
Abstract
Histiocytic sarcoma is a malignant neoplasm with cells showing morphologic and immunohistochemical features of histiocytes. The lung and stomach are rare sites of involvement, and few have been reported in the existing literature. We report a 72-year-old woman with primary histiocytic sarcoma involving the right lung, stomach, and bilateral adrenal glands. Computed tomography revealed a large heterogeneous mass in the upper lobe of the right lung, regional lymphadenopathy, and masses within the bilateral adrenal glands. Gastric involvement was discovered via polypectomy during a routine gastric endoscopy. Morphologically, the lung and stomach specimens showed sheets of large and spindle cells with increased mitotic figures. Immunohistochemical staining revealed CD163, CD68, and CD4 expression in the lung tumor and CD163 and CD4 in the gastric tumor. The patient deteriorated rapidly and died of a pulmonary infection two months after diagnosis. Surgical resection remains the most effective treatment. However, for those with advanced disease, systemic chemotherapy alone may be the only available option, but the outcomes are variable. Advancements in targeted therapy are needed to improve treatment outcomes for patients with multi-organ involvement of histiocytic sarcoma.
Introduction
Histiocytic sarcoma is a malignant neoplasm with cells showing morphologic and immunohistochemical features of histiocytes. 1 Histiocytic sarcoma can be a primary disease or associated with certain hematopoietic malignancies. 2 Patients commonly present with advanced disease due to early indolent course and non-specific presenting symptoms. It is an aggressive disease with a poor prognosis when discovered at an advanced stage. Histiocytic sarcoma most commonly affects the skin, connective tissue, lymphatic, and gastrointestinal tract. However, gastric involvement and pulmonary involvement of primary histiocytic sarcoma rarely occur. To our knowledge, only a handful has been reported. Radiological findings of pulmonary involvement are often non-specific, which results in a reliance on histological and immunohistochemical methods for diagnosis. In this article, we report a patient with a rare, advanced primary histiocytic sarcoma with pulmonary, gastric, and adrenal involvement with a review of published literature.
Patient Presentation
A 72-year-old woman presented with mild dyspnea on exertion for several months. Her medical history includes rheumatoid arthritis, peptic ulcer disease, osteoporosis, chronic hepatitis C infection, and hypertension, all of which are medicated and under regular follow-up at our subspecialty outpatient clinics. An initial chest x-ray revealed nodular opacities in the upper lobe of her right lung. Subsequent computed tomography (CT) of the chest demonstrated a 3.35 cm mass in the right upper lobe with an invasion of the visceral pleura and mediastinal pleura, with suspected involvement of the ipsilateral peribronchial, hilar, and intrapulmonary lymph nodes and suspected distal metastasis to the bilateral adrenal glands (Figure 1A and B). CT-guided biopsy of the right upper lobe pulmonary mass was performed.
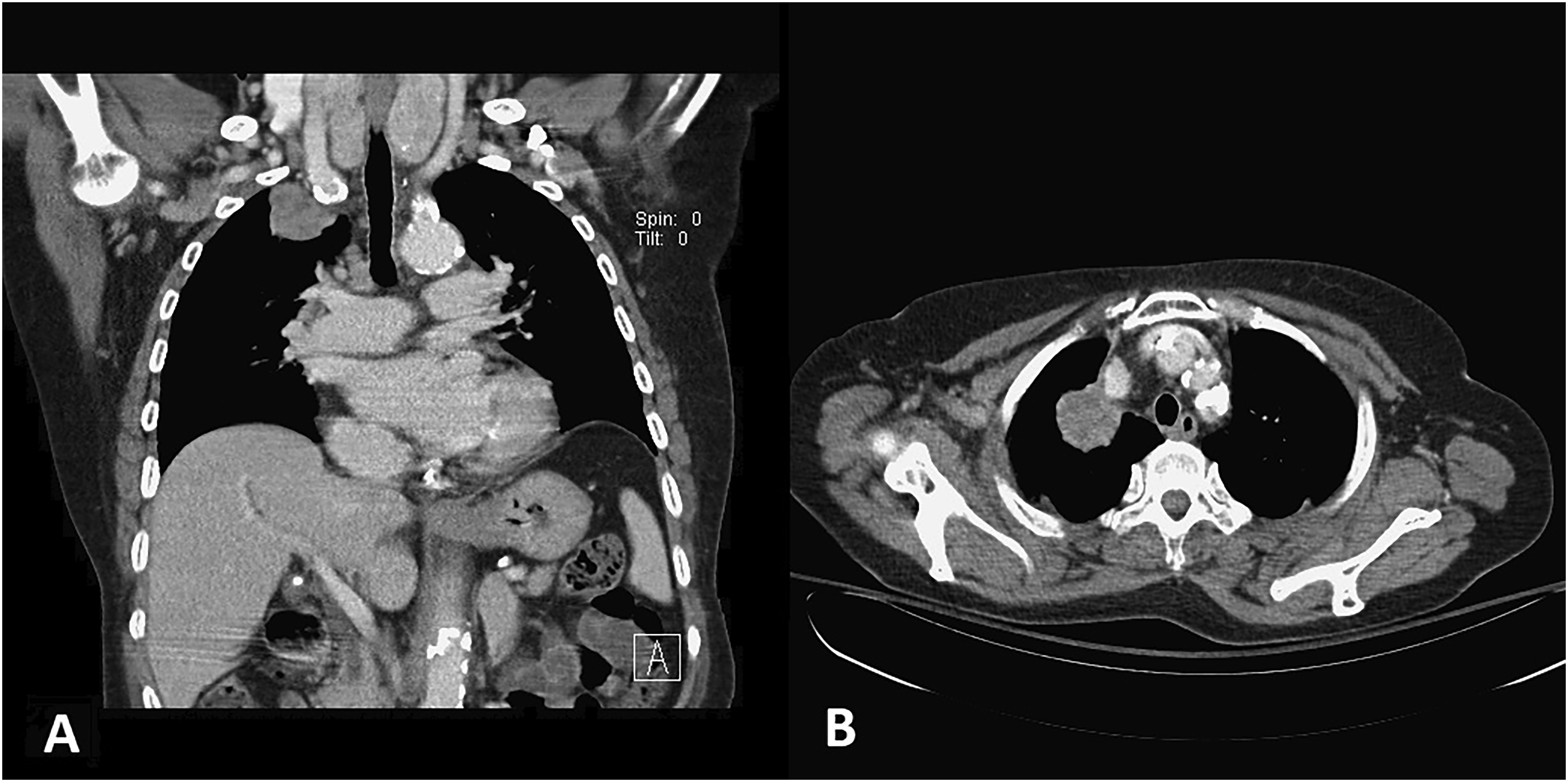
Coronal (A) and axial (B) thoracic contrast-enhanced computed tomography demonstrated a soft tissue mass located in the apex of the right lung, lateral to the superior vena cava.
Microscopically, the biopsied tissue demonstrated sheets of large spindle cells with increased mitotic figures associated with dilated blood vessels and focal necrosis. Immunohistochemically, these cells were positive for vimentin, CD4, and CD163. Cells with positive CD68 (Figure 2C) and lysozyme were found focally. Stains for keratin AE1/3, CD34, STAT6, SMA, S100, TTF1, EMA, HMB45, inhibin, synaptophysin, chromogranin, SOX10, beta-catenin, CD21, CD35, ALK, CAM5.2, HepPar1, CD1a, CD45, MPO, CD56, and CD123 were negative. The patient was then diagnosed with progressive multifocal histiocytic neoplasm with lungs as the suspected origin.
Incidentally, two 1.2 cm polyps on the gastric body were found during an esophagogastroduodenoscopy performed as a regular follow-up for her peptic ulcer disease. Biopsy revealed a background of mixed inflammatory cell infiltration with atypical epithelioid and spindle cells with pleomorphic nuclei, prominent nuclei, and irregular nuclear membranes infiltrating and replacing gastric mucosa (Figure 2D and E). Immunohistochemistry revealed positive staining for CD163 (Figure 2F) and CD4 and negative staining for CD68, KIT, DOG1, keratin AE1/3, S100, LCA and lysozyme. The morphology of the stomach neoplasm was compatible with that of the lung mass. The diagnosis of histiocytic sarcoma with pulmonary, gastric, and adrenal involvement was made. After a thorough explanation of her prognosis and different treatment options, the patient and her family decided to accept home hospice due to a poor projected prognosis. She passed two months after the diagnosis due to a pulmonary infection.

Tissue sections of the lung tumor showed a population of plump to spindle cells in a sheet pattern associated with some dilated vessels, necrosis, and mitoses (A, 100 ×; B, 400 ×). Malignant cells showed focal positivity for CD68 (C, 400 ×). Sections of the gastric polyps showed replacement of gastric mucosa by atypical epithelioid and spindle cells infiltrated with mixed inflammatory cell infiltration (D, 100 ×; E, 400 ×) and had intense staining for CD163 (F, 400 ×).
Discussion
Histiocytic sarcoma is a rare histiocyte neoplasm first described in 1972. 3 It makes up less than 1% of all hematopoietic malignancies. 4 Previously classified as a non-Langerhans histiocytic malignant neoplasm of monocyte-macrophage origin, based on a 2002 study of 61patients, histiocytic sarcoma is currently classified under histiocytic and dendritic cell neoplasms according to the World Health Organization classification criteria revised in 2016.5,6 Histiocytic sarcomas may develop as a de novo or in association with synchronous or metachronous lymphomas, commonly follicular lymphoma, lymphoid leukemias, and myeloid leukemias. In some rare instances, especially in young adults, mediastinal histiocytic sarcoma has been found in association with non-seminomatous germ cell tumors. 7 Furthermore, those that are thought to be transdifferentiated from hematopoietic malignancies and those associated with germ cell tumors retain the same genetic profile as their associated malignancies.2,8,9 In our patient, the neoplasm likely occurred de novo as the patient had no history of hematopoietic or germ cell neoplasms.
Histiocytic sarcoma can affect a wide age range, with reported occurrences in infants, adults, and the elderly. The median age of occurrence is usually in the sixth and seventh decades of life.10–12 Studying its epidemiological features remains challenging due to its inherent rarity. Kommalapati et al performed two of the largest population studies to date by pooling diagnosed instances of histiocytic sarcoma from two national databases, Patients, Surveillance, Epidemiology, and End Results (SEER) and National Cancer Database (NCDB).11,12 The study using 159 patients from SEER produced an estimated incidence of 0.17/million. 11 As for the site of occurrence, histiocytic sarcoma favors extranodal sites, especially in the skin and connective tissue and the gastrointestinal tract. 1 While primary histiocytic sarcoma involving the gastrointestinal tract represents a sizable portion of the reported instances, the disease rarely occurs in the stomach. Only a handful of tumors with gastric involvement have been reported. An extensive literature search on Pubmed found only 9 patients, with 6 above age 60.13,14 In the geriatric patients, 3 had lesions beyond the stomach. One had colon involvement and distal metastasis to the sternum; another had two distinct masses in the stomach and metastatic lesions in the spleen and intra-abdominal lymph nodes; the last patient had lymph nodes and small intestines metastasis. For primary histiocytic sarcoma with lung involvement, a literature search on Pubmed yielded 9 patients, all men (Tables 1 and 2).10,15–22 While male preference is evident in the published reports of primary pulmonary histiocytic sarcoma, it remains controversial since studies have produced contradicting results. The proportion of elderly patients was lower when compared with the overall trend, with only 3 above the age of 60 and 4 below the age of 40. Involvement of tissue other than the lungs was only seen in older patients. To the best of our knowledge, this is the first reported example of histiocytic sarcoma with simultaneous involvement of the lungs, stomach, and bilateral adrenal glands.
Characteristics of Reported Histiocytic Sarcomas Involving the Lungs.
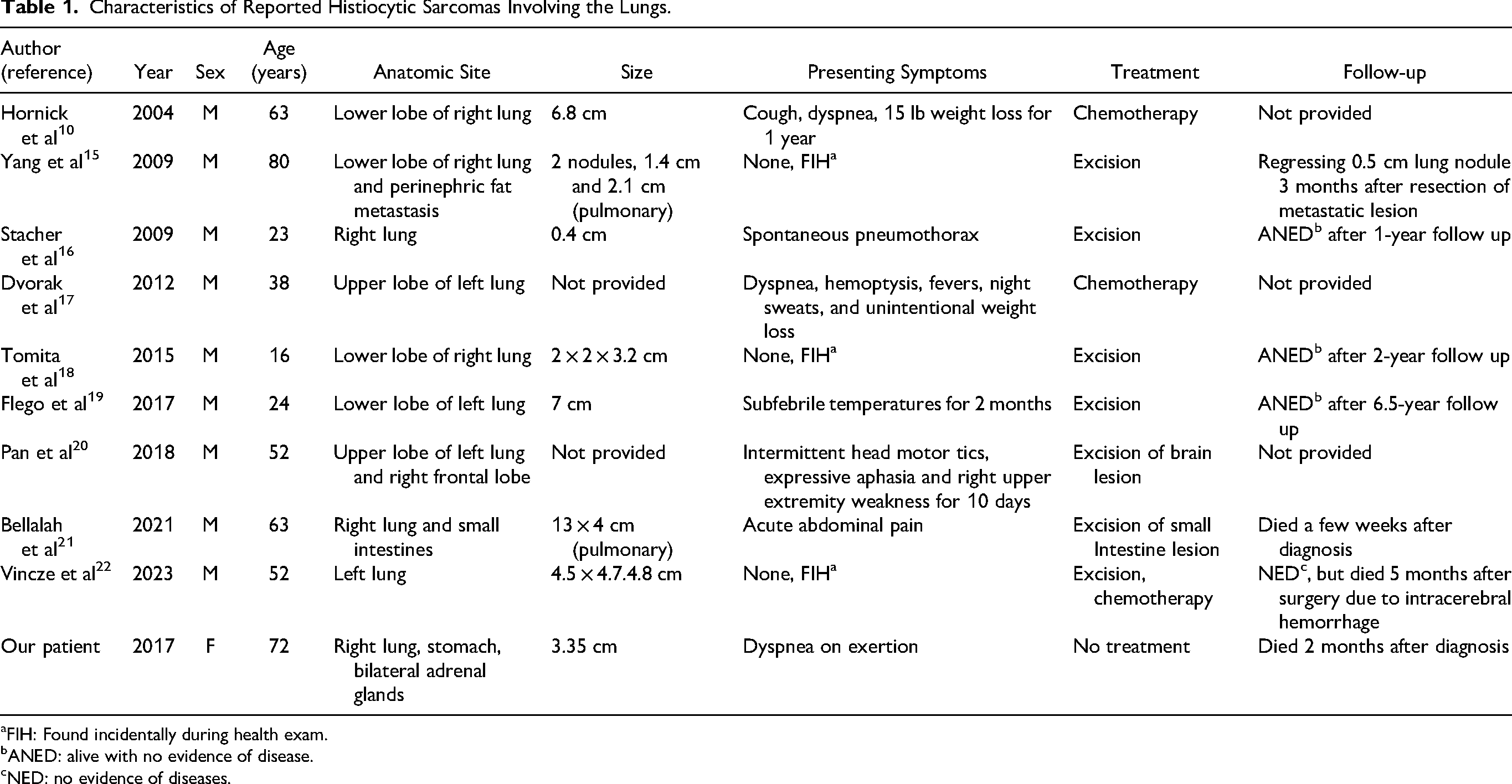
aFIH: Found incidentally during health exam. bANED: alive with no evidence of disease. cNED: no evidence of diseases.
Histomorphological and Immunohistochemical Characteristics of Reported Histiocytic Sarcomas Involving the Lungs.
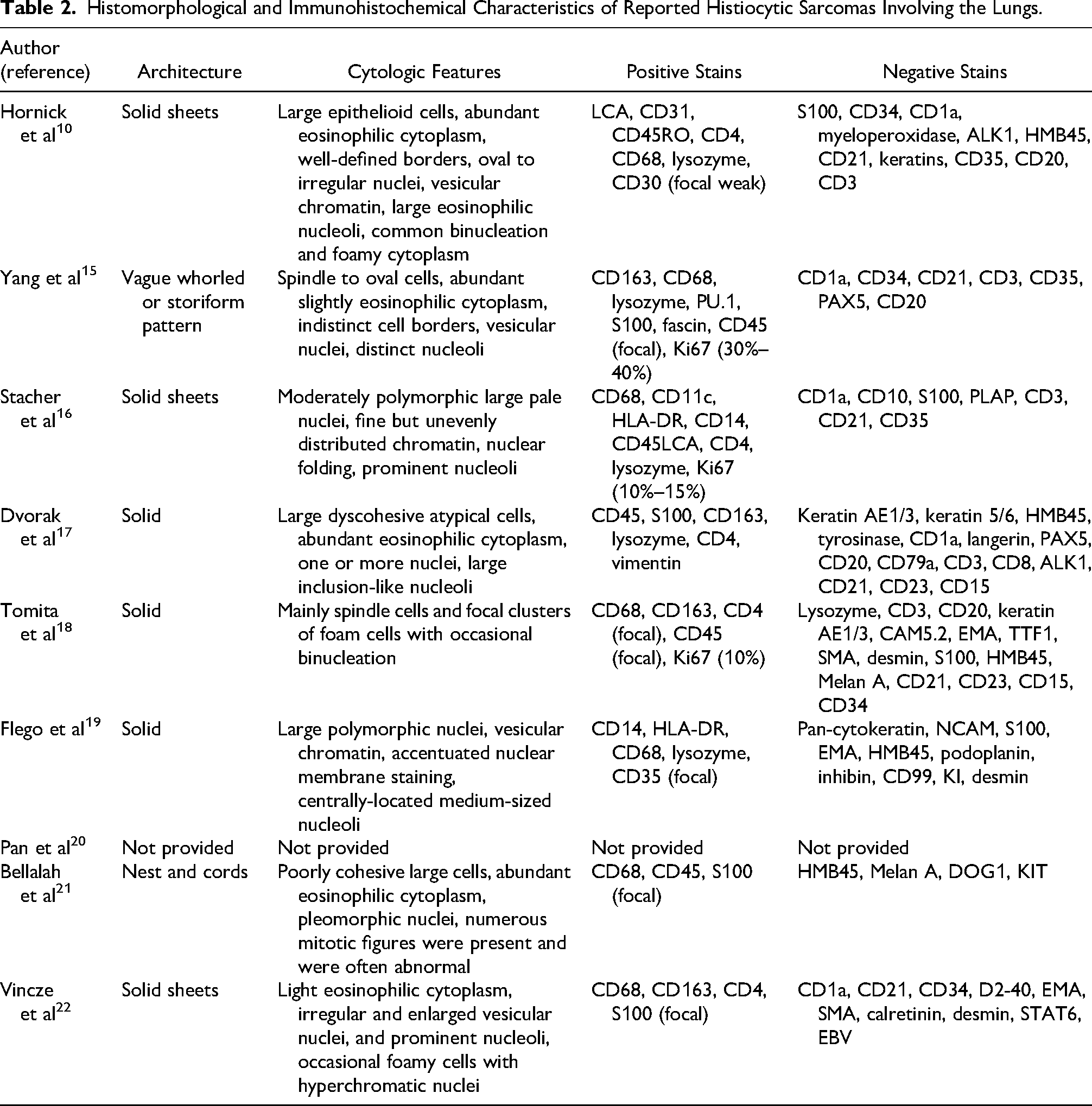
a-/+: immunohistochemical marker can be either present or absent.
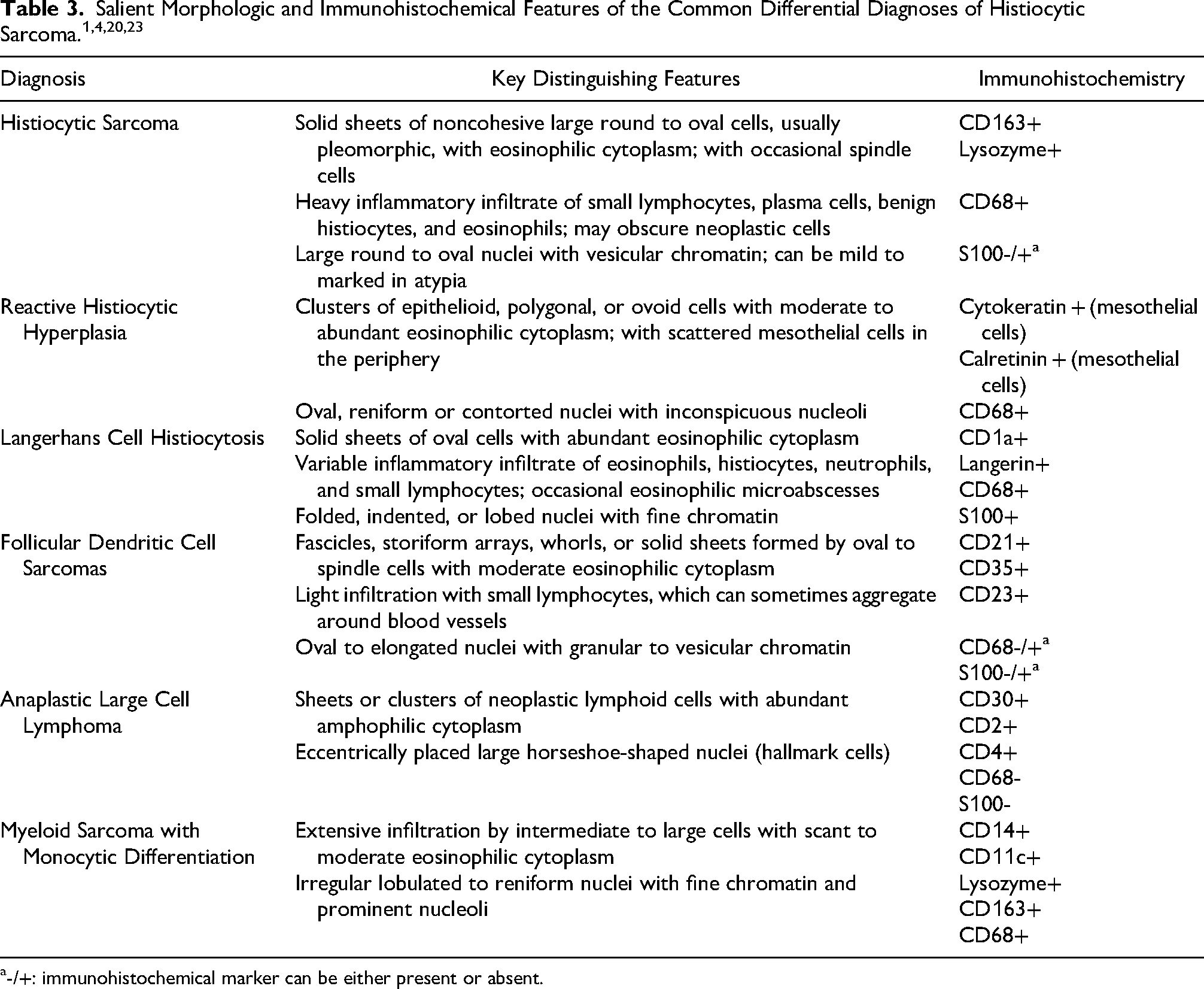
Morphologically, histiocytic sarcoma often presents as diffused noncohesive proliferation of polygonal large cells. These cells commonly have abundant eosinophilic cytoplasm and prominent nuclei with vesicular chromatin. Typical findings include cellular pleomorphism, hemophagocytosis, and mild to heavy infiltration of benign inflammatory cells. Immunohistochemically, neoplastic cells often stain positive for histiocytic markers, such as CD163, CD68, and lysozyme. They are negative for CD1a, langerin, CD21, and myeloperoxidase, differentiating histiocytic sarcoma with neoplasms and benign entities of the Langerhans cell, follicular dendritic cell, and other myeloid cell lineages (Table 3). 23 Histiocytic sarcoma cells also commonly express of HLA-DR, CD45, CD31, CD45RO, and CD4. Variable expression of CD15 and S100 can be seen in some tumors. Ki67 proliferation index is often variable. These features are present in the reported primary disease involving the stomach and lungs, including our patient. Due to its rarity, final diagnosis is often preceded by excluding more common tumors of the affected organ. In our patient, the multi-organ nature necessitated a more extensive initial repertoire of differential diagnoses, such as the more common epithelial, soft tissue, and hematopoietic tumors of the lungs. Metastatic melanomas, metastatic hepatocellular carcinoma, and anaplastic large cell lymphomas were also ruled out. Finally, other lineages of myeloid sarcomas were excluded. The gastric lesions were discovered incidentally after the diagnosis of the pulmonary lesion was made. While there were morphological and immunohistochemical similarities between tissue sampled from both sites, a gastrointestinal stromal tumor had to be excluded due to shared morphological features.
Radiological features were included in all reported primary pulmonary histiocytic sarcomas. The tumor usually appears as an infiltrative solid mass with or without apparent central necrosis on CT images. On the other hand, Tomita et al reported pulmonary histiocytic sarcoma with well-defined and non-infiltrative patterns. The non-specific and varied radiographical appearance makes it undistinguishable from more common malignant and benign pulmonary neoplasms. Other modalities, such as 18-FDG PET/CT findings reported by Pan et al 20 were non-specific as well. Similarly, chest imaging was ineffective in narrowing our patient's diagnosis.
Histiocytic sarcoma does not currently have a standard of treatment due to the rarity of the malignancy and the resulting lack of randomized control trials. Surgical resection, with or without chemotherapy and radiotherapy, remains the primary modality of treatment for patients with localized disease. For those with extensive or multifocal disease, multi-agent systemic chemotherapy regimens for non-Hodgkin lymphomas are often used. 24 Kommalapati et al found increased overall survival in those who received surgery compared to those who did not. 12 These treatment choice and survival trends were observed in those with reported pulmonary and gastric involvement.
In conclusion, we present a rare instance histiocytic sarcoma involving the right lung, stomach, and bilateral adrenal glands. The rarity of this histiocytic neoplasm makes excluding more common malignant and benign entities an essential step in its diagnosis. Initial radiological findings are mostly unhelpful in differentiating from more common malignancies. Histologic diagnosis may also be challenging since histiocytic sarcoma may display histological similarities to more common entities such as metastatic carcinoma, anaplastic large cell lymphoma, Langerhans cell histiocytosis, and metastatic melanoma. However, the specific expression of histiocytic makers can help elucidate its identity. While surgical resection is currently the most effective treatment modality, many patients present with unresectable advanced disease due to its aggressive nature. Systemic chemotherapy regimens can produce promising results in some patients but are usually more effective when administered as adjuvant to surgery. Advancements in genetic profiling and target therapy are needed to help diagnose and improve treatment outcomes.
Footnotes
Author Contributions
Resources: H.-W.C., C.-C.C., J.-S.L.; Writing – Original Draft Preparation: L.-W.L.; Writing – Editing and Reviewing: H.-W.C and L.-W.L.; Supervision: H.-W.C. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Ethical Approval
Not applicable, because this article does not contain any studies with human participants or animals.
Informed Consent
Not applicable, because this article does not contain any studies with human participants or animals.
Trial Regulation
Not applicable, because this article does not contain any clinical trials.