
Abstract
Angiomyofibroblastoma is a benign, usually small neoplasm typically constituted by spindle-shaped and epithelioid cells in a vascularized, myxoid-fibrous stromal background. It is most often seen in the superficial genitalia of female patients of reproductive age. However, various clinical and histologic features have been reported, including tumors in male patients, malignant transformation, extragenital sites, huge sizes, and a prominent lipomatous pattern. We report the clinical and pathologic features of one such tumor: a 23.5 cm lipomatous angiomyofibroblastoma of the vulva in a 40-year-old female patient. We also discuss important diagnostic considerations when approaching such large tumors, particularly in the setting of a biopsy specimen.
Introduction
Originally described 30 years ago, angiomyofibroblastoma is characterized as a small (usually <5 cm), benign soft tissue neoplasm in the superficial genitalia of female patients of reproductive age.1–3 Typically, angiomyofibroblastoma is a circumscribed, painless, slowly enlarging, subcutaneous mass in the external genitalia, which could be misinterpreted clinically as a Bartholin cyst or an inguinal hernia.4,5 Since its first description, there have been numerous studies and reports about this entity with other clinical and histologic features—their incidence in male patients, larger size, extragenital locations, and potential to contain a large amount of mature fat (originally referred to as a “lipomatous variant”)—thereby expanding the pathologic spectrum of the disease.3,4,6,7 Giant, lipomatous pattern angiomyofibroblastoma of the vulva is very rare and only one such tumor has been reported previously in literature. We herein report the second giant, lipomatous pattern angiomyofibroblastoma—this tumor arising in the vulva of a 40-year-old female patient—and provide a review of diagnostic considerations.
Report
A 40-year-old female patient with a history of obstructive sleep apnea, obesity hypoventilation syndrome, and Bartholin cyst presented with a chief complaint of one month of progressive left vulvar labial swelling and associated pain. Physical examination revealed a large, edematous, fluctuant, and non-erythematous left labia majora mass with normal mons pubis, introitus, vagina, right labia majora, and bilateral labia minora. An abdominopelvic CT showed a large labial lesion with associated inflammatory changes, potentially representing an infected labial cyst or a necrotic lipoma, among other diagnoses (Figure 1).

The patient presented with a large, protruding, edematous left labia majora mass with associated inflammatory changes on CT (A). The tumor measured 23.5 cm and was covered by thin, membranous tissue (B). Its cut surface was solid, soft, gelatinous, heterogeneous, and yellow-tan with scattered pink areas and firmer areas (C, after formalin fixation). No hemorrhage or necrosis was seen.
An open biopsy was performed and was consistent with angiomyofibroblastoma, lipomatous pattern. A month later, local excision of the vulvar mass was performed with intraoperative findings of a 21 cm, mobile, fibrous, and fatty mass in left labia majora extending to the mons pubis. Grossly the lesion consisted of a 23.5 × 16.4 × 5.4 cm, lobulated soft tissue specimen. The entire external surface was surrounded by white, thin, semitranslucent, membranous connective tissue. The specimen cut surface was solid, soft, gelatinous, heterogeneous, and yellow-tan with pink areas. Firmer nodular areas were appreciated within the mass. No hemorrhage or necrosis was seen (Figure 1).
Microscopic examination revealed an adipocyte-rich neoplasm with alternating cellular areas of loosely arranged spindle and plump epithelioid cells, organized in nests and cords or isolated around branching, thin, delicate, congested small vasculature. The neoplastic cells had scant cytoplasm and round or oval nuclei with homogeneous chromatin. No significant cytological atypia, mitoses, or necrosis were identified. The adipocytes were fully mature and no nuclear atypia or lipoblasts were seen. Focal areas with fewer adipocytes and looser fibromyxoid stroma were noted (Figure 2).

Microscopically, the tumor contained a rich background of adipose tissue, supporting the lipomatous subtype designation (A and B), within which classic features of myxoid stroma and mature fat could be seen (C). Thin, branching, and congested vasculature was present, surrounded by a condensation of tumor cells (D). The neoplastic cells showed both spindled and epithelioid morphology without significant atypia and were arranged in cords and nests (E and F). IHC testing for desmin showed a diffuse cytoplasmic staining pattern (G) while ER showed diffuse nuclear reactivity (H). IHC-based RB1 testing showed lack of staining in approximately 10% of nuclei distributed throughout the slide (I), and RB1 FISH testing showed no evidence of loss with two red RB1 signals present in every cell (J). [A-F H&E stain; A-B 50× original magnification, C-D 100× original magnification, E-I 400× original magnification]. IHC, immunohistochemical; FISH, fluorescence in situ hybridization.
By immunohistochemical (IHC) staining, the neoplastic spindle and epithelioid cells were strongly and diffusely positive for desmin and ER, weakly and focally positive for caldesmon and SMA, and negative for S100, CD34, ERG, and keratin AE1/3. ERG and CD34 highlighted the rich vascular component of the neoplasm. RB1 IHC showed a lack of nuclear expression in approximately 10% of tumor cells distributed throughout the tested section, and no gene deletion was detected by fluorescence in situ hybridization (FISH) (Table 1, Figure 2). Additionally, FISH for HMGA2 and MDM2 was negative for rearrangements and overexpression, respectively.
Summary of Clinical and Pathologic Features.
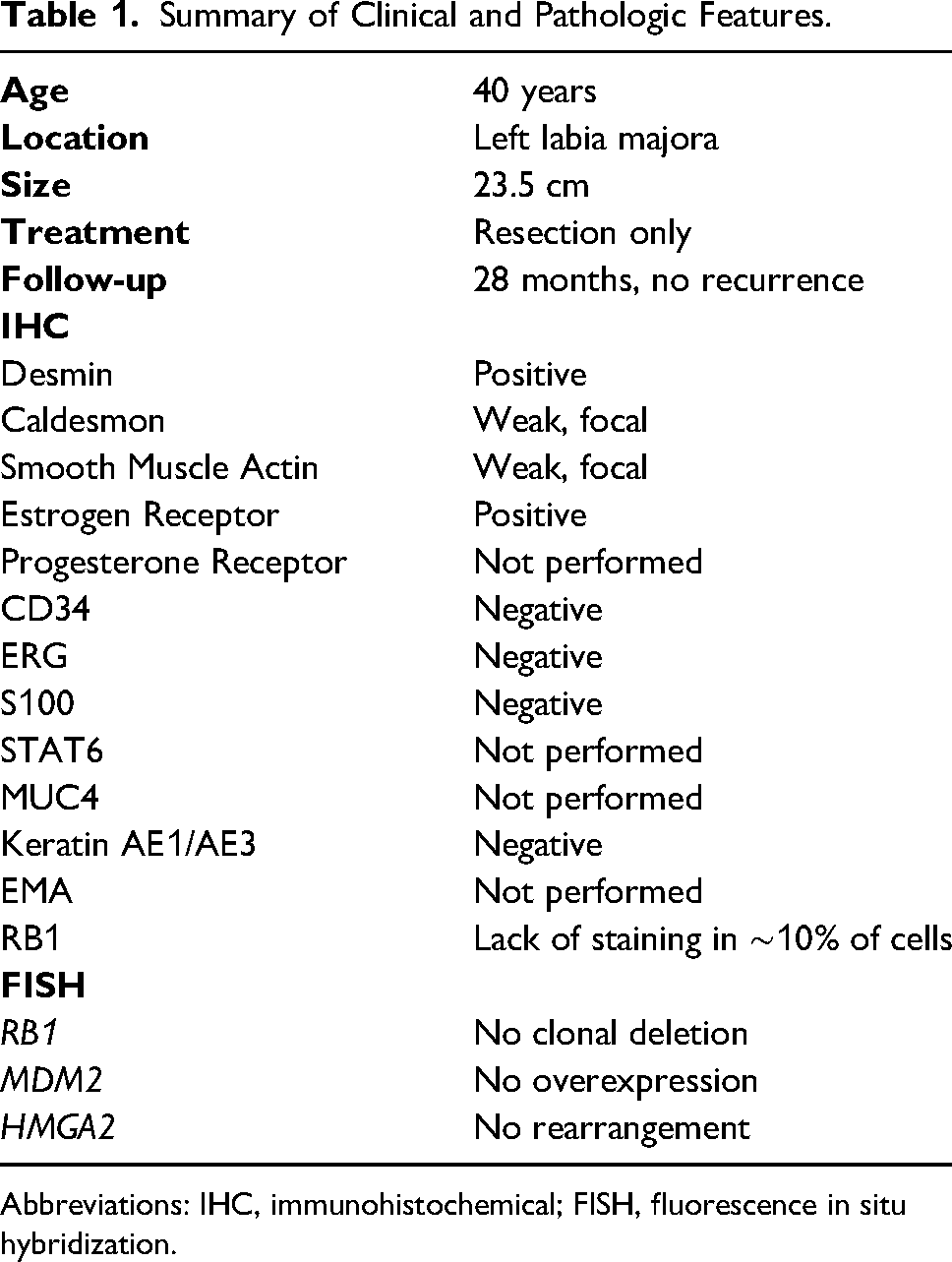
Abbreviations: IHC, immunohistochemical; FISH, fluorescence in situ hybridization.
Based on the clinical, morphologic, IHC, and FISH findings, a diagnosis of giant, lipomatous pattern angiomyofibroblastoma was confirmed. The patient received no additional therapy for the lesion and no evidence of disease 28 months after the surgery.
Discussion
Angiomyofibroblastoma is typically a benign, well-circumscribed myofibroblastic neoplasm, arising in the external genital region, originally described in 1992. 1 It arises principally in female patients with a wide age range between menarche and menopause. Few angiomyofibroblastomas have been reported in post-menopausal age, and no convincing angiomyofibroblastoma has been documented before puberty.5,8 Angiomyofibroblastomas in male patients are uncommon.6,7
Angiomyofibroblastomas are typically smaller than 5 cm and well-circumscribed clinically and grossly. Microscopically, it shows variable cellular areas of bland spindle to epithelioid tumor cells, frequently near a thin, delicate, and congested vasculature in a myxoid to fibrous stroma.1,2,4,9 Immunohistochemically, the tumor cells consistently express desmin, ER, PR, and BCL2 with retained RB1 expression; less frequently express CD34, SMA, CD10 and CD99; and do not express S100 or caldesmon.3,9–11 Immunoreactivity of each marker is rather nonspecific, but proper interpretation of a properly composed immunopanel could reveal the characteristic immunophenotype for the diagnosis.
Little was known about the oncogenic driver in angiomyofibroblastoma until a recent report of a novel MTG1::CYP2E1 fusion detected by reverse transcription-polymerase chain reaction in all 5 angiomyofibroblastomas and a subset of superficial myofibroblastomas tested, but not in angiomyxomas, cellular angiofibromas, fibroepithelial stromal polyps, and non-site-specific mesenchymal tumors occurring in the female lower genital tract. 12 A subsequent study has supported the finding of MTG1::CYP2E1 in vulvar angiomyofibroblastomas, indicating that detection of this fusion transcript may be useful for the diagnosis of angiomyofibroblastoma. 13
Fluorescence in situ hybridization or molecular assays for other molecular targets such as RB1 deletion, HMGA2 translocation, or MDM2 amplification can also help rule out entities in the differential diagnosis when testing for MTG1::CYP2E1 is not available. Loss of RB1 by immunostain or FISH raises the possibility of a RB1-deleted tumor, such as myofibroblastoma, cellular angiofibroma, or spindle cell lipoma. 14 Fluorescence in situ hybridization for detecting HMGA2 translocation could also be helpful when there is concerning for an aggressive angiomyxoma, particularly in such a large vulvar mass.3,15 Due to the amount the lipomatous element in lipomatous pattern angiomyofibroblastoma, FISH for MDM2 amplification is also helpful to rule out MDM2-amplified atypical lipomatous tumor or well-differentiated liposarcoma.
In general, the diagnosis can be made by clinical presentation (small size, well-circumscribed borders), histology, and immunophenotype (CD34, ER, desmin, SMA). The differential diagnosis includes cellular angiofibroma (angiofibroblastoma-like tumor of male genitalia), aggressive angiomyxoma, mammary-type myofibroblastoma, spindle cell lipoma, or other lipomatous tumors (in the setting of lipomatous pattern), all of which could have clinical, histological, and IHC overlap.3,9,16 The gross, microscopic, immunophenotypic, and molecular features of lipomatous pattern angiomyofibroblastoma and other stromal genital tumors of fibroblastic, myofibroblastic, and adipose tumors with overlapping characteristics are summarized in Table 2.
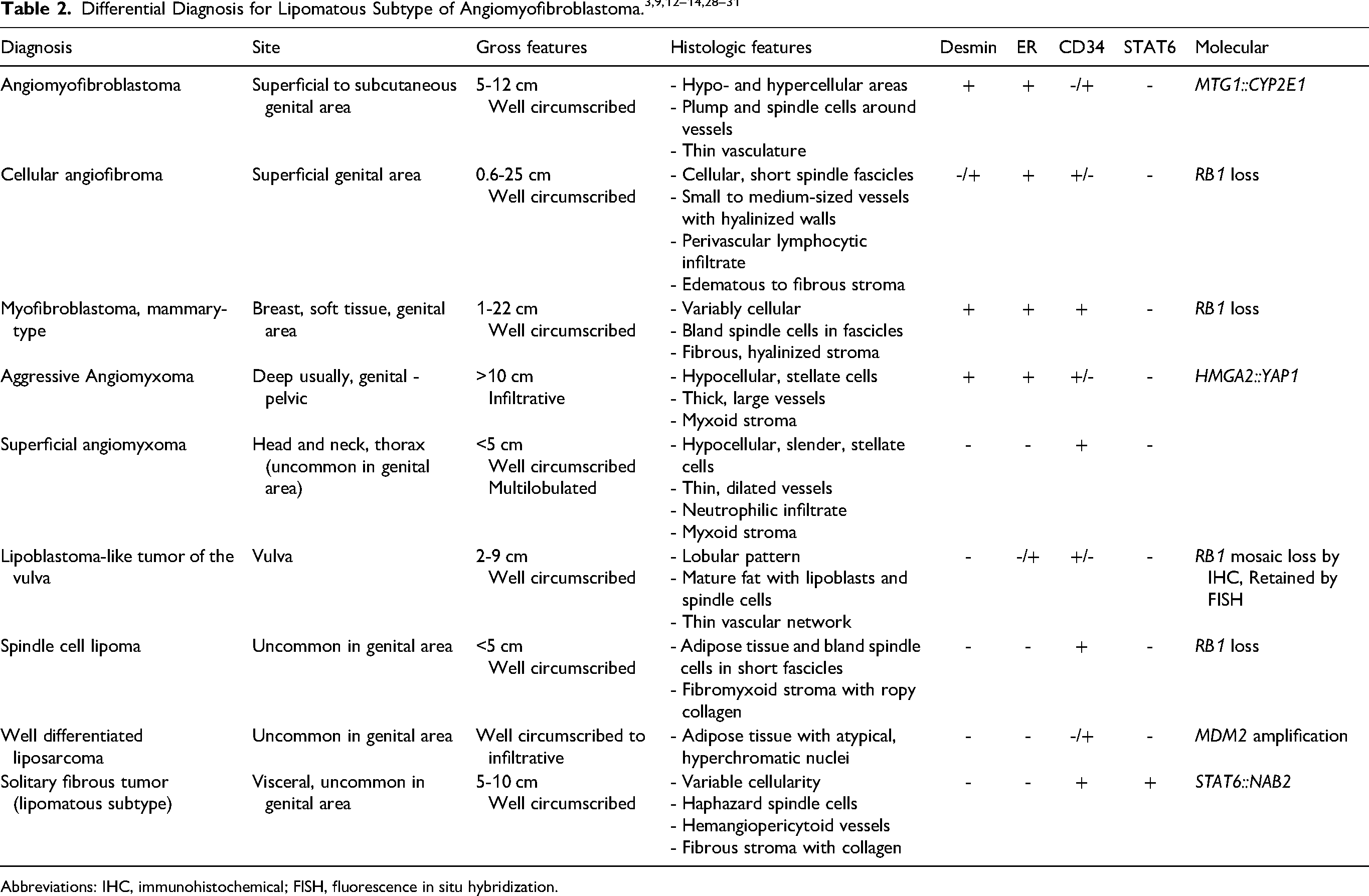
Abbreviations: IHC, immunohistochemical; FISH, fluorescence in situ hybridization.
Variable amounts of adipocytic tissue have been reported in 10% of reported angiomyofibroblastomas, ranging from small foci of mature fat that usually did not hinder diagnosis to extensive fat presence that accounted for 90% of the tumor total volume. The lipomatous pattern was originally termed a “lipomatous variant” by Laskin et al4,17 Although there is no concurrence on the threshold, Luis et al suggested to reserve this terminology for tumors where mature adipose tissue predominates and accounts for over 50% of the tumoral tissue. 17 With such a definition, lipomatous pattern is a very rare, and no more than twenty such tumors have been reported in literature. 18
For angiomyofibroblastoma, the size is usually less than 5 cm with the range of size reported between 1.1 and 12 cm, but there have been well-documented examples larger than 12 cm.3,5,19,20 Upon review of the English medical literature, three huge or giant angiomyofibroblastomas arising in the subcutaneous vulvar region have been reported, measuring 19, 23 and 37.5 cm.19,21 The third tumor was also a lipomatous pattern angiomyofibroblastoma in a 44-year-old woman with a 37.5 cm mass in the subcutaneous tissue left labium of the vulva, reported by Nabaei et al 18 In addition to female external genitalia, large angiomyofibroblastoma ranging 17 cm to 34 cm were also reported in nearby regions such as the pelvis and retroperitoneum as well as the perineum and paratesticular region of male patients.3,20,22–24
While it is uncommon for angiomyofibroblastoma to grow >20 cm, giant angiomyofibroblastoma with a prominent lipomatous element is even less common with only one such tumor previously reported. 18 Due to its unusual large size and lipomatous morphology, making the diagnosis could be challenging, particularly in a small core biopsy that may consist predominantly of fatty tissue. Careful evaluation of subtle histologic features, proper use and interpretation of an IHC panel and FISH assays, and correlation with clinical and radiographic presentation are crucial for making the correct diagnosis.
Angiomyofibroblastomas are benign tumors with an excellent prognosis. Recurrence is uncommon after complete excision. There are rare reports of “malignant” angiomyofibroblastoma with nuclear atypia and increased mitotic activity, one of which recurred locally after 2 years, but none with metastasis.25,26 For those lipomatous tumors with follow-up, there was no evidence of malignant transformation or a difference in prognosis.10,27 Similarly, for giant tumors with follow-up, no recurrence or metastasis has been reported for patients treated with simple excision.19–23
Conclusion
We report a second giant lipomatous angiomyofibroblastoma in the vulva of a 40-year-old female patient. It is important to recognize this unusual large-size presentation of a rare entity particularly in core biopsy of a large fatty tumor in the region because there is differential diagnosis of other benign and malignant tumors in the region with overlapping features. The diagnosis is based on the clinical and histologic and IHC features assisted with molecular tests when difficulty arises in histologic and IHC evaluation of a larger lesion with unusual histologic features. In addition to its typical presentation and histology, one should be aware of its capacity for unusually large size, extra-gynecologic site presentation, and lipomatous morphology, particularly in small core biopsies before surgical intervention.
Footnotes
Acknowledgments
The authors would like to thank Carlos Cotallo Solares for his assistance in creating the figures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.