
Abstract
Anastomosing hemangioma (AH) of the paravertebral/paraspinal region is a rare, benign vascular neoplasm. In this single-center observational study, we describe the clinicopathological features of 13 patients with AH, with a female-to-male patient ratio of 1.2:1 and an age range of 18 to 63 years. Most lesions were located in the thoracic spine (69%), followed by the lumbar region (15%). Histologically, the tumors showed characteristic findings, including lobulated architecture with focal infiltration, an anastomosing, sinusoidal vascular growth pattern, hobnail-shaped endothelial nuclei, mild cytologic atypia, fibrin thrombi, and occasional extramedullary hematopoiesis. Immunohistochemically, the lesions expressed endothelial markers CD31 and CD34. Clinical follow-up was available for 12 patients, all of whom exhibited a benign course without local recurrence. This study underscores the key clinical and histopathological features of paravertebral/paraspinal AH, a rare site of involvement compared to its more commonly reported genitourinary counterpart, thereby aiding accurate recognition and diagnosis.
Keywords
Introduction
Montgomery and Epstein 1 first described anastomosing hemangioma (AH) in 2009, as a rare vascular neoplasm, often mimicking well-differentiated angiosarcoma and primarily occurring in the kidney and testis. Since then, AH has been reported at multiple sites, including the spermatic cord, adrenal gland, liver, spleen, retroperitoneum, mediastinum, ovary, colon, small bowel, mesentery, breast, uterine cornu, pelvic ligament, bladder, soft tissue, and bone, presenting either as unilateral or bilateral, synchronous tumors.2–4
The histological features of AH have remained consistent across anatomical sites. Lesions typically exhibit an infiltrative or lobulated architecture, composed of irregular, interanastomosing, capillary-sized vascular channels, often arranged in a sinusoidal pattern. These channels are lined by a single layer of endothelial cells that characteristically show hobnail-shaped nuclei, mild nuclear atypia, and rare mitotic figures. Scattered intravascular fibrin thrombi and hemosiderin deposits are frequently observed. Intracytoplasmic hyaline globules of varying sizes, sometimes containing coarse granules, have also been described in a few lesions, particularly arising in the kidney, ovary, and liver. The background stroma may be myxoid, fibrous, or edematous, and is often accompanied by inflammatory infiltrates and extramedullary hematopoiesis.1–10
Bean et al 11 identified an activating mutation in GNAQ codon 209 in 69% of AH lesions. This mutation affects the catalytic GTPase domain, leading to constitutive activation and overactivation of the downstream MAPK signaling pathway. Interestingly, other capillary hemangiomas, such as congenital hemangioma, also harbor the GNAQ mutation, whereas it has not been reported in angiosarcoma.
In a comprehensive 2016 study, John and Folpe 2 evaluated the radiographic and clinicopathological features of 17 patients with AH in unusual locations, noting a particular predilection for the paravertebral/paraspinal soft tissues. They emphasized that radiographic findings often fail to suggest a hemangioma, potentially resulting in unnecessary and overly aggressive treatment. Histologically, however, these lesions are indistinguishable from AH at more common genitourinary sites. Thus, pathologists must recognize this entity to avoid misclassification as more ominous or aggressive vascular neoplasms.
The present study aims to share our institutional experience with AH of the paraspinal and paravertebral region over the past 4 years, with emphasis on clinical presentation, histomorphological features, and patient outcomes.
Materials and Methods
This descriptive observational study was conducted following approval from the Institutional Ethical Review Committee. It included all patients diagnosed with AH involving the soft tissue and bone of the paravertebral/paraspinal region between 2021 and 2024, identified electronically through the Integrated Laboratory Management System. Hematoxylin and eosin (H&E) and immunostained slides were retrieved and independently reviewed by 2 pathologists having a special interest and experience in soft tissue pathology.
Data were extracted using a structured proforma and categorized according to patients' age, gender, and tumor characteristics, including site, size, architectural patterns, cytological features, immunohistochemical findings, and treatment details (surgical management and adjuvant therapy). Data analysis was performed using Microsoft Excel (version 16.85). Frequencies and percentages were calculated for categorical variables (eg, gender, tumor site, and morphological patterns), while measures of central tendency were applied for continuous variables such as age and tumor size. Results were summarized in tables and figures to illustrate key findings.
Results
Patient Demographics and Clinical Findings
A total of 13 patients with AH in the paravertebral/paraspinal region were diagnosed, including both in-house as well referred specimens for the primary diagnosis. The cohort comprised 7 female patients (54%) and 6 male patients (46%), with ages ranging from 18 to 63 years, a mean age of 38.5 years, and a median age of 41 years. Most lesions were located in the thoracic region (9 patients, 69%), followed by the lumbar region (2 patients, 15%). In 2 patients (15%), the exact paravertebral/paraspinal site was not specified. The overall clinicopathological features are summarized in Table 1.
Clinical features of Paravertebral/Paraspinal AH (n = 13).
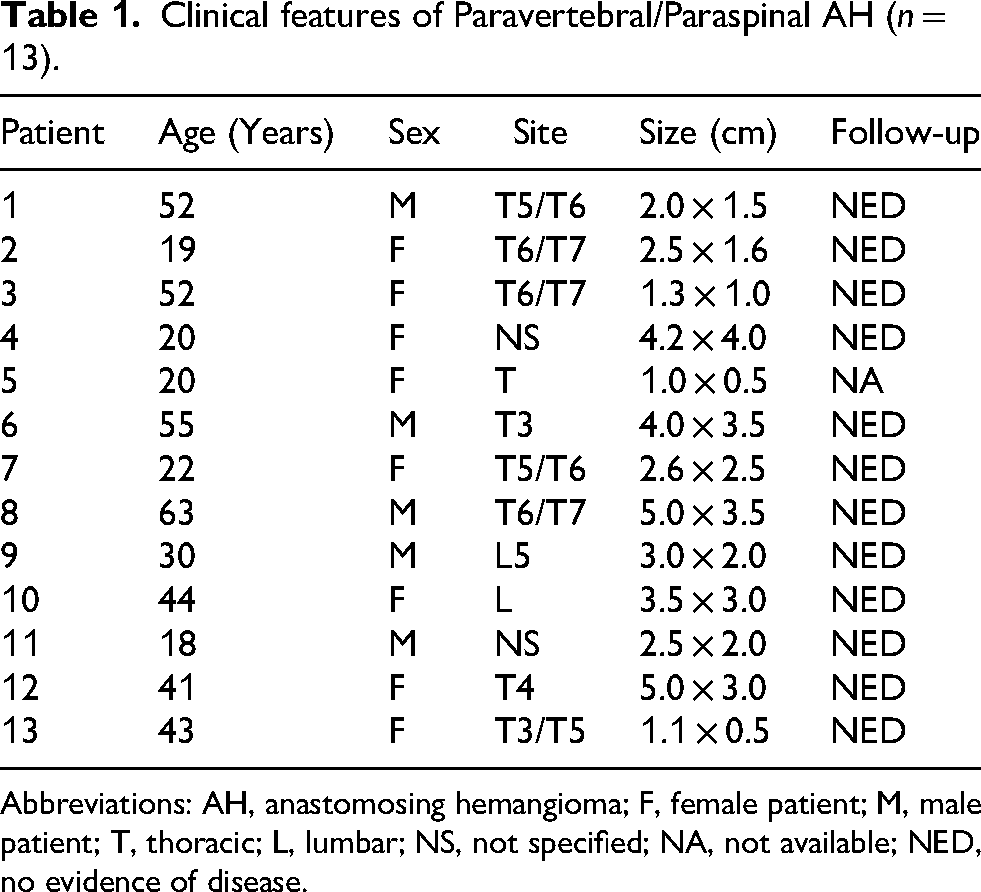
Abbreviations: AH, anastomosing hemangioma; F, female patient; M, male patient; T, thoracic; L, lumbar; NS, not specified; NA, not available; NED, no evidence of disease.
The most common presenting symptom was progressive paraparesis in 6 patients (46%), followed by acute-onset paraplegia in 2 patients (15%). Pain in both lower limbs, often associated with numbness, was reported in 2 patients (15%). The duration of symptoms ranged from 10 days to 1 year. All patients underwent excisional biopsy, and specimens were received as multiple fragmented tissue pieces measuring 0.5 to 5 cm in greatest dimension.
Radiological Findings
In-house noncontrast computed tomography imaging of the dorsal spine was available for one patient. A permeative lesion was identified involving the T7 vertebral body, with extension into the right pedicle, lamina, and paravertebral soft tissue as well as into the epidural space. No definite compression collapse was noted in the vertebral body. Posterior elements remained intact, with no evidence of instability (Figure 1).
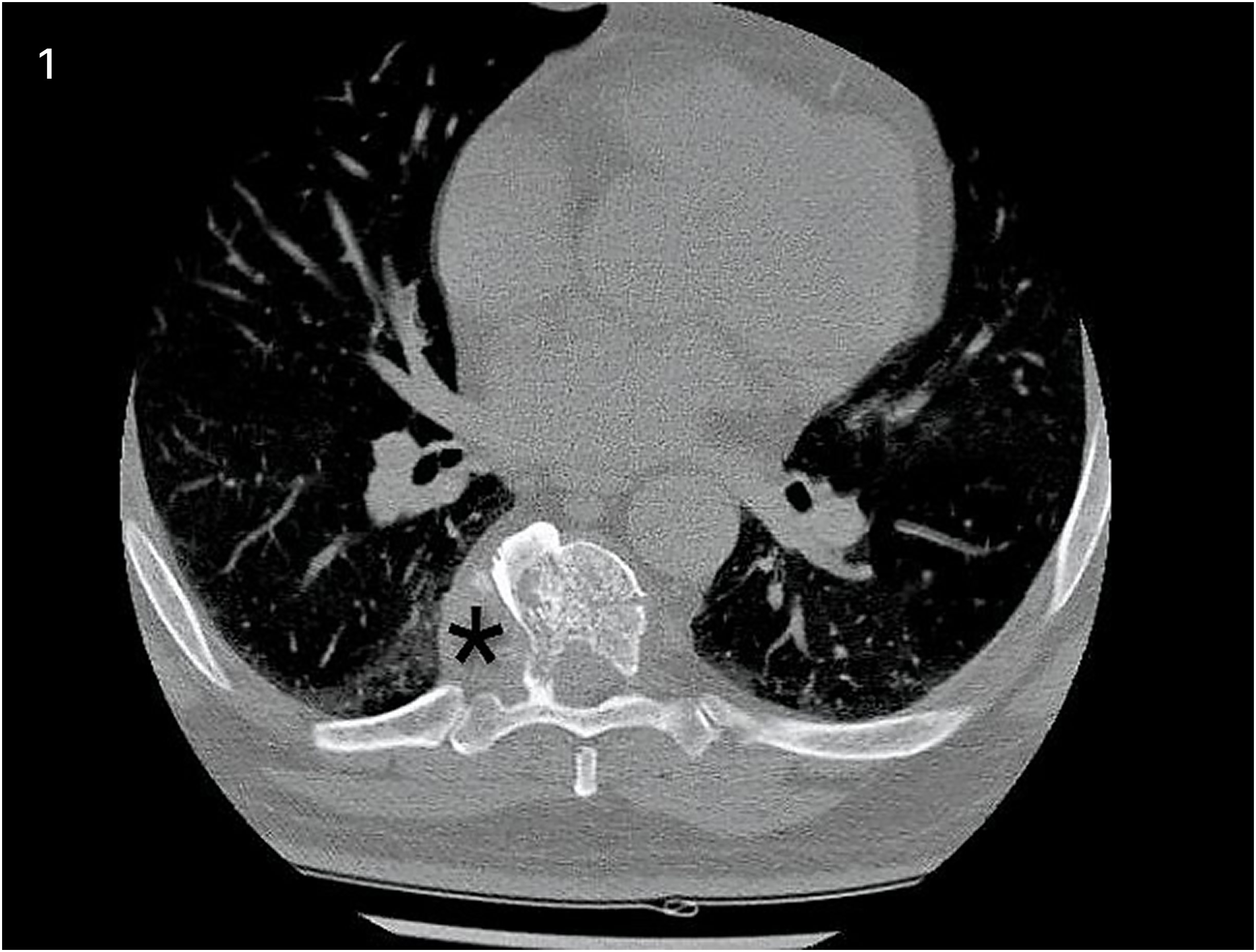
Coronal noncontrast Computed Tomography (CT) images of thoracic spine showing a permeative lesion involving the T7 vertebral body, with extension into the right pedicle, lamina, paravertebral soft tissue, and epidural Space (*).
Histological Features and Immunohistochemical Findings
At low magnification, lesions were located within bone or extended into the surrounding fibromuscular tissue. They were predominantly well-demarcated and lobulated, occasionally showing infiltrative architecture. All lesions consisted of capillary-sized vascular channels, and 1 lesion demonstrated involvement of a medium-caliber vessel.
At higher magnification, a prominent anastomosing sinusoidal vascular framework was observed, with mild endothelial cell atypia and hobnail-shaped nuclei. Mitotic figures were absent or rare, ranging from 1 to 2 per 10 high-power fields. The stroma exhibited edema and fibromyxoid changes, along with thrombosed vessels, foamy macrophages, and mild chronic inflammation (Figure 2A–F). Extramedullary hematopoiesis was present in a few lesions. Immunohistochemistry was performed on 6 lesions, all of which showed positive expression of the endothelial markers CD31 and CD34 (Figure 3).

(A) At low-power magnification, the lesion extends into surrounding fibromuscular tissue in a slightly infiltrative, but largely circumscribed manner (H&E stained). (B) At high-power magnification, it is a well-demarcated, lobulated lesion within bone. (C) Anastomosing, interconnected, small vascular channels lined by normochromatic endothelial cells. (D) The endothelial cells show hobnail-shaped nuclei without mitotic activity. (E) Small intravascular fibrin thrombi are seen. (F) Background stroma shows fibromyxoid changes.

Immunohistochemistry showing endothelial marker CD31 highlighting the anastomosing and sinusoidal configuration of vascular spaces.
Follow up
Follow-up was available for 12 patients, with a duration ranging from 4 months to 1 year. All patients were alive, reported improvement in nerve-related symptoms over the subsequent months, remained disease-free, and showed no evidence of recurrence at the last follow-up.
Discussion
The paravertebral/paraspinal region comprises the soft tissues surrounding the spine, extending from the fascia anteriorly to the aponeurosis of the paraspinal muscles posteriorly. Owing to its anatomical proximity to multiple spinal components, this region is a site for a wide spectrum of tumors, including lipomas, fibroblastic tumors, benign peripheral nerve sheath tumors, hemangiomas, and tumor-like benign masses such as hematomas, extramedullary haematopoiesis, or abscesses. 12
Vascular lesions account for approximately 3%–16% of all spinal and paraspinal masses, most commonly cavernous angiomas, capillary hemangiomas, and arteriovenous malformations (AVMs). 13 Cavernous angiomas are typically intramedullary in location and, in the familial setting, are associated with an autosomal dominant pattern of inheritance. Capillary hemangiomas, although rare, are usually extramedullary and may occur in either intradural or extradural locations, with histological resemblance to soft-tissue capillary hemangiomas. Among vascular lesions, AVMs are the most frequent, characterized by a nidus of arterial feeders and dilated draining veins. They may involve both extradural and intradural compartments or be confined entirely to the intradural space.14–16
As emphasized in the published literature, AH is often misinterpreted as well-differentiated angiosarcoma at the time of referral.2,17–19 However, the absence of adverse histologic features such as a diffuse infiltrative growth pattern, irregular and poorly formed vascular channels, marked cytological atypia, nuclear hyperchromasia, increased mitotic activity, endothelial tufting, multilayering, and necrosis supports a benign diagnosis.
Our cohort demonstrated a slight female predominance, with a female-to-male patient ratio of 1.2:1. The mean patient age was 36.8 years, which is considerably younger than the mean age of 66 years reported for 3 patients with paravertebral lesions in the series by John and Folpe, 2 as well as the 55 years reported in a case report by Fujita et al. 20
In our series, most lesions were well-marginated, involving both bone and adjacent fibromuscular tissue. The presence of a lobulated architecture, hobnail-shaped endothelial cells, an anastomosing vascular growth pattern, and fibrin thrombi closely paralleled the morphological features described in AH at other anatomical sites. However, interestingly, none of the lesions in our cohort demonstrated intracytoplasmic hyaline globules.
Fujita et al 20 reported a distinctive axial magnetic resonance imaging finding, characterized by horn-shaped extensions of the lesion encircling the spinal cord; however, similar features were not observed in either our in-house or referral patients.
Our series builds upon the observations of John and Folpe, 2 who highlighted a predilection of AH for deep soft tissue involvement in the paravertebral/paraspinal region, second only to the genitourinary tract. Given the rarity of this entity, only a small number of lesions were encountered in our institutional experience. Clinical follow-up data indicated a favorable outcome, with 12 of 13 patients alive and disease-free without recurrence at last follow-up.
Limitations
Although prior studies have highlighted the molecular pathogenesis of AH, particularly the recurrent GNAQ mutation, molecular testing was not routinely performed in our series due to unavailability at our center. This limitation reduces the ability to definitively differentiate AH from reactive or malformative capillary proliferations on a molecular basis.
Conclusion
We present the clinicopathological features of 13 patients with AH involving the soft tissue and bone of the paravertebral/paraspinal region. Awareness of this entity is essential for pathologists to avoid misdiagnosis as a more aggressive vascular neoplasm. Similar to AH in the genitourinary tract, paravertebral/paraspinal AH appears to follow an entirely benign course and typically requires only simple surgical excision for definitive management.
Footnotes
Author Note
Nasir Ud Din is now affiliated with the Department of Pathology and Laboratory Medicine, University of Miami, Miller School of Medicine, Miami, Florida, USA.
Ethical Approval
Ethical approval was sought.
Informed Consent
Not applicable, because this article does not directly involve human participants and/or animals.
Author Contributions
NU participated in the design of the study, retrieved data, and supervised. SS compiled data, did the literature search, and drafted the manuscript. MB edited the manuscript and supervised. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.