
Abstract
Primary classical Hodgkin lymphoma of the urinary bladder is an extremely rare entity, with only a few documented examples in the literature. Most of the previously reported tumors represent secondary bladder involvement by systemic classical Hodgkin lymphoma, whereas only two tumors have been documented as primary classical Hodgkin lymphoma of the bladder. Here, we report a 71-year-old woman who presented with hematuria and urinary incontinence. PET/CT revealed a 44 × 53 × 60 mm hypermetabolic mass on the posteroinferior wall of the bladder, invading the anterior vaginal wall (SUVmax 18.2), with only regional pelvic lymph node involvement (SUVmax up to 8.8). Histopathologic examination of the transurethral resection specimen showed classical Reed–Sternberg cells within a mixed inflammatory infiltrate. Immunohistochemically, the tumor cells were positive for PAX5 (weak), CD30, CD15, and negative for LCA, CD20, CD79a, CD3, CD5, CD10. The tumor cells were also positive for Epstein–Barr virus (EBV)–encoded RNA (EBER) by in situ hybridization. In the absence of systemic involvement, the patient was diagnosed with primary classical Hodgkin lymphoma of the bladder. This rare presentation highlights the importance of considering classical Hodgkin lymphoma in the differential diagnosis of bladder tumors with atypical morphology.
Introduction
Malignant tumors of the urinary bladder are predominantly urothelial carcinomas, while primary involvement by non-Hodgkin lymphoma is exceptionally uncommon, representing fewer than 0.2% of all extranodal lymphomas and less than 1% of bladder neoplasms. 1 Classical Hodgkin lymphomas of the bladder have been reported only rarely in the literature.2–7 This report highlights the diagnostic challenges and clinicopathological features of this exceptionally rare primary bladder classical Hodgkin lymphoma and emphasizes that it should be considered in the differential diagnosis of bladder tumors with atypical morphology. We believe that this report provides valuable data for the limited existing literature on this subject.
Case Report
A 71-year-old female patient presented to our hospital with complaints of urinary incontinence and hematuria that had persisted for several months. Physical examination was unremarkable. The patient had a known history of type 2 diabetes mellitus and hypertension, with no history of primary malignancy. Full blood count was normal.
Urinary ultrasonography and cystoscopy revealed an approximately 5 cm solid lesion covering the trigone of the bladder. In addition, ureteral dilatation and grade 3 hydronephrosis of the left kidney were observed. The patient underwent transurethral resection of the bladder tumor.
On gross examination, the specimen measured a total of 25 cc and consisted of irregular, soft, cream-white tissue fragments. All samples were processed according to routine pathological procedures. Serial sections showed transitional-type epithelium on the surface, with focal areas of metaplastic squamous epithelium. Beneath the epithelium, a dense mixed inflammatory cell infiltration containing eosinophils and focal necrotic areas was observed.
In the stroma, highly pleomorphic tumor cells were identified, some of which were multinucleated or binucleated, with prominent eosinophilic nucleoli and abundant eosinophilic or partially clear cytoplasm. Apoptotic bodies and frequent mitotic figures were present (Figure 1).

Mixed inflammatory infiltrate composed of lymphocytes, plasma cells, and eosinophils beneath the urothelial lining, with scattered classic Reed–Sternberg cells (A–C, hematoxylin & eosin staining; ×100, ×200, and ×400, respectively).
Immunohistochemically, the tumor cells were positive for PAX5 (weak), CD30, CD15, and negative for LCA, CD20, CD79a, CD3, CD5, CD10 (MME). The tumor cells were also positive for Epstein–Barr virus (EBV)–encoded RNA (EBER) by in situ hybridization (Figure 2). The tumor cells were negative for keratin AE1/AE3, keratin CAM 5.2, EMA, keratin 7, keratin 20, p63, p40, uroplakin 3, thrombomodulin, desmin, SMA, S100, HMB45, Melan-A, myogenin, MYOD1, WT1, PAX8, CD68, ER, GCDFP15, mammaglobin, hCG. CD3 highlighted the background small T cells. These findings were consistent with classical Hodgkin lymphoma, mixed cellularity type.

(A, B) Reed–Sternberg cells showing positive staining for CD30 and CD15, respectively. (C) Weak PAX5 positivity in Reed–Sternberg cells (normal B lymphocytes are strongly stained). (D) Reed–Sternberg cells negative for CD3, with surrounding CD3-positive T lymphocytes forming a rosette pattern around them. (E) CD20 highlights background normal B lymphocytes, while Reed–Sternberg cells are negative. (F) LCA (CD45) shows negativity in Reed–Sternberg cells, with positive staining in background lymphocytes. (G) In situ hybridization for EBV-encoded RNA (EBER) revealed strong and diffuse nuclear positivity specifically restricted to the neoplastic HRS cells, while the background small-to-medium sized lymphoid cells remained negative (immunohistochemistry, ×400; EBER in situ hybridization, ×400).
PET/CT demonstrated a hypermetabolic lesion on the posteroinferior bladder wall extending into the lumen and invading the anterior vaginal wall, measuring 44 × 53 × 60 mm (SUVmax: 18.2). Hypermetabolic regional lymph nodes were also observed in the right obturator (19 × 24 mm, SUVmax: 8.8) and left interiliac (10 mm, SUVmax: 4.9) regions. No distant metastasis was detected.
The presence of a markedly FDG-avid mass located on the posteroinferior wall of the bladder (SUVmax 18.2) with only regional pelvic lymph node involvement (SUVmax up to 8.8), and the absence of distant metastasis, were consistent with primary classical Hodgkin lymphoma of the bladder.
Discussion
Primary lymphomas of the bladder is rare, and the majority of primary lymphomas arising at this site are non-Hodgkin lymphomas. 8 Classical Hodgkin lymphoma involvement is much rarer and only six patients have been reported in the literature. Most of the reported tumors represent secondary bladder involvement by systemic classical Hodgkin lymphoma,4–7 and only two of them have been identified as primary tumors.2,3
The extreme rarity of lymphomas in the bladder is attributed to the absence of lymphoid tissue in this region under normal conditions. However, as a result of chronic inflammation and similar factors, lymphoid aggregates known as mucosa-associated lymphoid tissue (MALT) may develop in the bladder over time, and lymphomas can arise from these tissues. 9 In our report, the EBV positivity observed is thought to reflect EBV-associated lymphoproliferative processes that may develop in elderly individuals with long-term immunosuppression, as noted in the literature. 10
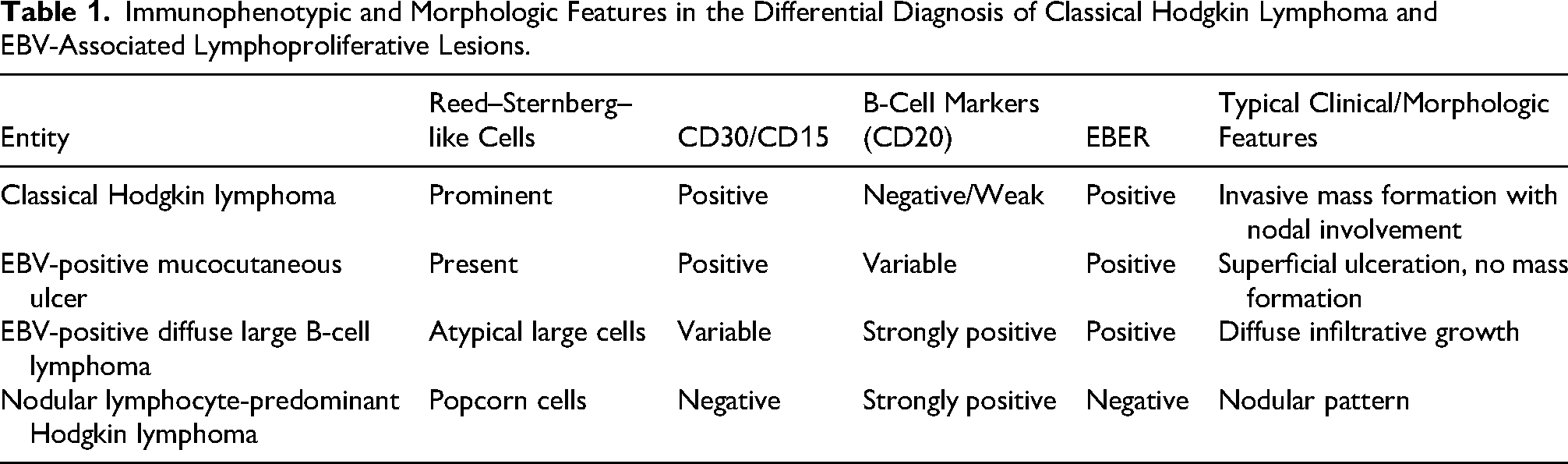
In the differential diagnosis of primary classical Hodgkin lymphoma of the bladder, exclusion of EBV-associated lymphoproliferative disorders is mandatory, particularly in elderly patients with detected EBV positivity. 11 EBV-positive mucocutaneous ulcer, which can morphologically mimic this diagnosis in mucosal sites, warrants primary consideration in the differential diagnosis. However, unlike in our patient, EBV-positive mucocutaneous ulcer typically follows a more superficial and limited clinical course. The 60-mm invasive mass and accompanying regional lymph node involvement in our patient support a diagnosis of classical Hodgkin lymphoma and favor it over EBV-positive mucocutaneous ulcer.11,12 Another significant entity for consideration is EBV-positive diffuse large B-cell lymphoma. This pathology generally exhibits strong and diffuse expressions of CD20 and CD79a. In our patient, the absence of these B-cell markers, coupled with weak PAX5 positivity and the presence of CD30/CD15 expression, solidified the diagnosis of classical Hodgkin lymphoma. 13 Furthermore, certain T-cell neoplasms, such as T-follicular helper cell-derived lymphomas, may trigger Hodgkin-like atypical B-cell proliferations in the background. This possibility is rendered unlikely in our presentation by the lack of a prominent T-follicular helper-phenotype T-cell infiltrate and the fact that CD3 staining was confined to reactive small lymphocytes. 14 Finally, nodular lymphocyte-predominant Hodgkin lymphoma is distinguished from the current presentation by the characteristic CD20 positivity and EBER negativity of its “popcorn” cells 15 (Table 1).
Immunophenotypic and Morphologic Features in the Differential Diagnosis of Classical Hodgkin Lymphoma and EBV-Associated Lymphoproliferative Lesions.
Although additional markers for EBV latency patterns (such as LMP1 and EBNA2) were not performed, the restriction of EBER expression to Reed–Sternberg cells strongly suggests a latency pattern consistent with classical Hodgkin lymphoma. The absence of EBER positivity in the background lymphoid cells helps to exclude a possible underlying T-cell lymphoproliferative disorder or other non-Hodgkin EBV-associated conditions.
In previously reported primary bladder classical Hodgkin lymphoma tumors, the most common presenting symptoms were hematuria, dysuria, and pelvic pain. Radiologically, these tumors usually manifest as a bladder mass with regional lymph node involvement, while distant spread is generally absent. In our patient as well, a 60-mm lesion located on the posteroinferior bladder wall with an SUVmax of 18.2 and only regional lymph node involvement (SUVmax 8.8) was identified.
This report represents the third reported example demonstrating the clinicopathological features of primary classical Hodgkin lymphoma of the bladder. With this report, we aimed to contribute to the limited existing literature and to emphasize that classical Hodgkin lymphoma should be considered in the differential diagnosis of bladder tumors with atypical morphology.
Footnotes
Acknowledgments
The authors used ChatGPT (OpenAI, San Francisco, CA, USA) for language editing and improvement of the manuscript. The authors take full responsibility for the content and interpretation.
Ethical Approval
Ethical approval was waived by the Institutional Ethics Committee of the University of Health Sciences, Antalya Training and Research Hospital because this study is a single case report with anonymized clinical data.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.