
Abstract
In the recent literature soft tissue neoplasms which harbor a recurrent YAP1::MAML2 fusion and have an epithelioid morphology with resemblance to myxoinflammatory fibroblastic sarcoma (MIFS) have been reported. In a recent series these tumors had a nodular appearance and central necrosis and were termed nodular necrotizing variants of MIFS. But their exact relationship to MIFS and their biological behavior seem to be unclear. We report a YAP1::MAML2 fusion positive nodular and necrotizing tumor with a MIFS-like morphology and provide a review of the literature.
Introduction
Recently, soft tissue neoplasms with recurrent YAP1::MAML2-fusions and epithelioid morphology resembling myxoinflammatory fibroblastic sarcoma (MIFS) have been reported.1,2 They share many features with MIFS, but there are also distinct differences. MIFS are known to have a predilection for the distal extremities, 3 while the reported YAP1::MAML2 fusion positive tumors had a wider anatomical distribution, occurring frequently at non-acral sites.1,2 MIFS present as infiltrative, rarely necrotic tumors composed of spindle and epithelioid cells, located in the superficial subcutaneous tissue, in a fibrous to myxoid stroma, admixed with a prominent inflammatory infiltrate. 4 The molecular landscape of MIFS is heterogeneous with three molecular alterations known to date: VGLL3 amplification (most common alteration), BRAF fusion/amplification, 2-OGA (MGEA5), and/or TGFBR3 rearrangements.3,5–7 In contrast, the YAP1::MAML2 fusion positive (3/7) MIFS-like tumors reported by Perret et al 1 presented as single, solid nodules with central necrosis, composed predominantly of epithelioid, virocyte-like cells with absent myxoid stroma. Clinically, they demonstrated a benign behavior. Dermawan et al 2 reported six epithelioid neoplasms with MAM2-gene rearrangements, three of which had YAP1::MAML2-fusions and resembled the MIFS-like tumors described by Perret et al 1 except that they lacked a nodular configuration, and one of the patients developed lung metastasis. Thus, the clinical behavior of YAP1::MAML2-rearranged epithelioid MIFS-like neoplasms and their pathogenetic relationship to MIFS seems to be unclear.
We report a YAP1::MAML2 fusion positive tumor in an acral position with MIFS-like morphology, a nodular appearance, necrosis, and a favorable course of disease.
Case Report
A 40-year-old man presented to the emergency department with progressive pain and swelling of the right thumb. First, he was treated conservatively for clinically suspected tenosynovitis. On his reentry, an excisional biopsy of the approximately 1.5 cm large mass was performed without pre-operative imaging. Histology of the excisional biopsy showed a solid mass, which—as far as could be assessed after intralesional excision—had a nodular appearance and areas of necrosis (Figure 1a-c). By microscopy, there was a predominance of large, plump, epithelioid, virocyte-like cells with eosinophilic, glassy cytoplasm, vesicular nuclei, and prominent nucleoli (Figure 2). The tumor cells were intermixed with a polymorphous inflammatory infiltrate consisting of lymphocytes, plasma cells, neutrophils, and eosinophils, embedded in a fibrous, non-myxoid stroma (Figure 1d). The mitotic rate was low. Ziehl-Neelson stain did not reveal any pathogen. The virocyte-like tumor cells expressed CD68, partially CD34 and were single-cell positive for keratin (AE1-AE3) (Figure 3). They expressed CD10 (MME), Cyclin D1, and Factor XIIIa, while D2-40 was negative (Figure 4). INI1 was retained (Figure 3). S100, SOX10, alpha smooth muscle actin, desmin, ERG, and ALK were negative, as were CD45, CD20, CD3 and myeloperoxidase (positive in the inflammatory infiltrate, Figure 3); CD30 was negative in the virocyte-like/Reed-Sternberg-like cells. Next-generation sequencing (NGS Archer FusionPlex Panel V2) detected a fusion transcript YAP1 (Exon 4)::MAML2 (Exon2).

(a) Low-power magnification of the tumor shows a nodular silhouette, (b, c) at higher power necrotic areas with leukocytoclasia are seen, and (d) a predominance of virocyte-like cells intermixed with inflammatory cells without myxoid stromal changes.

(a-d) The tumor cells range from histiocytoid to large, plump, epithelioid cells with glassy, eosinophilic cytoplasm, large, vesicular nuclei and prominent nucleoli (virocyte-like cells). The tumor stroma consists of collagen bundles; the collagen fibrers are occasionally arranged around the tumor cells; there are no significant myxoid stromal changes. (c) Mumified tumor cells with condensed, deeply eosinophilic cytomplasm are highlighted (arrows).

The tumor cells expressed CD68, CD34 and were single-cell positive for keratin (AE1-AE3). INI1 was retained. Myeloperoxidase (MPOX) highlights the necrotic areas and CD3 the admixed inflammatory infiltrate.

The tumor cells expressed CD10 (MME), Cyclin D1, and Factor XIIIa, while D2-40 was negative.
A complete exision of the lesion was performed with negative margins, and the patient is well without evidence of disease after 7 months.
Discussion
MIFS usually occurs in an acral location as an infiltrative mass with a tendency of local recurrence and rare distant spread. 3 In classic cases, necrosis is rare and focal. 4 Immunhistochemistry has a limited role in the diagnosis, 7 and the molecular landscape of MIFS is known to be heterogeneous with VGLL3 amplification being the most consistent finding. 7 Recently, tumors with morphological similarities to MIFS, but with a distinct molecular profile of YAP1::MAML2 fusion have been described by Perret et al 1 (seven tumors) and Dermawan et al 2 (three such tumors) (Table 1). The seven tumors reported by Perret et al 1 had a common histopathological phenotype and YAP1::MAML2-fusions (found in 3/7 tumors) (no. 2, 5, 7; Table 1). All manifested as a single, solid nodule with central necrosis, composed predominantly of large, epithelioid, virocyte-like cells with few or absent spindle cells, absence of pseudolipoblasts, and lack of myxoid stroma. The term « nodular necrotizing variant of MIFS » for these tumors was proposed by Perret et al, 1 but their exact pathogenetic relationship to MIFS seems to be unclear. MIFS are known to harbor rearrangments of TGFBR3 and 2-OGA (MGEA5), amplification of VGLL3 and BRAF rearrangments. VGLL3 amplification, tested in one tumor of the series, was not detected; however, another tumor of the cohort showed an additional BRAF rearrangement (no. 7; Table 1)—a potential link with BRAF-rearranged MIFS. While MIFS form infiltrative masses and mainly occur in the subcutaneous tissue of the acral extremities (hands and fingers), the tumors described by Perret et al 1 were well-circumscribed. They occurred not exclusively at acral sites. In fact, most tumors were located at non-acral sites (5/7, 71%), and only two were situated in acral positions. The tumors tended to be smaller than classic MIFS (mean size 20 mm vs 32 and 42 mm),3,5 and all tumors showed a benign clinical behavior with follow-up periods ranging from 7 to 63 months. The morphology and immunhistochemical phenotype were similar to classic MIFS (YAP1 immunostaining was negative in 6/6 analyzed tumors in the study by Perret et al 1 and positive in one of three tumors with YAP1::MAML2-rearrangements reported by Dermawan et al 2 ).
Clinicopathological Features of the Reported Epithelioid Neoplasms with MAML2-Rearrangements.
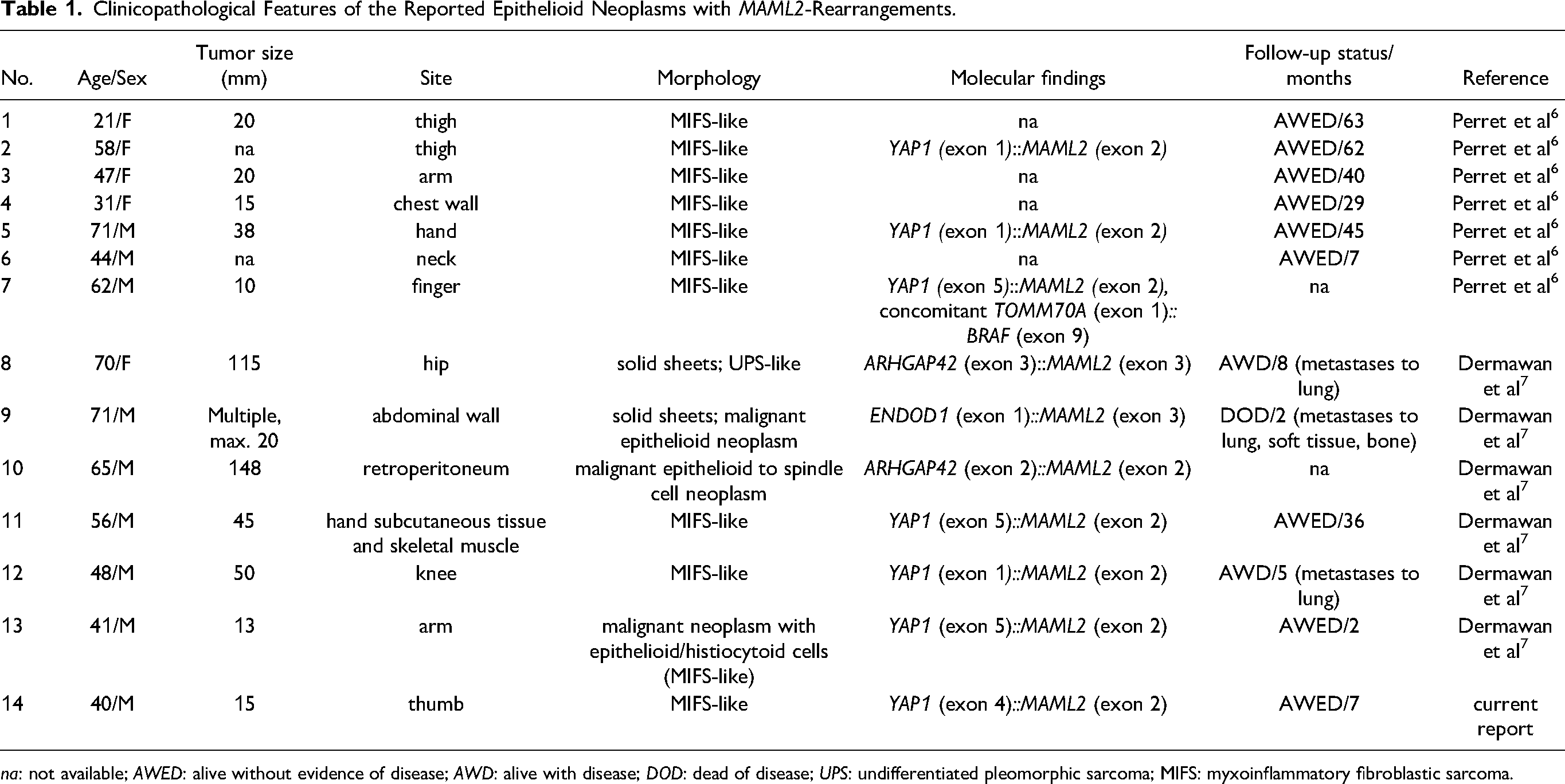
na: not available; AWED: alive without evidence of disease; AWD: alive with disease; DOD: dead of disease; UPS: undifferentiated pleomorphic sarcoma; MIFS: myxoinflammatory fibroblastic sarcoma.
Dermawan et al 2 reported six MAML2-rearranged undifferentiated malignant neoplasms with epithelioid morphology and MAML2-gene fusions arising in the deep soft tissue. The fusion partners of MAML2 were YAP1 (n = 3), ARHGAP42 (n = 2), and ENDOD1 (n = 1). Microscopically, all tumors had an epithelioid morphology, prominent mitotic acitivity, (focal or extensive) necrosis, and an infiltrative growth pattern. Three of these MAML2-rearranged tumors harbored YAP1::MAML2-rearrangements and had morphological similarities to MIFS (no. 11-13 ; Table 1), but—different than the tumors described by Perret et al 1 —they were not well-circumscribed or nodular. Only one tumor occurred in an acral position, the other two were located at extra-acral sites. Notably, one tumor showed an aggressive clinical behavior (metastases to lung), while the other two had a favorable course of disease. One of these YAP1::MAML2-rearranged tumors, located in an acral location (hand) and associated with a benign course of disease, resembled most the tumors reported by Perret et al, 1 despite the lack of a nodular tumor configuration (no. 11 ; Table 1).
Following these observations, the biological potential of YAP1::MAML2-rearranged tumors seems to be not fully understood to date, and larger cohort studies with long periode follow-ups would be needed to determine their exact biological potential. MIFS are known to harbor rearrangments of TGFBR3 and MGEA5, amplification of VGLL3 and BRAF rearrangments. The genetic heterogeneity of MIFS raises the question of whether MAML2-rearranged tumors should be grouped under the same umbrella term of MIFS. Future investigations for the pathogenetic relationship between MAML2-rearranged tumors and MIFS are required including transcriptional and epigenetic plattforms.
Although three cases of the cohort reported by Dermawan et al 2 had overlapping features with MIFS, the remaining three tumors with MAML2-rearrangements (but different fusion partners than YAP1) did not demonstrate histological or clinical features of MIFS. In all except one case, the tumors were located in non-acral locations, and three of all tumors showed an aggressive behavior.
MAML2-fusions have been described also in other, morphologically distinct entities, including rare cases of retiform and composite hemangioendothelioma with neuroendocrine differentiation. 8 MAML2-rearrangements have been reported in metaplastic thymomas (YAP1::MAML2), 9 in poromas/porocarcinomas (YAP1::MAML2) 10 and spindle cell/sclerosing rhabdomyosarcoma, 11 but these entities have specific discriminative clinicopathologic features. Entities, that can be considered in the differential diagnosis of MIFS, include pleomorphic sarcoma, superficial CD34-positive fibroblastic tumor (but many harbor PRDM10-rearrangements), 12 and Hodgkin lymphoma (exclusive cutaneous presentation of Hodgkin lymphoma is rare, and MIFS are negative for CD30 and CD15). 13
In conclusion, the pathogenetic relationship of epithelioid neoplasms with YAP1::MAML2 rearrangement with the family of MIFS remains unclear, given the low frequency of acral presentation and of VGLL3 upregulation/amplification as well as the reported distant metastases. Further clinicopathologic studies with molecular correlates would be needed to determine, if MAML2-gene rearrangments define a heterogeneous group of tumors or merely a wide morphologic spectrum of a single pathologic entity of soft tissue sarcomas with epithelioid phenotype.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because the article does not contain any studies with human or animal subjects.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Trial Registration
Not applicable, because the article does not contain any clinical trials.