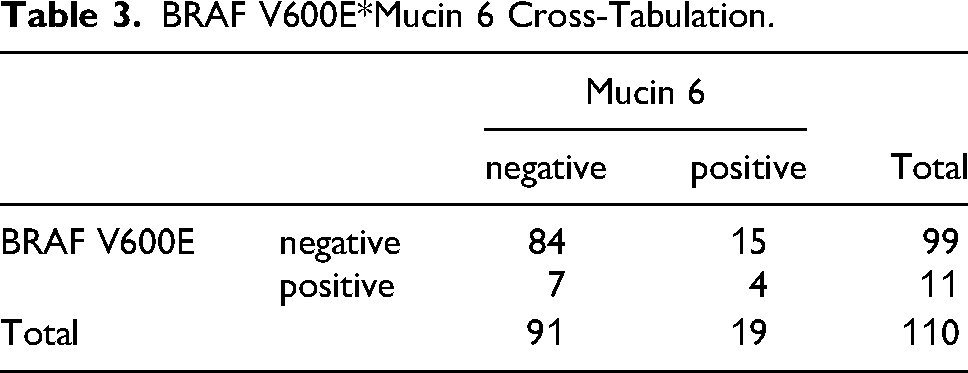
We performed a correlation analysis of the expression of BRAF V600E and mucin 6 and did not find a significant correlation(P = .077) between the expression of the two genes (Table 3).
The correlation between the expression of either of the immunohistochemical markers and tumor differentiation was performed and showed in Table 4 and Table 5. There was no statistically significant correlation between the expression of either gene and the degree of tumor differentiation (P = .843/.725).
BRAF V600E *Tumor Differentiation Cross-Tabulation.

Mucin 6 *Tumor Differentiation Cross-Tabulation.

Discussion
In this study, we performed immunohistochemical investigation of BRAF V600E and mucin 6 expressions, evaluated their prognostic values, and explored their associations with clinicopathological features in intrahepatic cholangiocarcinoma patients using a tissue microarray approach. Through analysis of clinical data and follow-up data, we found that among the patients included in this study, BRAF V600E expression was pathologically diagnosed in 11 patients and mucin 6 expression was found in 19 patients. The statistical analysis revealed the tendency of significant association between the expression of BRAF V600E and mucin 6. KM analysis revealed that patients with positive BRAF V600E expression had a significantly longer median survival than those with negative expression (46 months vs 13 months, P = .016). A similar conclusion was reached for mucin 6 protein expression analysis (P < .001), and a comparable trend was observed in the comparison of overall survival rates during the same period. Additionally, our statistical results suggest that MUC6 positive, BRAF V600E positive, mucinous adenocarcinoma and multiple tumors were significantly associated with the prognosis of intrahepatic cholangiocarcinoma patients. In previous studies, there was strong overall consistency between BRAF V600E immunohistochemistry and BRAF V600E mutation molecular testing, with both sensitivity and specificity reaching over 90%. 23 Therefore, the exploration of the correlation between BRAF immunohistochemistry results and prognosis in this study is also credible.
The findings of this study indicate that intrahepatic cholangiocarcinoma patients with positive expression of the BRAF V600E gene have a favorable prognosis, contrary to the current mainstream conclusion that positive expression of BRAF V600E is associated with a worse prognosis.24,25 We posit that a significant proportion of intrahepatic cholangiocarcinomas exhibiting BRAF V600E positivity predominantly arise from the small bile duct epithelia. This assertion is substantiated by existing scholarly literature, which demonstrates a predilection for BRAF V600E mutations in intrahepatic cholangiocarcinomas of small bile duct origin. 26 Intrahepatic cholangiocarcinoma has two origins: one originating in the small bile duct group (lumen diameter <300 μm) and the other in the large bile duct group (lumen diameter 300-800 μm).27,28 Bile duct adenomas are potential precancerous lesions in the small bile duct group and may lead to intrahepatic cholangiocarcinoma. 29 In previous studies, the detection rate of BRAF mutations in tumours of intrahepatic cholangiocarcinoma patients ranged from 5% to 22%.30–32 Moreover, the detection rate of BRAF V600E gene expression in intrahepatic bile duct adenomas has been reported to be over 50%. 33 The possibility of biliary adenomas as intrahepatic cholangiocarcinoma of small bile duct origin is further suggested by the presence of positive expression of the BRAF V600E gene in pathological specimens of both tumours. We reported four patients with intrahepatic bile duct cell carcinoma whose tumours had malignant transformation from intrahepatic bile duct adenoma.34,35 In contrast, intrahepatic cholangiocarcinoma of small bile duct origin treated with surgery has a better prognosis than intrahepatic cholangiocarcinoma of large duct origin (5-year RFS 38% vs 10%, 5-year OS 60% vs 20%).34,35 Therefore, the results of this study show that patients with a positive BRAF V600E have a better prognosis.
In our study, we observed a significant correlation between positive mucin 6 expression and the survival time of intrahepatic cholangiocarcinoma patients. Those with mucin 6 positive status showed a significantly longer survival time compared to those with mucin 6 negative. In previous studies, we have also found that intrahepatic cholangiocarcinoma of biliary adenoma origin can be positive for the expression of the MUC6 gene, just as it is in biliary adenoma. 35 Similarly, patients with intrahepatic cholangiocarcinoma derived from bile duct adenomas exhibit a relatively better prognosis. The results of several studies also support the idea that intrahepatic cholangiocarcinoma patients with positive mucin 6 expression have a longer survival time. 36 In previous studies, it was found that intrahepatic cholangiocarcinoma patients with positive expression of mucin 6 glycoprotein had more differentiated tumours and that mucin 6 expression gradually decreased with the progression of tumour malignancy.36,37 And MUC6 positive intrahepatic cholangiocarcinoma is likely to have lower levels of invasiveness and extension of cancer cells, which contributes to the relatively good prognosis of patients.38,39 Based on these findings, we postulate that intrahepatic cholangiocarcinoma patients with positive mucin 6 expression tend to have more differentiated tumors, potentially contributing to their longer survival.
In the analysis of the clinicopathological features potentially influencing the prognosis of patients with intrahepatic cholangiocarcinoma, MUC6 positive (hazard ratio = 0.091, 95% confidence interval = 0.034-0.247, P < .001), BRAF V600E positive (hazard ratio =0.150, 95% confidence interval = 0.058-0.388, P < .001), mucinous adenocarcinoma compared to adenocarcinoma (hazard ratio =3.706, 95% confidence interval = 1.431-9.597, P = .007) and multiple tumors (hazard ratio = 2.351, 95% confidence interval = 1.439-3.844, P = .001). Typically, the number of tumors in a patient is often considered to be positively correlated with the heterogeneity of the tumor, so that patients with a high number of tumors have a more heterogeneous tumour and therefore a worse prognosis. Multiple tumors, or satellite lesions, have been reported in several publications as significant risk factors for survival in intrahepatic cholangiocarcinoma patients.40–42 With regard to histopathological subtypes of intrahepatic cholangiocarcinoma, patients with mucinous adenocarcinoma have a significantly worse prognosis compared to those with adenocarcinoma. A similar trend is observed in several other cancer types, like gastric cancer, where the mucinous adenocarcinoma subtype is associated with a worse prognosis.43,44 This demonstrates that patients with multiple tumours and pathological findings suggestive of mucinous adenocarcinoma should be given a more active postoperative focus on survival. Besides, mucinous adenocarcinoma is a relatively rare disease in intrahepatic cholangiocarcinoma, with reported incidence rates ranging from 3% to 9%. 45 In this study, the incidence rate of mucinous adenocarcinoma was 8% due to the use of TMA as a pathological research method, which may be attributed to the fact that the core slice containing mucinous adenocarcinoma was not obtained during sampling, and relatively high grade differentiated tissue slices were obtained instead, resulting in certain research bias.
This study mainly used tissue microarray method for pathological evaluation. Tissue microarray is mainly used for high-throughput research on candidate genes and their proteins identified by molecular biology techniques such as DNA microarrays. One potential limitation of tissue microarray is that the small cores sampled may not accurately represent the entire tumors. 46 Although studies have demonstrated good accuracy of tissue microarray in pathologically detecting certain homogeneous solid tumor cells, there is currently no evidence to support its representation of all data from large pathological sections. Therefore, in the follow-up of this study, pathological sections need to be used for evaluation to increase the accuracy of the research. 47 Our current work has certain innovations and strengths. (1) To date, to our best knowledge, BRAF V600E and mucin 6 expression were not widely reported in solid tumors and the present work served as the large-volume study for addressing the association between mucin 6 expression and survival outcomes as well as clinicopathological features in intrahepatic cholangiocarcinoma patients. (2) By applying strict patient selection criteria, a total of 110 patients were included and analyzed, forming a large retrospective cohort (especially for a rare disease) from which to make clinical reasonable assumptions about patients. Despite the mentioned strengths or potential clinical utility, limitation should also be admitted. Namely, the detailed or definite molecular mechanisms implicated in this correlation or process were not explored, thus relatively weakening the conscientiousness and influencing the integrity of our results. Nevertheless, the current study undoubtedly took the first step in developing a persuasive argument for prognostic significances of BRAF V600E and mucin 6 in intrahepatic cholangiocarcinoma.
Conclusion
In conclusion, BRAF V600E positive expression and mucin 6 positive expression implied significant survival benefits for intrahepatic cholangiocarcinoma patients. Hence, BRAF V600E and mucin 6 expression might provide a new tool to discriminate survival for intrahepatic cholangiocarcinoma patients.
Footnotes
Authors’ Contributions
WSR analyzed and interpreted the patient data regarding the expression and clinicopathological significance of BRAF V600E and Mucin 6 in ICC, contributed to the design of the research methodology, including data collection methods and analysis techniques and conducted data analysis and interpreted the results to derive meaningful conclusions. WMH performed the data collection of the data of pathology, and was a major contributor in writing the manuscript. ZQH revised the article according to the request, polished the article. THW critically reviewed the final manuscript, ensuring the accuracy of the content before submission. WZB critically reviewed the final manuscript, ensuring the accuracy of the content before submission and may have been involved in securing funding for the research. All authors read and approved the final manuscript.
Additional Information
All authors have contributed significantly, and all authors are in agreement with the content of the manuscript.
Availability of Data and Materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Our research was conducted with informed consent from both patients and their family members, and all study analyses were carried out with the patient's consent signature.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The study was reviewed and approved by the Ethics Committees of the PLA General Hospital (Beijing, China)
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.