
Abstract
Autoimmune metaplastic atrophic gastritis (AMAG) is a chronic immune-mediated form of gastritis characterized by damage to oxyntic cells, ultimately resulting in both iron deficiency with or without anemia and pernicious anemia. The current dogma is that AMAG is a disease of White Northern European women of advanced age. We, therefore, sought to examine the prevalence of AMAG in biopsies obtained from populations enriched for self-identified Hispanics for cross-comparison against data from previously reported populations enriched for self-identified White, non-Hispanic patients. To that end, we prospectively collected 1708 sequential gastric biopsies performed at the University of Miami Hospitals/Jackson Health Systems clinics from 1692 patients over a 1-year period as well as pertinent clinical parameters. These Florida data were then compared against data previously collected from the Baltimore population, which has far lower numbers of Hispanic patients. Self-identified race and/or ethnicity were used. From these 1692 patients, we identified 79 patients (4.6%) with AMAG. These included 60 women (76%) and 19 men (24%), with a F:M ratio of 3.1:1. Patients had a median age of 60 years (range: 15–83). Self-identified race and/or ethnicity were: 60 (76.0%) Hispanic, 9 (11.4%) Black, 9 (11.4%) White, and 1 Asian (1.2%). The median age at initial presentation was: 51 years (range: 15–83) in Hispanics, 77.2 years (range: 46–74) in Blacks, 59 years (range: 49–79) in Whites, and 58 years in the only Asian patient. The overall demographics of AMAG largely mirrored the Florida population, with an over-representation of Hispanics (Florida inhabitants self-report as 70% Hispanic). The overall 4.6% prevalence of AMAG in the Florida population differed significantly from the 1.1% in Baltimore (p < .00001), a finding that presumably reflects the large Hispanic population. In fact, the prevalence of AMAG is far higher in Hispanic patients. Awareness of these data should increase recognition of AMAG in this population.
Introduction
Autoimmune metaplastic atrophic gastritis (AMAG) is an uncommon corpus-predominant form of chronic gastritis, characterized by immune-mediated damage to oxyntic glands that results in loss of parietal cell mass, metaplasias (pyloric, intestinal, and pancreatic), and atrophy. The overall prevalence of AMAG has been estimated at 2% of the population above the age of 60 years, many of whom ultimately suffer from pernicious anemia secondary to AMAG. 1 In contrast, autoimmune gastritis is vanishingly rare in children and is associated with tandem extra-gastric immune-related disorders.2,3
The immune-mediated damage to parietal cells in patients with AMAG leads to a gradual inability to absorb vitamin B12 secondary to loss of intrinsic factor and diminished acid production leading to hypochlorhydria and, ultimately, pernicious anemia, a neurodegenerative condition.4,5 From the clinical perspective, serologic studies and clinical follow-up play a critical role in patient management.4,5
Biopsies from the gastric body/fundus are required for diagnosing AMAG.6,7 Endoscopic findings may be subtle and depend on the severity of the disease. 7 Early parietal cell damage may not result in endoscopically detectable mucosal changes. However, as the disease progresses, endoscopic findings may include atrophic mucosal changes with attenuated rugal folds and prominence of submucosal blood vessels.7,8
Histologic features are also variable and ultimately depend on disease progression (Figures 1 and 2). Unfortunately, many pathologists have not been trained to recognize even advanced cases. For this reason, AMAG can be easily overlooked, particularly when it is incompletely developed.9,10 Nonetheless, common histologic features include disorganization of oxyntic glands, intestinal, pyloric, and pancreatic metaplasia of oxyntic glands, basal predominant lymphocytic infiltration, and glandular atrophy or dropout, all to varying degrees. Background reactive gastropathy, particularly in the antral mucosa, is also a common finding, 10 although the antral mucosa may be normal.9,10

(A) Fully developed AMAG. This example of fully developed AMAG shows intestinal and pyloric metaplasia as well as parietal cell loss (20×, magnification). (B) This is from the same fully developed AMAG biopsy. Chromogranin immunohistochemistry highlights striking linear ECL cell hyperplasia defined as >5 ECL cells arranged in a linear fashion (20×, magnification). This is a result of feedback loop interruption secondary to parietal cell loss, which leads to hypergastrinemia in AMAG. (C) Gastrin immunohistochemistry highlights the paucity of G-cells (20×, magnification).

(A) Early/incompletely developed autoimmune metaplastic atrophic gastritis (AMAG). This example of the early pattern of AMAG displays basally oriented lymphoplasmacytic inflammation surrounding oxyntic glands with mild glandular disorganization and mild parietal cell loss (20×, magnification). (B) Higher power magnification demonstrates marked lymphoplasmacytic infiltration of oxyntic glands (40×, magnification).
Patients with autoimmune gastritis are prone to several types of polyps and neoplasms, including hyperplastic polyps, 11 adenomas of the intestinal and pyloric types12,13 (or gastritis-associated “lesions” using the terminology promulgated by European colleagues in the “management of epithelial precancerous conditions and lesions in the stomach”/management of patients with precancerous conditions and lesions of the stomach system 14 ), well-differentiated neuroendocrine tumors of enterochromaffin-like (ECL) cell type (Type 1 carcinoid tumors), lymphomas, other hematologic abnormalities, and adenocarcinomas.
Historically, in the early 20th century, autoimmune gastritis was observed in Baltimore, MD, as a condition affecting Northern European Whites 15 and elderly White patients seemed more likely to have reduced serum vitamin B12 than Black patients. 16 However, in our 21st-century study at the same institution, 1.1% of gastric biopsies showed autoimmune gastritis without racial predilection but with a female predominance (F: M = 2:1). 17 However, in the latter study, there was a trend toward a predominance of Hispanics over Whites and Blacks that failed to meet statistical significance based on low numbers of Hispanic patients in the catchment area. Other studies have shown a similar prevalence of AMAG among Whites, Blacks, and non-White Hispanics.1,18 Interestingly, recent pathology literature continues to promote the concept of autoimmune gastritis as a disease of White women of advanced age. 19
Limited data regarding the natural prevalence of AMAG among individuals from diverse racial and ethnic subgroups are available. This study aimed to examine the prevalence of AMAG in the Florida system, a large, racially/ethnically diverse teaching hospital that is enriched for Hispanics, and compare it to that in a Baltimore hospital population enriched for self-identified Whites that we have previously studied. 17 In addition, clinical awareness as well as adequate sampling of the gastric body and antral mucosa, is imperative due to the numerous clinical comorbidities associated with AMAG.
Methods and Materials
Two of the authors prospectively assessed consecutive in-house gastric biopsies from daily specimens reviewed in the course of routine patient care in the Florida System hospitals and clinics between October 2020 and September 2021. Approval from our Institutional Review Board was obtained to review clinical data. Race and/or ethnicity were recorded from the patients’ electronic medical records; the medical record uses a patient's self-identified race and/or ethnicity. We collected 1708 sequential gastric biopsies performed at our institution's clinics from 1692 patients. Helicobacter pylori (HP) examination was carried out by routine hematoxylin and eosin evaluation and immunohistochemical studies.
Immunohistochemical confirmation was used in a subset of specimens, which demonstrated negative gastrin staining in oxyntic mucosa and linear and/or micronodular ECL cell hyperplasia by synaptophysin or chromogranin staining. Clinical data, including serologic studies and endoscopic findings, were recorded for each patient, when available. Demographics were self-identified by the patients. The data were compared with those from our prior retrospective study using the Chi-square test with publicly available software (https://www.socscistatistics.com/tests/chisquare/default2.aspx). A p-value <.05 was considered statistically significant.
Results
A total of 1708 sequential in-house gastric biopsies from 1692 patients obtained in the course of routine care between October 2020 and September 2021 were reviewed. Among them, we prospectively identified 79 patients (4.6%) with AMAG. These included 60 women (76%) and 19 men (24%), with a F:M ratio of 3.1:1. Patients had a median age of 60 years (range: 15–83). Self-identified demographics as recorded by the patients were as follows: 60 (76.0%) Hispanic, 9 (11.4%) Black, 9 (11.4%) White, and 1 (1.2%) Asian. The results can be seen in Table 1.
Demographics of Autoimmune Metaplastic Atrophic Gastritis (AMAG), South Florida.

Endoscopically detected lesions in AMAG patients included hyperplastic polyps (n = 4; 5%), neuroendocrine neoplasms (n = 3; 3.8%), low-grade B-cell lymphoma (n = 2; 2%), and adenocarcinoma (n = 1; 1%).
A total of 79 gastric biopsies from the body or fundus displayed variable diagnostic features of AMAG, which, as above, depended on the degree of disease severity. The most common histologic feature encountered was significant oxyntic gland/parietal cell loss with pyloric metaplasia (antralization of body or fundus oxyntic mucosa), followed by intestinal metaplasia with or without accompanying glandular atrophy and variable lymphoplasmacytic infiltration.
Interestingly, within the AMAG group, only 7 patients (9%) showed either concurrent HP infection or had previous biopsies showing HP infection. HP infection was not observed in association with any of the encountered low-grade B-cell lymphomas. In the overall study group, HP-associated gastritis was observed in 219 of 1692 patients (13%).
The early/incomplete pattern of AMAG,9,10 namely patchy oxyntic glandular destruction, parietal cell pseudohypertrophy/pseudopolyps, 20 and variable intestinal metaplasia, was observed in 17 patients (21.5%) with a median age of 50 years (range: 18–68). Self-identified demographics of the latter patients included: 16 Hispanic (17% of all female patients and 2% of all male patients) and 1 White patient (1.2% of all female patients).
Laboratory values prior to or after the diagnosis of AMAG were rendered were available for 69 of the 79 patients and demonstrated 13 of 69 (19%) with iron deficiency anemia, 22 of 69 (32%) with vitamin B12 deficiency, 15 of 69 with both vitamin B12 and iron deficiency (22%), and 19/69 with laboratory values within normal reference ranges (27%). No laboratory data were available for 10 of the 79 patients (12%).
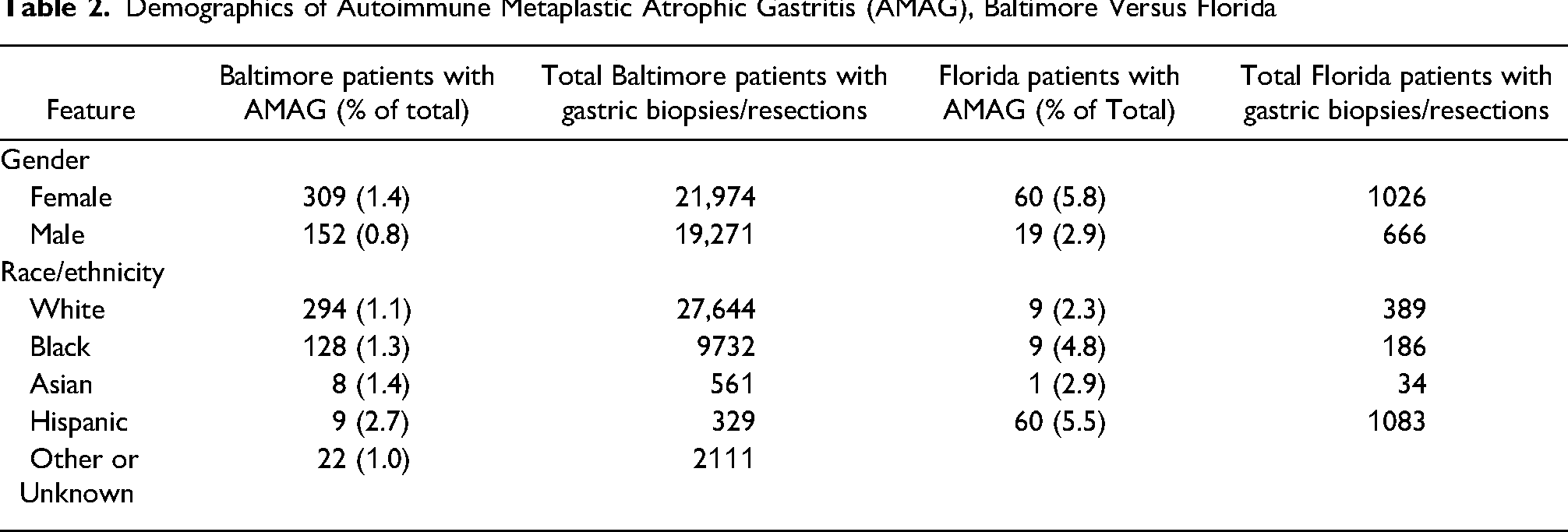
In our prior analysis of patients in Baltimore, 17 AMAG was diagnosed in 461 of 41,245 patients, accounting for 1.1% in a mostly White population (67%), but there were 9 AMAG patients among 329 patients who self-identified as “non-White-Hispanic”; a percentage of 2.7%. However, this difference did not reach statistical significance based on the limited number of self-identified Hispanics in the Baltimore area.
In our population in Florida, AMAG was diagnosed in 79 of 1692 patients (4.6%), a difference that reached statistical significance (p < .00001) when compared with the Baltimore data. In addition, the prevalence of AMAG among the Hispanic population is statistically significant from the prevalence in other ethnicities/races in our study.
The Baltimore study only included patients with fully developed AMAG (Figure 1A) and did not include patients with “early/incompletely atrophic AMAG” (Figure 2A). However, after removing the 17 “early AMAG” patients from the analysis, 62 out of 1692 (3.7%) Florida patients’ biopsies displayed fully developed AMAG, most of whom were Hispanic. This difference (1.1% vs 3.7%) also reached statistical significance (p < .00001).
A comparison between the Baltimore and the Florida findings is shown in Table 2.
Demographics of Autoimmune Metaplastic Atrophic Gastritis (AMAG), Baltimore Versus Florida
Discussion
AMAG is an immune-mediated form of chronic gastritis directed against oxyntic glands that results in loss of the parietal cell mass. The gastric corpus is, therefore, the site of disease.
We reviewed consecutive non-consultation gastric biopsies for AMAG and noted a higher prevalence of AMAG (4.6%) in our Florida population, which is heavily enriched for Hispanics compared to the previously studied population in Baltimore (1.1%). We chose to collect specimens prospectively and sequentially as AMAG had not been consistently diagnosed in archived samples in the Florida Hospital system, whereas it had in the Baltimore system. Self-identified demographics as recorded by the patients in our study included 60 (∼76.0%) Hispanic patients, 9 (∼11.4%) Black patients, 9 (∼11.4%) White patients, and 1 (1.2%) Asian patient.
Interestingly, Hispanics were diagnosed at younger ages than self-identified Blacks and Whites, a finding mirroring those in the Baltimore study. 17 The spectrum of disease severity varied from an early/evolving type of AMAG pattern to overt histologic manifestations of disease, including gland destruction/dropout, intestinal metaplasia, and variable basally oriented lymphoplasmacytic infiltrate of lamina propria. Endoscopically identifiable lesions, similar to those previously reported, were observed, including hyperplastic polyps, well-differentiated neuroendocrine neoplasms, adenocarcinomas, and lymphomas. In our study, we found background endoscopically identifiable lesions in 10 of 79 (13%) patients with AMAG. Also, similar to the findings in other studies, hyperplastic polyps were the most common lesions identified, 17 presumably secondary to chronic gastric injury. Since the current study included both patients with “early” AMAG and fully developed AMAG, not surprisingly, a lower percentage of patients in the current study had identifiable lesions than those in the Baltimore study (10 of 79, 13% vs 143 of 461, 31%).
Unfortunately, defining Hispanic can be difficult. The Meriam-Webster dictionary offers the following: “of, relating to, or being a person of Latin American descent and especially of Cuban, Mexican, or Puerto Rican origin living in the U.S.” (https://www.merriam-webster.com/dictionary/Hispanic). People meeting this description can have a variety of ancestries and appearances, and the current practice of the medical demographics of race/ethnicity is based on self-identification. Publicly available data for demographics of Florida indicate that the overall population is comprised of ∼70% self-identified Hispanics (https://statisticalatlas.com/county/Florida/Dade-County/Ancestry), and most also regard themselves as White (https://worldpopulationreview.com/us-cities/fl-population). The population of Baltimore consisted of 5% Hispanics in the 2010 US Census (https://www.census.gov/quickfacts/fact/table/baltimorecitymaryland,US/POP010210), close to the time when the AMAG data were collected by Park et al. 17
One possibility that was considered was the influence of our population's prevalent Helicobacter-pylori (HP) infection, which accounts for 13% of all gastric biopsies, on the prevalence of AMAG in our study. This is in contrast to the Baltimore study, which recorded a 7% HP infection rate in their evaluated gastric biopsies. 22 However, contrary to prior studies, which have suggested antigenic similarities and antibody crossover between HP infection and AMAG, mainly through the production of autoantibodies to parietal cell H+, K+, ATPase, 23 HP infection was only documented in 7 of our AMAG patients (9%). Thus, HP infection may not necessarily be an immunologic trigger to AMAG in the susceptible host. However, a limitation of this study is that HP antibodies, indicative of prior or current infection, were not examined in our AMAG population, whereas they were detected in 83% of patients with AMAG in 1 study. 24
In summary, although AMAG has traditionally been regarded as a disease of elderly White women of Northern European or Scandinavian descent, 15 the majority of affected patients in our population self-identified as Hispanic and we detected AMAG in 4.6% of our samples. Hispanic patients are the main population served by our institution, which has allowed us to review numerous gastric biopsies from this population. In a similar previous study, we found a prevalence among Hispanic patients of 2.7% in Baltimore, which did not reach statistical significance compared to the prevalence in Whites (1.1%) because of low numbers of Hispanic patients in the hospital catchment area. 17 Regardless, based on this study, this group of people (especially women) seems prone to developing autoimmune gastritis and physicians should be prepared to recognize it and treat it.
Conclusion
In conclusion, this study underscores the importance of recognition of AMAG in routine gastric biopsies as it may lead to iron deficiency early on (the high gastric pH impedes iron absorption), pernicious anemia over time, and the development of various gastric polyps and neoplasms. Our findings suggest that AMAG is more common in populations enriched for Hispanics compared to those enriched for Blacks or Whites. It is especially important for endoscopic colleagues to recognize this entity and perform adequate sampling of both oxyntic and antral mucosa in line with sampling protocols established years ago.21,25,26
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Approval from our Institutional Review Board was obtained to review clinical data (ID: 20201121).
Informed Consent
We prospectively analyzed samples. Patients are de-identified. Our Gastrointestinal Institutional Review Board number is listed above.
Trial Registration
Not applicable, because this article does not contain any clinical trials.