
Abstract
The staging of cervical carcinomas that appear confined to endocervical polyps presents a rare but recurring diagnostic and reporting challenge. Current classification systems, including the International Federation of Gynecology and Obstetrics (FIGO) 2018 staging system, the American Joint Committee on Cancer (AJCC) eighth edition, and College of American Pathologists (CAP) protocols, do not provide specific guidance for this scenario. Endocervical polyps are typically benign lesions, but in rare instances they may harbor invasive carcinoma. When invasion appears limited to the polyp stroma, assessment of the depth of invasion and assignment of a pathologic stage becomes challenging due to the polyp's limited, distorted, or fragmented architecture. Importantly, it is often difficult in routine practice to distinguish a truly polyp-confined carcinoma from an exophytic cervical tumor involving a polyp. This review highlights the gaps in staging of cervical carcinomas arising in or confined to endocervical polyps and draws cautious conceptual parallels to staging approaches in other organ systems, not to propose guideline changes, but to highlight existing gaps and reporting ambiguities. Currently, for reporting and staging purposes, pathologists use the same approach as that for other exophytic tumors. Here, we emphasize standardized documentation and transparent reporting of staging limitations as a practical interim approach, while acknowledging the absence of evidence sufficient to support formal staging modifications. Until additional data are available, careful descriptive reporting may facilitate clinical decision-making and enable future data collection needed to inform evidence-based revisions.
Introduction
Cervical carcinomas that appear confined to endocervical polyps pose a unique interpretive challenge for surgical pathologists, largely because this scenario is not clearly addressed in major staging systems, including the International Federation of Gynecology and Obstetrics (FIGO) 2018 staging system,1–3 the American Joint Committee on Cancer (AJCC) eighth edition, or the College of American Pathologists (CAP) protocols. 4 The definition of a carcinoma arising in a cervical polyp was first described in 1987 as “requiring the absence of disease in the base and remaining cervical tissue.” 5 Although tumors involving polyps may appear circumscribed, it is often not possible to determine with certainty whether invasion is truly limited to the polyp or represents an exophytic growth pattern arising from the cervical wall.
This article is intended as a narrative review and interpretive perspective, based on published literature and professional experience, rather than a proposal for immediate staging revisions. The discussion covers human papillomavirus (HPV)-associated adenocarcinomas and squamous cell carcinomas (SCCs), which share a common HPV-driven pathogenesis, though they may differ in certain molecular and clinical characteristics6,7 However, HPV-independent adenocarcinomas, particularly gastric-type adenocarcinoma (GAS), represent biologically distinct entities for which the considerations discussed here may not be applicable. 8
Endocervical Polyps: Histologic and Clinical Considerations
Endocervical polyps are benign, often incidental, exophytic growths protruding from the surface of the cervical canal. They are composed of a fibrovascular core containing blood vessels of varying sizes, often including thick-walled arteries, lined by endocervical glandular epithelium with variable squamous metaplasia.9–13 These common lesions typically arise in the endocervical canal of women aged 40 to 60 years.
Large retrospective studies demonstrate that premalignant and malignant lesions in endocervical polyps are uncommon but not negligible. Schnatz et al reported that approximately 2.7% of cervical polyps in women under age 50 may harbor premalignant or malignant lesions, while such findings are exceedingly rare in women under 20.14–17 The overall prevalence of malignancy ranges from 0.1% to 0.3% across multiple large series, with dysplasia identified in 0.4% to 0.7% of patients.12,14–16 Importantly, the prevalence of any abnormality (malignancy, dysplasia, or atypia) is significantly lower in postmenopausal women (1.4%) compared with premenopausal women (2.7%). 14
Both SCC and adenocarcinoma can arise within endocervical polyps, though primary invasive carcinoma originating within a polyp is distinctly rare. Park et al identified high-grade squamous intraepithelial lesions (HSILs) in 1.1% and SCC in 0.1% of 1905 endocervical polyps over a 12-year period. 12 Squamous intraepithelial lesions (SILs) occurring in endocervical polyps are frequently HPV-associated, with HPV DNA detected in 88% of lesions by in situ hybridization. 10 Importantly, in 8 of 9 patients with SILs arising in polyps, there was no evidence of dysplasia on colposcopic examination or biopsy of the remainder of the cervix, suggesting that these lesions can occur de novo within the polyp. 10
Adenocarcinoma arising within endocervical polyps has also been documented, though most malignancies identified in polyps represent metastatic involvement from endometrial or other sources rather than primary cervical lesions.15–17 The National Comprehensive Cancer Network (NCCN) Cervical Cancer Guidelines recognize that endocervical adenocarcinoma can demonstrate “stromal invasion and/or exophytic invasion,” acknowledging polyps or polyp-like lesions as distinct presentation patterns.18,19 Most primary cervical adenocarcinomas are HPV-associated usual-type, which are caused almost exclusively by HPV-16, -18, and -45. 20 Rarer variants include endometrioid, clear cell, mesonephric, and gastric-type subtypes, with the latter being HPV-independent and associated with more aggressive behavior. 21
Cervical SCCs account for approximately 75% of cervical carcinomas worldwide and arise on the ectocervix, with the majority (>90%) being HPV-associated, most commonly with high-risk HPV types 16 and 18.22,23 Adenocarcinomas comprise 20% to 25% of cervical cancers and develop in the endocervical canal, with adenocarcinoma in situ (AIS) as the precursor lesion.18,22,23 Unlike SILs, where invasion is not a concern for staging purposes, invasive carcinomas (whether squamous or glandular) require careful assessment of stromal invasion to assign stage and predict lymph node metastasis risk.22,24
The development of invasive carcinoma within endocervical polyps may be linked to chronic inflammation, hormonal exposure, or underlying dysplasia. When invasion arises in a polyp, the altered stromal architecture of the fibrovascular core differs substantially from the underlying cervical wall stroma, complicating direct application of depth-based staging metrics and necessitating careful identification of the presumptive point of origin. 25 Correlation with imaging—particularly MRI to assess cervical stromal involvement and tumor extent—and multidisciplinary discussion become essential for accurate staging and treatment planning. 26
Current Staging Systems and Their Limitations
For measurement purposes, the International Society of Gynecological Pathologists (ISGyP) recommends that depth of stromal invasion be measured from the basement membrane of the surface epithelium or the point of origin to the deepest point of invasion. 25 According to the CAP protocol for examination of resection specimens from patients with primary carcinoma of the uterine cervix, 4 accurate measurement of stromal invasion is essential for FIGO and AJCC staging for both SCC and HPV-associated adenocarcinoma.18,22,24,25,27 FIGO stage IA is defined as invasive carcinoma diagnosed only by microscopy with maximum depth of invasion ≤5 mm, subdivided into IA1 (stromal invasion ≤3 mm) and IA2 (stromal invasion >3 mm and ≤5 mm).18,22,27 For stage IB and beyond, both depth of invasion and tumor size (maximum diameter) become critical staging parameters.25,28 In SCC, the depth of invasion is a particularly important risk factor for recurrence, while in cervical adenocarcinoma, tumor size becomes more pronounced as a risk factor, especially in the presence of lymphovascular space invasion (LVSI). 18 The Gynecologic Oncology Group (GOG)/Sedlis criteria for adjuvant radiation after radical hysterectomy stratify risk based on the combination of LVSI, depth of stromal invasion (superficial, middle, or deep third), and tumor size, reflecting the clinical importance of accurate depth measurement.29–31
In addition, tumors that are predominantly or entirely exophytic—where there is little or no invasion into the underlying stroma—should not be regarded as in situ. Instead, the tumor thickness should be measured from the surface of the tumor to the deepest point of invasion. Furthermore, the depth of invasion should not be reported relative to the epithelial origin, as this may not truly reflect the biological potential of these tumors.4,32
The Silva pattern-based classification system provides a complementary approach for risk stratification of HPV-associated endocervical adenocarcinomas based on the destructiveness of stromal invasion rather than absolute depth. 18 Pattern A tumors demonstrate non-destructive invasion with well-demarcated rounded glands without solid growth, single stromal cells, desmoplastic stromal response, or LVSI, and have excellent survival without lymph node metastases or recurrences.18,33,34 Pattern B shows localized (early) destructive stromal invasion arising from well-demarcated glands, while Pattern C demonstrates diffuse destructive stromal invasion or solid growth. 18 Recent studies suggest combining pattern A and pattern B without LVSI into a low-risk group and pattern B with LVSI and pattern C into a high-risk group, as this binary classification demonstrates improved interobserver agreement and superior prognostic stratification.18,33–36
However, handling lesions where tumors appear to arise from within an endocervical polyp presents unique challenges that differ from tumors that are predominantly or entirely exophytic. Both the 2018 FIGO staging system 1 and the 2020 AJCC system 28 address exophytic tumors but do not provide specific guidance for carcinomas arising within polyps.19,25,28
The endocervical stroma refers to the supporting tissue of the endocervix beneath the epithelium, composed of dense fibro-muscular tissue containing vessels, lymphatic systems, and nerves. 37 Although endocervical polyps also possess a surface epithelium and an underlying stroma like the adjacent or underlying (deep to the polyp) endocervical tissue, the stromal architecture differs substantially. The fibrovascular core of endocervical polyps contains blood vessels of varying sizes, often including thick-walled arteries, embedded within a stromal framework that is distinct from the native cervical wall stroma.13,15,38 This altered architecture complicates the assessment of depth of invasion in polyp-based lesions.
The ambiguity in assigning a stage to lesions arising within endocervical polyps potentially leads to inconsistent reporting and management strategies. When invasion arises in a polyp, pathologists must carefully identify the presumptive point of origin within the altered stromal architecture and measure to the deepest invasive focus, but the biological significance of invasion depth measured within the polyp's fibrovascular core versus invasion into the underlying cervical wall stroma remains unclear. 25 This uncertainty is compounded by the fact that the fibrovascular stroma of polyps may have different immunophenotypic characteristics compared to native endocervical stroma, with studies demonstrating differential expression of CD34 and CD10 between endocervical and endometrial stromal cells. 39 Furthermore, the pattern-based Silva classification system for HPV-associated endocervical adenocarcinomas, which stratifies tumors based on the destructiveness of stromal invasion rather than absolute depth, may offer complementary prognostic information in polyp-based lesions. 40 However, its application to tumors arising within polyps has not been systematically studied, and the distinction between non-destructive invasion (Pattern A) and AIS can be particularly challenging in the context of a polyp's altered architecture.40,41
Lessons From Other Organ Systems
The challenge of staging carcinomas arising within polyps has been addressed in other organ systems, providing conceptual frameworks that may inform approaches to cervical carcinomas confined to endocervical polyps. However, it is important to acknowledge that these analogies are drawn from tumor types with substantially larger evidence bases and distinct biological behaviors, and their direct applicability to cervical carcinomas in polyps (currently supported by only limited case reports) requires cautious interpretation and prospective validation.
Endometrial Carcinoma
The 2023 FIGO staging system for endometrial cancer explicitly addresses carcinomas confined to polyps, defining stage IA1 as non-aggressive histological type (ie, low-grade endometrial endometrioid carcinomas) limited to an endometrial polyp or confined to the endometrium, whereas stage IC includes aggressive histological types (serous, high-grade endometrioid, clear cell, mesonephric-like, carcinosarcoma, undifferentiated, gastrointestinal-type mucinous, and mixed) within a polyp or confined to the endometrium without myometrial invasion.42,43 This staging framework is evidence-based and supported by studies demonstrating that endometrial carcinomas confined to polyps or restricted to the endometrium are associated with favorable prognosis regardless of the histologic subtype.44–47
Vulvar Squamous Cell Carcinoma
In vulvar carcinoma, tumor thickness and depth of invasion are measured separately, 48 with tumor thickness excluded from staging because vulvar carcinomas can have significant exophytic components. 49 The 2021 FIGO staging system adopted an alternative method to measure depth of invasion: the distance from the basement membrane of the deepest, adjacent, dysplastic, tumor-free rete ridge (or nearest dysplastic rete peg) to the deepest point of invasion, rather than the previous method measuring from the epithelial-stromal junction of the adjacent most superficial dermal papilla.24,49–51 This prompts down-staging some conventional stage IB (tumor size greater than 2 cm or stromal invasion greater than 1 mm) tumors to IA (tumor size less than or equal to 2 cm and stromal invasion less than or equal to 1 mm). Patients who are down-staged using this approach experience fewer inguinal recurrences, improved disease-specific survival, and lower risk of inguinal lymph node involvement at diagnosis compared to those with conventional stage IB disease, suggesting that lymphadenectomy may be avoidable in this down-staged group.48,50,51 Several studies assessed this alternative measurement method and demonstrated its prognostic superiority, findings that have been subsequently validated.52,53
Colorectal Carcinoma
In colorectal pathology, the management of carcinomas arising in polyps has been extensively studied because the depth of submucosal invasion is a critical determinant of lymph node metastasis risk and guides the necessity for additional surgical intervention.54–57 The Haggitt classification, proposed in 1985, stratifies pedunculated polyps into levels based on the extent of invasion: level 1 (invasion into the head of the polyp), level 2 (invasion into the neck), level 3 (invasion into the stalk), and level 4 (invasion beyond the stalk into the submucosa).58–60 In Haggitt's original study of 129 patients, when invasion was limited to the head, neck, or stalk (levels 1-3), there were no lymph node metastases and only 1 of 101 patients died with colorectal cancer; in contrast, 7 of 28 patients (25%) with level 4 invasion were diagnosed with lymph node or systemic metastasis. 60 For sessile polyps and poorly oriented or fragmented specimens, the Kikuchi classification may be used to assess the depth of submucosal invasion, where submucosal involvement is divided into superficial (SM1), mid (SM2), and deep (SM3) levels, with lymph node metastasis rates of 3.4%, 8.5%, and 22.6%, respectively.61–63
Implications for Cervical Carcinoma in Endocervical Polyps
These data from endometrial, vulvar, and colorectal tumor systems highlight the importance of potentially integrating scenarios of carcinoma arising in endocervical polyps into the FIGO and AJCC staging systems. However, several critical differences must be acknowledged. The endometrial polyp staging categories emerged from substantial outcome data demonstrating favorable prognosis for polyp-confined disease. The vulvar depth of invasion methodology was validated in studies with clinical outcome correlation. The colorectal Haggitt and Kikuchi classifications are supported by decades of accumulated evidence from thousands of patients with lymph node metastasis data.
In contrast, the current discussion of cervical carcinomas confined to endocervical polyps is based on extremely limited case reports, representing a completely different tumor type with distinct biology, HPV association patterns, and metastatic behavior. The extrapolation of frameworks from these other organ systems, while conceptually logical, requires prospective data collection and validation before any staging recommendations can be made. The primary value of these analogies lies in demonstrating that other staging systems have successfully addressed the challenge of carcinomas arising in polyps, providing a rationale for developing similar approaches for cervical carcinomas, but not in directly applying their specific criteria to cervical lesions without supporting evidence.
Future efforts should focus on systematic documentation of cervical carcinomas arising in endocervical polyps, including detailed pathologic parameters (depth of invasion within the polyp, invasion into underlying cervical stroma, tumor size, LVSI, Silva pattern for adenocarcinomas), clinical outcomes, and lymph node status, to establish an evidence base that could eventually inform staging recommendations specific to this rare presentation.
Histopathologic Challenges in Endocervical Polyp-Confined Carcinomas
The classification systems discussed above—including the Haggitt and Kikuchi classifications for colorectal carcinomas and the alternative depth measurement methods for vulvar SCC—cannot be directly applied to endocervical polyps. Unlike colorectal polyps, endocervical polyps lack a submucosa and may not always have a histologically identifiable stalk.19,64 The fibrovascular core of endocervical polyps, while containing stromal tissue, differs fundamentally from the layered architecture of the colorectal wall that underlies the Haggitt and Kikuchi systems.
Furthermore, the nature of the specimen received significantly impacts the ability to assess invasion. Specimens may be received fragmented and unoriented (Figure 1) depending on the procedure performed: resection versus polypectomy versus excisional biopsy (cone, LEEP, LLETZ) versus curettage.4,32,64 The NCCN Guidelines emphasize that the intent of a cone biopsy is to remove the ectocervix and endocervical canal en bloc using a scalpel, providing the pathologist with an intact, non-fragmented specimen without electrosurgical artifact, which facilitates margin status evaluation. When a LEEP is chosen for treatment, the specimen should not be fragmented, and care must be undertaken to minimize electrosurgical artifact at the margins.

Invasive endocervical adenocarcinoma, HPV-associated, arising in and confined to an endocervical polyp. Hematoxylin and eosin (H&E)-stained sections of endocervical curettage specimen examined at 40× (A) objective, and surgical resection specimen examined at 20× (B) and 200× (C) objectives. Positive high-risk HPV RNA in situ hybridization, DAB staining examined at 200× objective (D). The schematic was created in BioRender (2025) https://BioRender.com/cnxoveb.
However, in practice, specimens are frequently suboptimal. 19
Studies have demonstrated that biopsy specimens frequently underrepresent the presence and extent of stromal invasion. Djordjevic and Parra-Herran found that while the pattern of invasion on cone/LEEP specimens correlated with the overall pattern on hysterectomy in 92.8% of tumors, agreement between patterns in biopsy and the overall tumor was only 37.5%. 64 In all discrepant instances, biopsy failed to reveal destructive invasion that was evident on excision. 64 Similarly, Spasić et al reported that in papillary SCC (an exophytic variant), 94% of presurgical biopsies showed no evidence of stromal invasion, yet 76.5% of subsequent excision specimens demonstrated invasive carcinoma. 65 Besides, Rivera-Colon et al found that the pattern of invasion could be classified in only 50% of cervical biopsies for adenocarcinoma, compared with 100% of resection specimens. 66
When specimens are fragmented, poorly oriented, or limited to biopsy or curettage material, it is often inappropriate to assign a definitive pathologic stage due to the inability to accurately assess invasion. In such scenarios, the pathology report should clearly state the limitations and defer staging. The Association of Directors of Anatomic and Surgical Pathology recommends that the maximum depth of invasion by tumor into the cervical stroma, in millimeters or the proportion of the wall involved, should be recorded, with the depth of invasion measured from the base of the epithelium of the presumptive point of origin, whether squamous or glandular.24,67 However, when this measurement cannot be reliably performed, the report should explicitly acknowledge this limitation.
The presence of invasive carcinoma confined to a polyp, without stromal invasion beyond or deep to the polyp into the underlying endocervical tissue, complicates staging even further. No published guidelines explicitly address this scenario or incorporate it into any staging system or classification. The literature contains only a limited number of published case reports with adequate follow-up or prognostic data describing carcinomas confined to endocervical polyps. Berzolla et al reported that in a series of 2246 cervical polyps, malignancy was diagnosed in only 0.1% of specimens, and because no tumors represented primary malignancies arising de novo within polyps, the authors concluded that progression of cervical polyps to malignancy appears unlikely. 15
To support the relevance of this diagnostic challenge, we compiled previously published reports (Table 1) and briefly reviewed available outcomes, where reported. These data, though limited, suggest that some of these carcinomas may exhibit indolent behavior when confined to polyps. However, the small number of reported tumors and the heterogeneity of follow-up intervals preclude definitive conclusions about prognosis. For HPV-associated adenocarcinomas, the Silva pattern-based classification may provide complementary prognostic information, as Pattern A tumors have demonstrated excellent survival without lymph node metastasis or recurrence. Whether this favorable prognosis extends to Pattern A tumors arising within polyps remains to be determined. For SCC, the stage-for-stage prognosis is not dissimilar to that for adenocarcinoma, though adenosquamous and clear cell histologies may have inferior recurrence-free survival.22,71
Three Case Reports of Invasive Cervical Carcinoma Arising In and Confined to Endocervical Polyp Reported in Literature.
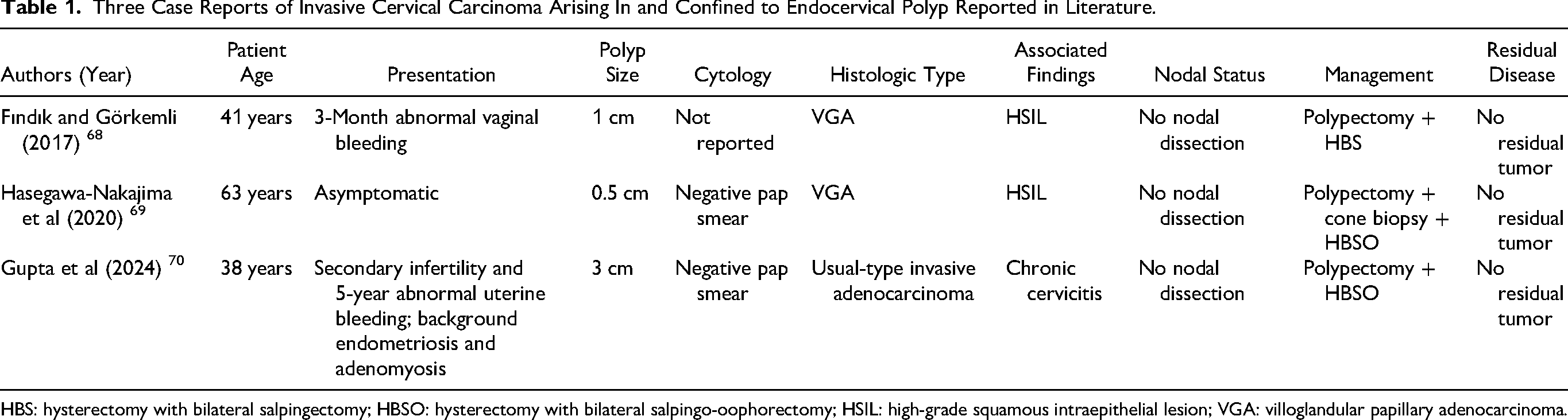
HBS: hysterectomy with bilateral salpingectomy; HBSO: hysterectomy with bilateral salpingo-oophorectomy; HSIL: high-grade squamous intraepithelial lesion; VGA: villoglandular papillary adenocarcinoma.
Considerations for Documentation and Reporting
Given the histopathologic challenges outlined above, standardized documentation is essential for carcinomas arising in endocervical polyps. Pathology reports should include: (a) tumor size (maximum diameter), histologic type, and HPV status; (b) whether invasion is confined to the polyp or extends into underlying cervical stroma; (c) depth of invasion within the polyp (if measurable); (d) presence or absence of LVSI; (e) margin status; (f) Silva pattern for HPV-associated adenocarcinomas; and (g) explicit acknowledgment of any limitations in staging due to specimen fragmentation, orientation, or the unique architecture of polyp-based lesions. This standardized documentation will facilitate future data collection and enable the development of evidence-based staging recommendations for this rare but clinically important presentation. To address these issues, we suggest the following considerations.
Histopathological Assessment
Pathologists are advised to meticulously evaluate the polyp to determine the extent of stromal invasion within or beyond the polyp. The depth of invasion should be measured from the base of the epithelium—whether squamous epithelial surface or an endocervical gland at the surface—that is involved by invasive adenocarcinoma to the deepest point of invasion.42,43 This approach aligns with the FIGO and AJCC staging systems, which measure depth from the base of the epithelium of the presumptive point of origin.42,43,46
If the invasive focus or foci are not in continuity with the surface epithelium, the depth of invasion should be measured from the deepest focus of tumor invasion to the base of the nearest surface epithelium or endocervical gland at the surface that is involved by invasive adenocarcinoma. If the invasive carcinoma is exclusively or predominantly exophytic and confined to the polyp, this should not be regarded as in situ lesion and the tumor thickness (from the surface of the tumor to the deepest point of invasion) should be measured, consistent with CAP protocol recommendations for exophytic tumors. 47
When measurement of the depth of invasion is not feasible, for example, in specimens with multiple invasive foci or significant fragmentation, the greatest linear dimension (maximum tumor diameter) should be measured microscopically and clearly stated on the pathology report. The pathology report should also clearly document the reason the depth of invasion cannot be assessed and explain why only the greatest linear dimension is provided. Whether the invasion is confined within the polyp stroma or extends beyond and deep to the polyp into the underlying cervical stroma should be clearly documented. This distinction is critical because the biological behavior of carcinomas confined to polyps may differ from those with cervical stromal invasion, though data remain limited.
To facilitate systematic data collection, we propose that the CAP protocol be extended to include documentation of polyp involvement. Under the “TUMOR” heading, the section “+Tumor Site (select all that apply)” can be extended to include “___ Endocervical Polyp.” Additionally, besides documenting “Depth of Stromal Invasion,” “+Extent of Depth of Stromal Invasion,” “+Horizontal Extent of Stromal Invasion,” and “+Silva System for Invasion,” an additional section could indicate whether the invasive carcinoma arose and is confined to a polyp or not. Gathering data on this opens the door for future research and enables prediction of tumor behavior in such scenarios. This approach provides critical insights into whether the scenario of carcinoma arising within a polyp should be incorporated into staging systems based on its prognostic significance or distinct tumor behavior.
Staging Assignment
In occasions where invasive carcinoma is confined to the polyp stroma and there is no evidence of underlying cervical stromal invasion (beyond and deep to the polyp), it is reasonable, for the time being, to consider staging by measuring the tumor depth of invasion—when possible—and sub-staging based on the 2018 FIGO staging system 1 and the 2020 AJCC system.28,42,43,46 This approach would essentially only include pT1 tumors (FIGO stage I), as carcinomas confined to polyps without cervical stromal invasion would by definition be limited to the cervix. The 2018 FIGO staging system defines stage IA as invasive carcinoma diagnosed only by microscopy with maximum depth of invasion ≤5 mm (IA1: ≤3 mm; IA2: >3 mm and ≤5 mm), while stage IB includes tumors with depth >5 mm or visible lesions, further subdivided by greatest dimension (IB1: ≤2 cm; IB2: >2 cm and ≤4 cm; IB3: >4 cm).42,43
However, this approach should be applied cautiously, acknowledging the lack of explicit guidelines addressing carcinomas arising in polyps. The ISGyP has provided recommendations for tumor staging of endocervical adenocarcinoma, emphasizing that pathologic findings are crucial in determining stage for early-stage disease, which in turn determines treatment and prognosis. 72 Yet these recommendations do not specifically address the unique scenario of polyp-confined carcinomas.
If a stage cannot be assigned due to specimen limitations or the unique architecture of polyp-based lesions, the pathology report may include a comment on the staging ambiguity due to current guideline limitations. For example: “Note: Most of the invasive component is confined to an endocervical polyp. The depth of invasion within the polyp measures [X] mm. The area of invasion shows focal destructive invasion (Silva pattern C). No invasion into the underlying cervical stroma is identified. Current staging guidelines do not explicitly address carcinomas confined to endocervical polyps; therefore, definitive staging cannot be assigned. Clinical correlation and multidisciplinary discussion are recommended.” This transparency aids in proper clinical decision-making and helps with future risk stratification and assessment.
Need for Guideline Updates
Rather than proposing immediate changes to staging protocols, professional societies such as FIGO, CAP, and ISGyP are encouraged to advocate for broader documentation and study of carcinomas confined to polyps. The International Collaboration on Cancer Reporting (ICCR) (an alliance formed by the Royal Colleges of Pathologists of Australasia and the United Kingdom, the CAP, the Canadian Partnership Against Cancer, and the European Society of Pathology) has developed standardized, evidence-based reporting data sets for cervical carcinomas. 73 This collaborative framework provides an ideal mechanism for incorporating polyp-specific documentation elements.
This initiative may, in the future, support formal revisions to existing guidelines. It could eventually lead to updates in the staging guidelines and reporting protocols to explicitly address tumors confined to endocervical polyps. Incorporating such criteria would enhance the accuracy of staging and treatment planning. The revised 2018 FIGO staging system was developed through review of literature and consensus view of the FIGO Gynecologic Oncology Committee and related societies, with the explicit conclusion that “data collection and publication will inform future revisions.” Systematic documentation of polyp-confined carcinomas represents an opportunity to generate the evidence base necessary for such future revisions. 46
Until formal guidelines are established, pathologists are encouraged to document all relevant histopathologic parameters in detail, clinicians should review these tumors in multidisciplinary tumor board discussions, and institutions should contribute data to registries or structured case series that may ultimately inform evidence-based staging recommendations for this rare but clinically important presentation.
Conclusions
The staging of invasive cervical carcinomas—both SCC and adenocarcinoma—confined to endocervical polyps remains a significant diagnostic challenge due to the absence of clear guidance in current staging systems, including the FIGO, AJCC, and CAP protocols. The unique histologic architecture of endocervical polyps, characterized by a fibrovascular core that differs fundamentally from native cervical stroma, complicates the direct application of depth-based staging metrics designed for conventional cervical carcinomas. Furthermore, the frequent receipt of fragmented or poorly oriented specimens compounds the difficulty in accurately assessing the extent of invasion within the polyp.
This narrative review highlights the need for updated staging guidance to better address tumors arising in endocervical polyps. However, until formal guidelines are established, pathologists—particularly gynecologic pathologists—are advised to provide comprehensive pathology reports detailing the criteria outlined above: tumor size (maximum diameter), histologic type, HPV status, whether invasion is confined to the polyp or extends into underlying cervical stroma, depth of invasion within the polyp (when measurable), presence or absence of LVSI, margin status, Silva pattern for HPV-associated adenocarcinomas, and explicit acknowledgment of any limitations in staging due to specimen quality or the unique architecture of polyp-based lesions. This standardized documentation could improve staging accuracy, clinical decision-making, and prognostication.
Future research, ideally involving international collaborations among pathologists, gynecologic oncologists, and professional societies, is needed to validate whether carcinomas arising within endocervical polyps exhibit distinct biological behavior that merits unique staging criteria. Systematic data collection through registries and multi-institutional case series will be essential to generate the evidence base necessary for future guideline revisions. Ultimately, clear and standardized criteria will facilitate more precise treatment strategies and potentially improve outcomes for patients with these rare but clinically important presentations.
Footnotes
Acknowledgments
Figure 1 was created with BioRender.com (accessed in October 2025). All rights and ownership of BioRender content are reserved by BioRender. BioRender content included in the completed graphic is not licensed for any commercial uses beyond publication in a journal. For any commercial use of this figure, users may, if allowed, recreate it in BioRender under an Industry BioRender Plan.
Ethical Approval
This work is mostly a narrative review without any new patient-level data generated. All images were derived from archival material used solely for illustrative purposes. Ethical approval is not applicable (No outright data included).
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not applicable.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The original contributions presented in this review are included in the article. Further inquiries can be directed to the senior author.