
Abstract
Objectives
Goblet cell adenocarcinoma is an amphicrine tumor composed primarily of goblet-like mucinous cells with variable numbers of endocrine cells and Paneth-like cells, typically arranged in crypt-like tubules. It typically arises in the appendix; primary extra-appendiceal goblet cell adenocarcinoma is rare. This study aimed to analyze the clinicopathological characteristics of extra-appendiceal goblet cell adenocarcinoma.
Methods
We retrospectively examined the clinicopathological, immunophenotypic and molecular features of patients with gastrointestinal and biliary goblet cell adenocarcinoma.
Results
Eight patients (four women) with tumors in the stomach (n = 4), colorectum (n = 3), and extrahepatic bile duct (n = 1) were evaluated. Tumors exhibited goblet or signet ring-like cells arranged in tubular, fused, infiltrative single-file, or anastomosing cord patterns. Some higher-grade tumors exhibited solid sheet-like growth with scattered goblet-like cells. Tumors were classified as low-grade (n = 2), intermediate-grade (n = 2), or high-grade (n = 4). All tumors expressed at least one neuroendocrine marker (synaptophysin, chromogranin A, insulinoma-associated protein 1). No mutations were detected in the KRAS, NRAS, PIK3CA, or BRAF. All seven tested tumors were microsatellite stable. Two of the patients had early-stage disease, while six had advanced disease, with two patients of death.
Conclusions
Extra-appendiceal goblet cell adenocarcinoma is rare and distinct, exhibiting similar histological, immunophenotypic and molecular features to its appendiceal counterpart. Histological grade and tumor stage have some predictive value with regard to prognosis. The incidence of this tumor may be underestimated, as it can be misdiagnosed as other tumors; awareness of it remains insufficient. These preliminary findings, constrained by a limited sample size, warrant validation in larger cohorts.
Introduction
Goblet cell adenocarcinoma is a distinctive mixed endocrine-exocrine tumor, characterized as an amphicrine tumor composed mainly of goblet-like mucinous cells, as well as variable numbers of endocrine cells and Paneth-like cells, typically arranged as tubules resembling intestinal crypts. 1 It was previously termed “goblet cell carcinoid”, as it was considered a low-grade malignant tumor with a biological behavior between that of well-differentiated neuroendocrine neoplasm and adenocarcinoma. 2 A 2016 study by Reid et al 3 analyzed a cohort of 77 patients with high-grade appendiceal goblet cell carcinoid and characterized the tumor as a highly aggressive and morphologically distinct entity specific to the appendix. Owing to frequent presentation with combinations of high-grade adenocarcinoma components and a biological behavior similar to that of adenocarcinoma, 4 the fifth edition of the World Health Organization (WHO) Classification of Tumors of the Digestive System in 2019 officially named it as “goblet cell adenocarcinoma”. The classification does not include references to extra-appendiceal goblet cell adenocarcinoma. 1 Recent reports have documented tumors occurring just outside the appendix, without appendiceal involvement.5–7 Case reports of primary extra-appendiceal goblet cell adenocarcinoma are currently rarely reported. This tumor is uncommon and easily confused with neuroendocrine neoplasm, adenocarcinoma, and signet ring cell carcinoma. 8 We collected a series of gastrointestinal tract and bile duct goblet cell adenocarcinomas in order to examine their clinicopathological, immunophenotypes, and molecular features. The aim of this research is to increase awareness and understanding of this particular tumor type among clinicians and pathologists.
Materials and Methods
Patients
Eight patients with gastrointestinal and biliary goblet cell adenocarcinoma who were treated via endoscopic or surgical resection at Beijing Friendship Hospital, Capital Medical University, were selected between November 2020 and August 2024. All of the slides were reviewed by two trained pathologists. Clinical data, including sex, age, endoscopic manifestations, treatment approach, and prognosis, along with imaging data, were collected for analysis.
Pathological Features
A retrospective analysis was conducted regarding the gross features, microscopic findings, and immunophenotypes of the eight tumors. The tumors were graded according to the latest WHO classification (fifth edition) for appendiceal goblet cell adenocarcinoma, 1 supplemented by the description of low- and high-grade features of appendiceal goblet cell adenocarcinoma developed by Bell et al. 9 The tumors were graded as follows: Grade 1 (>75% tubular or clustered growth), Grade 2 (50–75% tubular or clustered growth), or Grade 3 (<50% tubular or clustered growth).
Immunohistochemistry and Histochemistry
Immunohistochemistry for AE1/AE3, synaptophysin (SYP), chromogranin A (CHGA), insulinoma-associated protein 1 (INSM1), D2-40, and Ki-67 was performed using an automated stainer (Ventana, Tucson, AZ, USA). Elastica van Gieson staining was performed to evaluate vascular invasion. Alcian Blue (AB)-Periodic acid-Schiff (PAS) staining was performed to evaluate mucin content, following the manufacturer's protocol.
Molecular Pathology
PCR was conducted to perform genetic testing for KRAS, NRAS, PIK3CA, and BRAF on all eight tumor samples. Microsatellite instability testing was performed on seven of these samples, per manufacturer's protocol. One sample was excluded from microsatellite instability testing due to a lack of sufficient normal tissue for comparison.
Results
Clinical Features
Among the eight patients, four were men and four were women. Median patient age was 66.5 years (range: 53–79). Tumor locations included the stomach (n = 4), colorectum (n = 3), and common bile duct (n = 1). Preoperative biopsy correctly identified goblet cell adenocarcinoma in only one patient, while the remaining were diagnosed as poorly differentiated adenocarcinoma, signet ring cell carcinoma and mucinous adenocarcinoma. The therapeutic strategy was guided by a comprehensive preoperative evaluation. Accordingly, three patients suspected of having early-stage disease were treated with endoscopic submucosal dissection, while the other five patients, diagnosed with advanced disease, underwent surgical resection. The final pathological staging ranged from pT1 to pT4a, with lymph node metastases identified in three patients. Patient 1 initially underwent endoscopic submucosal dissection, followed by additional bowel resection and lymph node dissection due to positive lymphovascular invasion. This revealed a small amount of residual cancer and one lymph node metastasis. The final stage was pT3N1a. In the patient with a tumor in the rectum, ovarian metastases were detected 1 year later, followed by peritoneal metastases 22 months after the initial diagnosis. Patient 6 had concomitant type A gastritis. The details of the clinicopathologic findings and surgical procedures performed are summarized in Table 1. All patients underwent at least two preoperative and postoperative abdominal CT scans, supplemented by a PET–CT scan in one patient. Furthermore, no appendiceal abnormalities were noted during surgical examination. A retrospective review of all imaging studies by a specialist radiologist likewise revealed no evidence of a primary appendiceal lesion. Based on the combined evidence from surgical and imaging findings, all tumors were considered to be of primary origin.
Clinical Features and Staging Parameters of Eight Patients with Extra-Appendiceal Goblet Cell Adenocarcinoma.
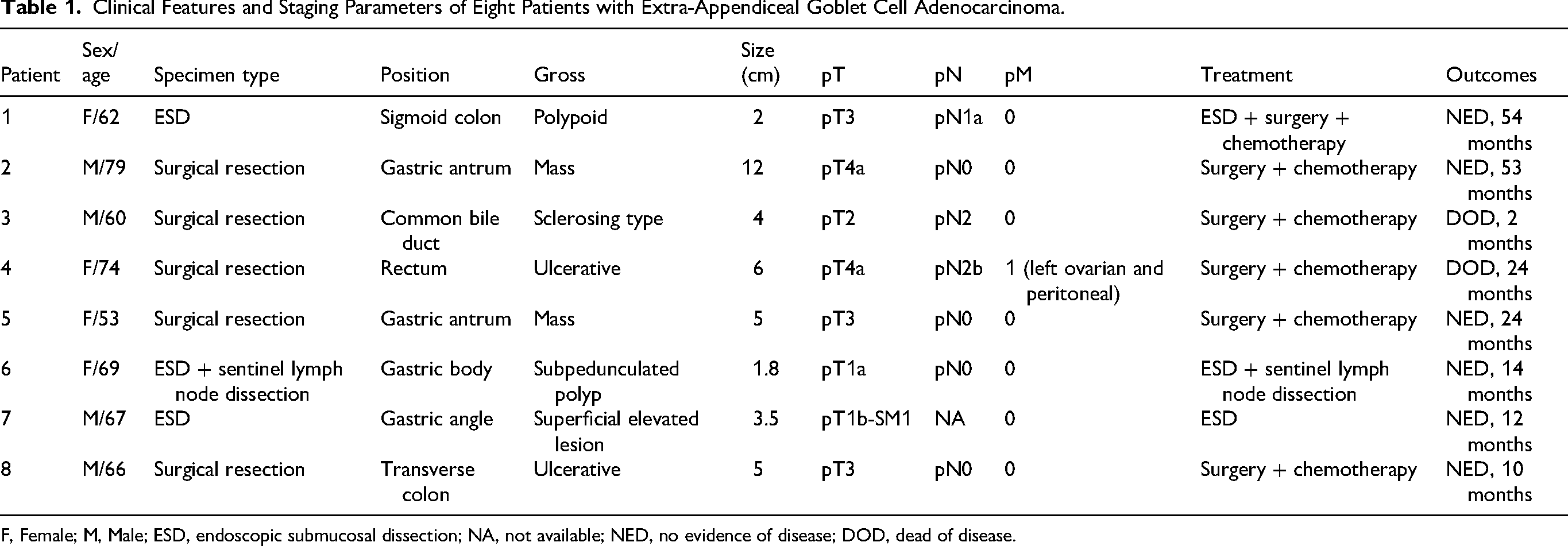
F, Female; M, Male; ESD, endoscopic submucosal dissection; NA, not available; NED, no evidence of disease; DOD, dead of disease.
Pathological Findings
The tumors ranged in size from 1.8 to 12 cm, with a mean size of 4.9 cm. Early-stage tumors presented as type 0-Isp and 0-IIa lesions, whereas advanced-stage tumors manifested as polypoid masses or ulcers. The tumor in the common bile duct exhibited a sclerosing pattern, leading to annular constrictive thickening of the bile duct (Figure 1).
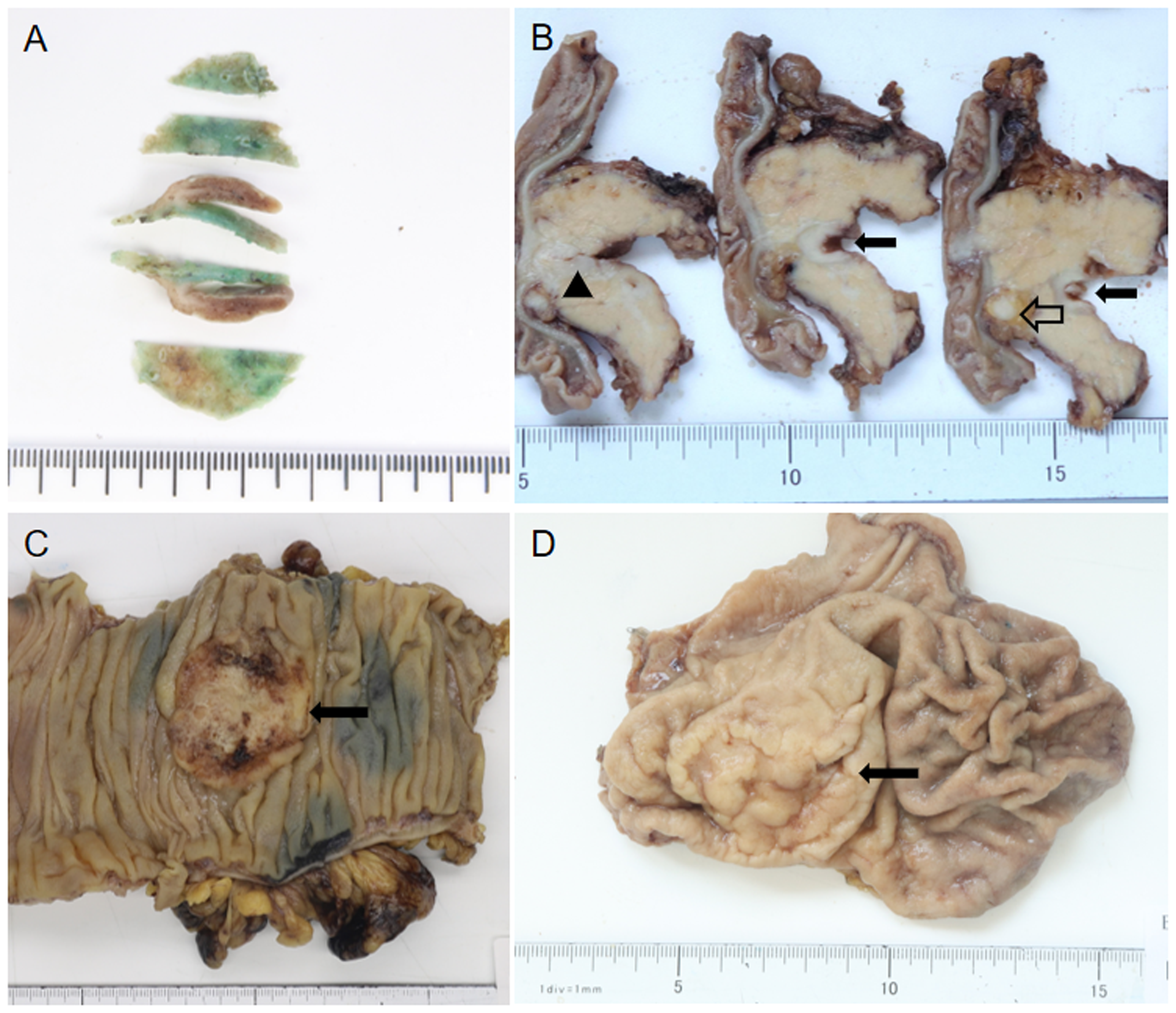
Macroscopic appearance of the extra-appendix GCA. A. An early stage tumor, presented as a 1.8×0.6 cm subpedunculated polyp in the gastric body. B. The cross section of the tumor occurring in the common bile duct, showed sclerosis and thickening of the bile duct (filled arrow) and suspicious involvement of the pancreas (triangle), and an enlarged lymph node was seen around the pancreas (open arrow). C. 5×4 cm ulcerative mass of the colon (filled arrow). D. 5×3 cm mass in the antrum of the stomach (filled arrow).
Following histological evaluation, two tumors were classified as Grade 1, two as Grade 2, and four as Grade 3. Lymphovascular invasion was observed in four tumors (Table 2).
Grading and Lymphovascular Invasion Status of Eight Patients with Extra-Appendiceal Goblet Cell Adenocarcinoma.
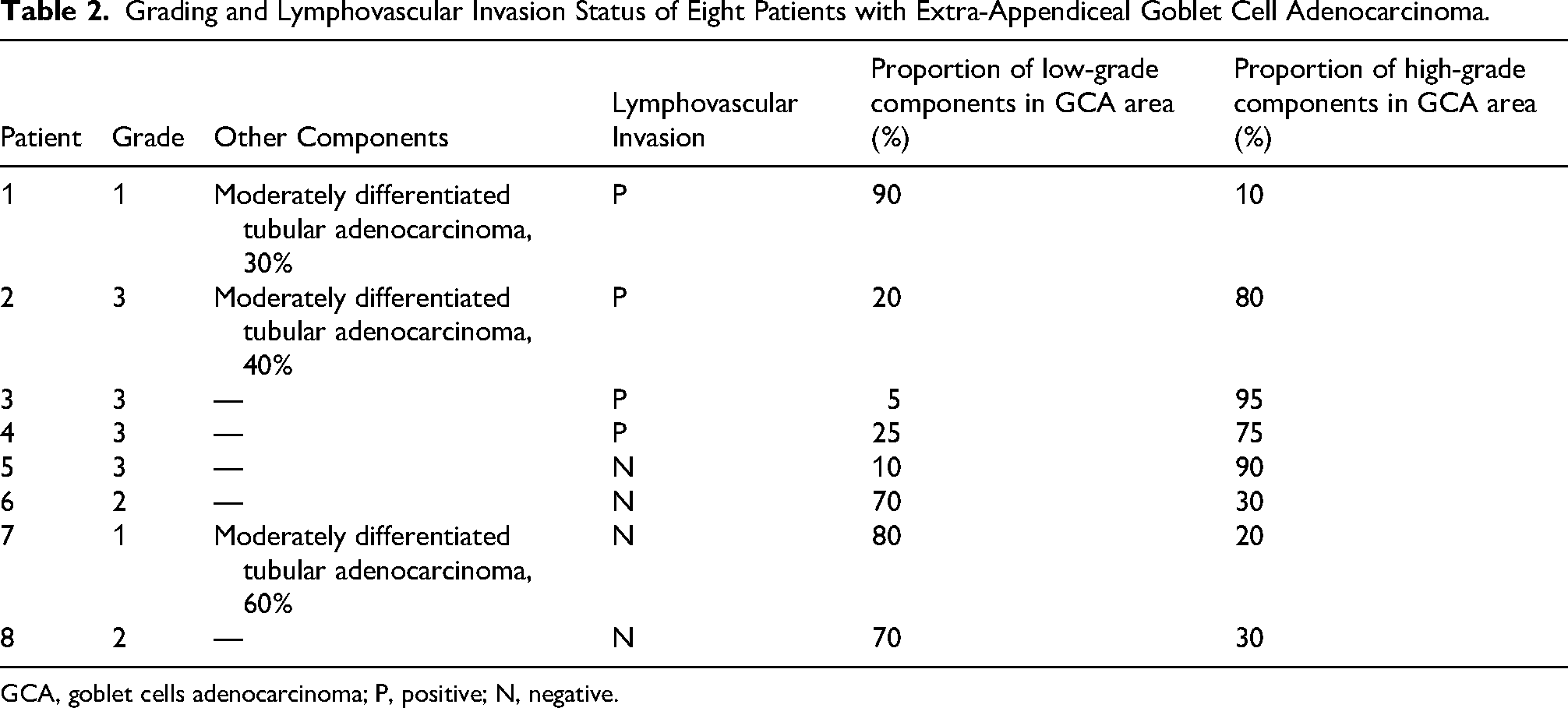
GCA, goblet cells adenocarcinoma; P, positive; N, negative.
The histological features of the tumors were broadly categorized into two groups (Table 2). The first group comprised five tumors characterized by pure goblet cell adenocarcinoma without additional histological components. The second group included three tumors with mixed goblet cell adenocarcinoma and conventional adenocarcinoma. The proportion of conventional adenocarcinoma components varied between 30% and 60% (Figure 2A). Additionally, dysplasia of the surface epithelium was observed in five tumors.

Histopathological features of the extra-appendix GCA. (A) Mixed GCA and conventional adenocarcinoma; the right part of the figure shows GCA, while the left part shows conventional adenocarcinoma. ×100 magnification. (B) Magnification of the GCA component in (A); tumor cells are arranged in a tubular pattern, and some of these tubules are located within extracellular mucin pools. ×200 magnification. (C) Tubular structures comprise cohesive clusters of goblet-like mucinous cells, with or without lumina. ×200 magnification. (D) Tubules invading the muscularis mucosae appear compressed. ×400 magnification. (E) The high-grade component of GCA comprises signet ring-like cells forming complex anastomosing structures; tumor cells exhibit prominent cytological atypia and numerous mitotic figures. ×400 magnification. (F) Tumor cells with high-grade nuclei diffusely infiltrated, with intracytoplasmic mucin scattered in few cells. ×400 magnification. (G) Tumor cells were positive for syn. ×200 magnification. (H) Some tumor cells were positive for CgA. ×200 magnification, the figure shows the same area with (C). (I) AB-PAS staining shows intracytoplasmic mucin of the signet ring-like cells; the figure shows the same area with (C). ×200 magnification.
The proportion of low-grade components varied between 5% and 90% (Table 2). Typical tubular structures, characteristic of appendiceal goblet cell adenocarcinoma, were observed in six tumors. These structures comprised small, cohesive clusters of goblet-like mucinous cells and endocrine cells, with or without lumina. Other low-grade features included extracellular mucin pools containing tumor cells or ruptured tubules (C-shaped glands), observed in four tumors, and tubules with nonmucinous glands, present in minimal amounts in four tumors. The low-grade components exhibited mild to occasionally moderate cytologic atypia and infrequent mitotic figures (Figure 2B–D).
The proportion of high-grade components varied from 10% to 95%. The most common high-grade morphological features included signet ring-like cells that diffusely infiltrated as single cells or formed large, complex anastomosing structures and large aggregates resulting from the fusion of clusters, both of which were observed in five tumors. In four tumors, single or anastomosing cords of tumor cells with high-grade nuclei were observed, with intracytoplasmic mucin present only focally. In two tumors, focal solid sheet-like growth patterns of tumor cells with high-grade nuclei and scattered intracytoplasmic mucin were observed. The high-grade areas exhibited prominent cytological atypia, including numerous mitoses and atypical mitotic figures (Figure 2E and F).
Immunohistochemical staining revealed that all eight tumors were positive for at least one neuroendocrine marker (SYP, CHGA, or INSM1), with varying proportions of positive cells (Figure 2G and H). Mucin staining with AB-PAS highlighted goblet cells and signet ring-like cells (Figure 2I). The Ki-67 proliferation index ranged from 20% to 90%. Specifically, the Ki-67 index ranged from 20% to 60% in the Grade 1 tumors, from 30% to 80% in the Grade 2 tumors, and from 30% to 90% in the Grade 3 tumors, with no significant differences in proliferative activity across the different grades (Table 3).
Histochemical and Immunohistochemical Staining Results.
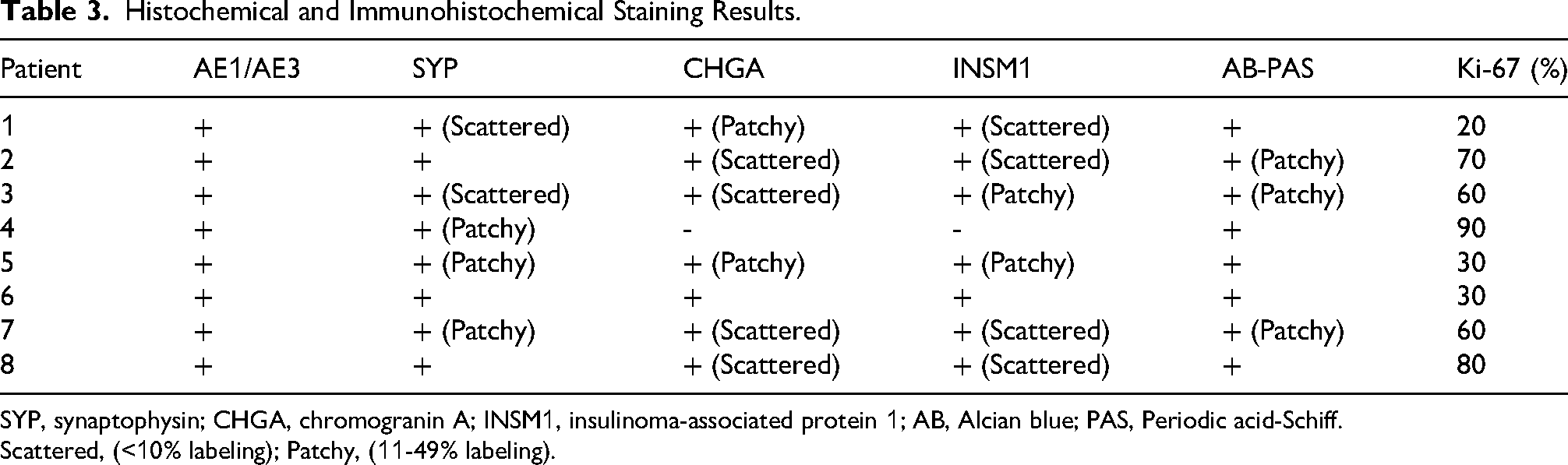
SYP, synaptophysin; CHGA, chromogranin A; INSM1, insulinoma-associated protein 1; AB, Alcian blue; PAS, Periodic acid-Schiff.
Scattered, (<10% labeling); Patchy, (11-49% labeling).
No mutations were detected in the KRAS, NRAS, PIK3CA, or BRAF genes in any of the eight tumors tested. All seven tumors tested for microsatellite instability were found to be microsatellite stable.
Follow-up Treatment After the Initial Resection and Survival Outcomes
Regarding treatment after initial resection, one of the three patients who underwent endoscopic submucosal dissection subsequently received additional surgery and chemotherapy. This patient remained tumor-free at 54 months. The remaining two patients did not receive surgery or radiotherapy, and remained tumor-free at follow-ups ranging from 12 to 14 months. All five of the surgical patients received postoperative chemotherapy. Among these, at the time of writing this report, two patients had died from the disease 2–24 months postoperatively; the other three patients remained alive and tumor-free at follow-ups 10–53 months (Table 1).
Discussion
Goblet cell adenocarcinoma is a rare amphicrine tumor, previously thought to occur exclusively in the appendix. Gui et al 10 reported that, of 16 patients with extra-appendiceal goblet cell adenocarcinoma, only 1 tumor (6.2%) was truly extra-appendiceal origin after comprehensive examination. Four patients (25%) were later diagnosed as primary appendiceal goblet cell adenocarcinoma. The authors concluded that extra-appendiceal goblet cell adenocarcinoma is most likely extra-appendiceal presentations of appendiceal primary, and thorough pathological examination of the appendix should be the diagnostic criterion. However, recent reports have documented tumors occurring just outside the appendix, without appendiceal involvement.5–8,11–13 The most common locations include the gastrointestinal tract, such as the stomach, colorectum, duodenum, ampulla, perianus, and esophagus. However, it can also occur in the ampullary region, with one tumor even having been reported outside the digestive system, in the bladder.5–8,11–13 Furthermore, in some patients, thorough histological examination of the appendix revealed no evidence of tumor, confirming the existence of primary extra-appendiceal goblet cell adenocarcinoma.10,14–16 Additionally, two colon tumors showed high-grade dysplasia of the lining epithelium, providing further evidence to support an extra-appendiceal origin.17,18 In our series of eight patients, both pre- and post-operative follow-up abdominal CT scans revealed no appendiceal lesions, and five tumors demonstrated dysplasia of the surface epithelium, supporting the possibility of extra-appendiceal origins. Since goblet cell adenocarcinoma was once considered a tumor specific to the appendix, we speculate that its actual prevalence may have been previously underestimated.
Some researchers have used the term “amphicrine carcinoma” to refer to extra-appendiceal goblet cell adenocarcinoma,19,20 while others have referred to it as mixed adeno-neuroendocrine carcinoma.21,22 Amphicrine carcinoma is also a rare tumor type characterized by the presence of both mucinous and neuroendocrine features within the same tumor cells. It may encompass goblet cell adenocarcinoma with a broader range of morphological features, and that goblet cell adenocarcinoma may be one of the most common types of amphicrine carcinoma with specific morphological features. 23 However, the current WHO Classification of Tumors of the Digestive System does not include the classification of amphicrine carcinoma. The term “goblet cell adenocarcinoma” used in the appendix was used in this study as it has become widely accepted in the literature.
A low-grade component is required for a diagnosis of goblet cell adenocarcinoma. The typical low-grade component is a tubule-like structure resembling an appendiceal crypt that contains goblet mucinous cells and a few neuroendocrine and Paneth-like cells. These tubules can rupture, forming extracellular mucus pools in which cells can be seen floating. Low-grade tumors are characterized by mild cellular atypia, infrequent nuclear mitoses, and often a lack of desmoplastic reaction. In contrast, high-grade tumors show marked atypia, including single or cord-like signet ring-like cells and complex cellular aggregates. Cells with reduced intracellular mucus may grow in linear or solid sheet-like patterns, with glandular structures occasionally present. All tumors in our cohort exhibited variable expression of at least one neuroendocrine marker (SYP, CHGA, or INSM1), and the presence of intracytoplasmic mucins was confirmed via AB-PAS staining. A previous study suggested that the prognostic significance of the Ki-67 index in appendiceal goblet cell adenocarcinoma varies significantly, making the role of proliferation rates a subject of ongoing debate. 2 The Ki-67 proliferation index ranged between 20% and 90% in our patients, indicating limited grading and prognostic relevance, consistent with previous findings. 2
Molecular studies have shown that appendiceal goblet cell adenocarcinoma is distinct from neuroendocrine neoplasm and adenocarcinoma, and that goblet cell adenocarcinoma has few or no mutations to the TP53, KRAS, BRAF, and APC genes, while mutations in genes related to Wnt signaling are frequent.24,25 Arai et al detected 592 groups of genes in 495 appendiceal tumor samples (53 goblet cell adenocarcinoma, 428 adenocarcinoma and 14 neuroendocrine neoplasm) using next-generation sequencing, and found that the mutation rates for TP53 (24.0%), ARID1A (15.4%), SMAD4 (9.4%), and KRAS (7.5%) were lower than those in adenocarcinoma; however, the mutation rates for CDH1, CHEK2, CDC73, ERCC2, and FGFR2 were higher than those in neuroendocrine neoplasm. 26 Microsatellite instability high was observed in none of the tumors. 26 Molecular studies in extra-appendiceal goblet cell adenocarcinoma have been less frequently reported. The most commonly mutated gene identified in a group of six tumors was TP53, while KRAS and APC mutations, which are common in adenocarcinoma, were not detected. This finding is consistent with appendiceal goblet cell adenocarcinoma. 5 In this study, no mutations were detected in the KRAS, NRAS, PIK3CA, or BRAF genes in any of the eight tumors tested. All seven tumors tested for microsatellite instability were found to be microsatellite stable. This is consistent with the results of previous studies. 5 Earlier evidence5,24–26 and our results indicate that the molecular genetic alterations in extra-appendiceal goblet cell adenocarcinoma differ from those in conventional adenocarcinoma and neuroendocrine tumors, aligning instead with those observed in appendiceal goblet cell adenocarcinoma.
It is widely hypothesized that appendiceal goblet cell adenocarcinoma originates from pluripotent intestinal stem cells at the base of intestinal crypts, which possess the capacity for both mucosal and neuroendocrine differentiation. 27 The origin of extra-appendiceal goblet cell adenocarcinoma is unclear, and it may similarly originate from stem cells. One reported example of goblet cell adenocarcinoma derived from Barrett's esophagus was considered to have originated from the altered intestinal crypt within the patient's Barrett's esophagus. 6 One unique finding in this case series was the coexistence of gastric goblet cell adenocarcinoma with type A gastritis in one patient, a phenomenon that has not previously been reported. It remains unclear whether the neuroendocrine differentiation observed in goblet cell adenocarcinoma is related to the proliferating ECL cells in the surrounding mucosa. This intriguing association warrants further investigation to elucidate its potential implications regarding tumor pathogenesis and behavior.
The incidence of extra-appendiceal goblet cell adenocarcinoma is likely underestimated in routine clinical practice, as it may be misdiagnosed as poorly differentiated adenocarcinoma, signet ring cell carcinoma, mucinous adenocarcinoma, or mixed neuroendocrine neoplasm–non-neuroendocrine neoplasms. In some lesions, the tumor may produce extracellular mucus resembling mucinous adenocarcinoma. High-grade components with abundant signet ring-like cells should also be differentiated from signet ring cell carcinoma. In this case series, only one patient was accurately diagnosed in the preoperative biopsy. The key to distinguishing goblet cell adenocarcinoma from other tumors lies in the presence of low-grade components with a unique tubular growth pattern. However, in some tumors, the low-grade component is scarce, requiring careful inspection. Some tumors exhibit a tubular pattern of non-mucinous cells that can resemble conventional tubular adenocarcinoma, these tubules are more distinctive due to their relatively round, rosette-like architecture, and rigid luminal borders. Additionally, goblet cell adenocarcinoma differs from signet ring cell carcinoma histologically in that the tumor cells tend to aggregate rather than infiltrate diffusely. The presence of distinct clusters of goblet cells is indicative of goblet cell adenocarcinoma. 28 A mixed neuroendocrine neoplasm–non-neuroendocrine neoplasm comprises two distinct components with different morphologies and immunophenotypes, each of which exceeds 30% of the total. While goblet cell adenocarcinoma is defined by its uniform, biphasic (neuroendocrine and glandular) differentiation within the same cell population. According to the latest WHO classification (fifth edition), 1 this term is best avoided in the context of goblet cell adenocarcinoma. The bidirectional differentiation characteristics of tumor cells can be demonstrated through the immunohistochemical detection of neuroendocrine markers and mucin staining. This can be used to rule out poorly differentiated adenocarcinoma or neuroendocrine carcinoma.
The fifth edition of the WHO Classification of Tumors of the Digestive System adopted the three-tiered scoring system proposed by Yozu, et al, 4 which grades tumors according to their proportions of low-grade (tubular or clustered growths) and high-grade (loss of tubular or clustered growths) cells. Prognosis of appendiceal goblet cell adenocarcinoma depends on stage and tumor grade. 1 Yozu et al 4 reported that histological classification is a significant independent prognostic factor, with marked differences in overall survival among patients with different grades. The median overall survival for Grade 1, 2, and 3 tumors was 204, 86, and 29 months, respectively. The study also demonstrated that tumor staging serves as a strong predictor of prognosis. Furthermore, a study by Reid et al 3 analyzed a cohort of 77 patients with high-grade goblet cell adenocarcinoma, revealing that 77% of patients involved peritoneal metastasis. A total of 33 patients (52%) died from the disease, with a median overall survival of 38 months and a 5-year survival rate of 32%. This confirms the highly aggressive nature of high-grade goblet cell adenocarcinoma. However, it should be noted that the study included only patients with high-grade goblet cell adenocarcinoma, resulting in a relatively poorer prognosis. Currently, there are limited prognostic data available for patients with extra-appendiceal goblet cell adenocarcinoma due to the small number of reports. A study by Lin et al included nine patients with extra-appendiceal goblet cell adenocarcinoma, of whom four died while the remaining five were followed for 5–46 months without recurrence or metastasis. 11 Our case series included two low-grade, two intermediate-grade, and four high-grade tumors of extra-appendiceal goblet cell adenocarcinoma. Death occurred in two of the patients, both of whom had high-grade tumors, suggesting a possible correlation between histological grade and prognosis. Tumor pT staging included two T1, one T2, three T3, and two T4 tumors. Ovarian and peritoneal metastases occurred in one T4 patient, who died two years after the initial surgery, indicating high tumor aggressiveness, consistent with previous reports. 3 Previous literature on extra-appendiceal goblet cell adenocarcinoma has almost exclusively documented advanced-stage tumors.6,7,14,18 In contrast, this study contributes two early-stage (pT1) tumors to the literature. Notably, both corresponding patients remained disease-free, suggesting a potential link between early tumor stage and favorable prognosis. These findings underscore the critical importance of combining histological grading with tumor staging to predict clinical outcomes. However, given the limited sample size, further validation with larger datasets is essential.
Despite its significant findings, this study was subject to certain limitations. First, although this study excluded appendiceal origin through imaging and surgical examinations, a histological examination of the appendix was not performed, and the possibility of an occult primary, though considered low, cannot be entirely ruled out. While it may be reasonable to exclude the appendix as the primary source of goblet cell adenocarcinoma found in extra-appendicular locations, it is unlikely that most reports will be able to demonstrate this, as shown in this study. Second, follow-up duration was insufficient for some patients. Further pathological and clinical studies with larger cohorts are warranted to provide sufficient information to optimize of clinical treatment strategies for extra-appendiceal goblet cell adenocarcinoma, as well as to enhance the current prognostic understanding of this malignancy.
Conclusions
Extra-appendiceal goblet cell adenocarcinoma has diverse morphological features; its immunophenotypes, as well as molecular genetic profiles, are consistent with goblet cell adenocarcinoma originating in the appendix. The incidence of this tumor may be underestimated, as it may be misdiagnosed as poorly differentiated adenocarcinoma, signet ring cell carcinoma, or neuroendocrine neoplasm. Current deficiencies in the overall understanding of this tumor may also lead to its underdiagnosis. Therefore, further studies are warranted to better characterize extra-appendiceal goblet cell adenocarcinoma and develop targeted treatment strategies to address it.
Footnotes
Acknowledgments
Ethical Approval
This study was approved by the Bioethics Committee of Beijing Friendship Hospital, Capital Medical University (Ethics Approval No.: 2025-P2-046-01).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Research Ward Excellence Program, National Key Research and Development Program of China (Grant Number BRWEP2024W162020100 (BRWEP2024W162020114), 2023YFC2507400 (2023YFC2507406)).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Not applicable (this manuscript does not report data generation or analysis).