
Abstract

Brief Report
Secretory carcinoma (SC) is a malignant salivary gland neoplasm defined by the pathognomonic ETV6::NTRK3 gene fusion and notable for its histopathologic similarity to SC of the breast.1–3 Although SC classically exhibits solid, microcystic, and tubular growth patterns, it shows considerable morphologic heterogeneity, including the rare macrocystic subtype proposed in 2019.1,4 This subtype is defined by large cystic spaces filled with eosinophilic or mucinous secretions and may closely mimic benign cystic lesions or low-grade salivary malignancies such as cystadenoma and low-grade mucoepidermoid carcinoma, especially in limited biopsy samples.2,4 Given its recent recognition and risk of underdiagnosis, further reports are needed to clarify the clinicopathologic spectrum of macrocystic SC.
A 36-year-old man with no relevant medical history and no tobacco or alcohol use, presented with a 2-year history of a progressively enlarging left parotid nodule that had become painful on palpation in recent months. Physical examination revealed a well-circumscribed, fibroelastic mass measuring approximately 3.0 cm in the inferior pole of the left parotid gland, without cervical lymphadenopathy. Computed tomography demonstrated an expansile lesion up to 4.2 cm with well-defined margins, multilocular low-attenuation areas, and peripheral contrast enhancement, suggestive of cystic degeneration, extending to the deep lobe and ipsilateral temporomandibular joint (Figure 1A, B). Ultrasound showed a multilobulated cystic lesion with well-defined contours and preservation of adjacent structures. Fine-needle aspiration yielded serohematic cystic fluid with low cellularity and scant inflammatory cells and was non-diagnostic on two occasions. Based on these findings, a benign cystic neoplasm was initially suspected.

Clinicopathological features of the macrocystic subtype of secretory carcinoma. (A, B) Contrast-enhanced CT scan showing a heterogeneous enhancing mass in the left parotid gland (axial and coronal views). (C) Low-power H&E section demonstrating multilocular macrocystic pattern. (D-G) Representative H&E histology showing: (D) Epithelial lining interface with surrounding stroma, (E) papillary growth, (F) lining cells with hobnail and scattered cells with signet-ring appearance, (G) solid nests of tumor cells secretory features with eosinophilic cytoplasm. (H) Periodic acid-Schiff with diastase (PAS-D) highlighting extracellular mucin. (I-L) Immunohistochemical staining: (I) Mammaglobin strongly positive, (J) S100 diffusely positive, (K) p63 showing peripheral/myoepithelial cell staining (green arrows), (L) GATA3 nuclear positivity in tumor cells.
The patient underwent subtotal parotidectomy. Gross examination of the surgical specimen revealed a nodular, heterogeneous lesion measuring approximately 2.7 × 1.6 cm, with areas of cavitation, the largest of which measures 1.5 cm. Microscopic evaluation demonstrated a multi- and macrocystic architecture (Figure 1C), with cystic spaces lined by cuboidal (Figure 1D) to squamous epithelium exhibiting papillary intraluminal (Figure 1E) and intramural proliferation. The tumor cells showed often hobnail and vacuolated/signet-ring morphology (Figure 1F), with areas of hyaline secretory material (Figure 1G). A focally infiltrative growth pattern was also noted. Surgical margins were involved by the tumor.
Periodic acid-Schiff (PAS) with diastase confirmed the presence of a mucoid hyaline-secreted material (Figure 1H). Immunohistochemical studies revealed diffuse positivity for keratin 7, mammaglobin (Figure 1I), and S100 (Figure 1J), with focal expression of p63 (Figure 1K; restricted to the surrounding myoepithelial component of the papillary regions) and GATA3 (Figure 1L). Although molecular testing was not available, the panel provided was characteristic and sufficient to support for the diagnosis of SC, macrocystic subtype.
Given the malignant diagnosis, the patient underwent a second procedure consisting of total parotidectomy, ipsilateral level Va neck dissection, and facial nerve reconstruction with a sural nerve graft. Histopathological examination of the resection specimen demonstrated the absence of residual neoplasia, and all 16 lymph nodes retrieved were free of tumor. The final pathological staging was pT2N0M0. No adjuvant radiotherapy was administered. The patient has been followed for 18 months, with no clinical or radiological evidence of recurrence.
The salivary gland SC has emerged over the past decade as a distinct diagnostic entity defined by recurrent ETV6 gene fusions and a characteristic immunophenotype marked by diffuse S100, mammaglobin, and pan-TRK positivity.2,3,5 The morphological subtypes range from microcystic/solid, tubular, follicular, papillary-cystic, and macrocystic architecture, which can occur in different areas of the same lesion. 1 The macrocystic subtype clinical and histopathologic presentation frequently overlaps with both benign cystic lesions and other low-grade malignant tumors, creating substantial diagnostic challenges.4,6 In particular, this may closely mimic cystadenoma, papillary-cystic subtype of acinic cell carcinoma, intraductal carcinoma, and low-grade mucoepidermoid carcinoma, underscoring the need for clinical expertise and careful morphology, immunohistochemistry, and molecular testing. 4
Recent large series consistently show that SC is most commonly diagnosed in the parotid gland, with a median age in the fourth to fifth decades, and a slight male predominance, which is strictly in line with what has been reported for the macrocystic subtype.3,4 Different proposals for histological grading have recently been published, including a dichotomous classification based on the number of mitotic figures per high-power field and the presence of necrosis (low-grade and high grade), 2 and another tripartite classification based on architecture, septation and hyalinization of the stroma, nuclear/nucleolar atypia, number of mitotic figures in a 2mm2 field, proliferation index, presence of necrosis, lymphatic and perineural invasion, and infiltrative pattern. 3 In our specimen, mitotic figures were quite rare, necrosis was not evaluated, nor was perineural or lymphovascular invasion, in addition to the majority component of the lesion being papillary-cystic. In this scenario, in the dichotomous classification, it would be low-grade, and in the tripartite classification, it would be grade 1. Lesions with this profile have an expected disease-free survival rate of around 89.6%-93% at 5 years and 73-80.6% at 10 years.2,3
Diagnostic pitfalls surrounding SC largely stem from its cystic and papillary growth pattern. The Acinic cell carcinoma, particularly zymogen-poor subtype, may exhibit vacuolated cells and papillary-cystic structures, closely simulating SC. However, careful evaluation for true basophilic zymogenic granules, apical/membrane positivity for DOG1 (ANO1), nuclear positivity for NR4A3 (NOR1), and NR4A subfamily gene rearrangements are hallmark features of Acinic cell carcinoma and provide an important distinction. 7 Mucoepidermoid carcinoma represents another critical differential, especially in its low-grade cystic forms. The identification of true mucocytes, often highlighted by mucicarmine or PAS-D stains, and CRTC1/3::MAML2 fusions are diagnostic of mucoepidermoid carcinoma and absent in SC. Intraductal carcinoma, formerly known as low-grade cribriform cystadenocarcinoma, may show overlapping morphology and even S100/mammaglobin expression in its intercalated subtype. The presence of a continuous peripheral p63-positive basal layer and recurrent RET fusions are reliable distinguishing features. Cystadenoma lacks the diffuse S100, SOX10, mammaglobin, and MUC4 expression that typifies macrocystic SC. Finally, cystadenocarcinoma can mimic SC when predominantly cystic, but generally demonstrates greater cytologic atypia and invasive growth, without the diffuse mammaglobin, S100, and pan-TRK profile or recurrent ETV6 fusions. Pan-TRK is a cost-effective discriminator between SC and its mimics, particularly in limited cystic samples.1,4,5
Our proposed integrated diagnostic algorithm (Figure 2) addresses these pitfalls through a structured sequential approach based on the following key questions: (1) Are papillary-cystic spaces present? (2) Are vacuolated cells with hyaline secretions identified? (3) Is there a continuous peripheral rim of p63 expression? (4) Is there diffuse expression of S100, mammaglobin, or pan-TRK? (5) Is there diffuse expression of DOG1 or NR4A3 (NOR1)? (6) Is a specific recurrent gene fusion detected? Systematic integration of these morphologic, immunophenotypic, and molecular features reduces diagnostic ambiguity. Nevertheless, molecular confirmation remains the gold standard, including detection of ETV6::NTRK3 in SC, NR4A genes rearrangements in acinic cell carcinoma, CRTC1/3::MAML2 in mucoepidermoid carcinoma, and RET fusions in intraductal carcinoma. 8
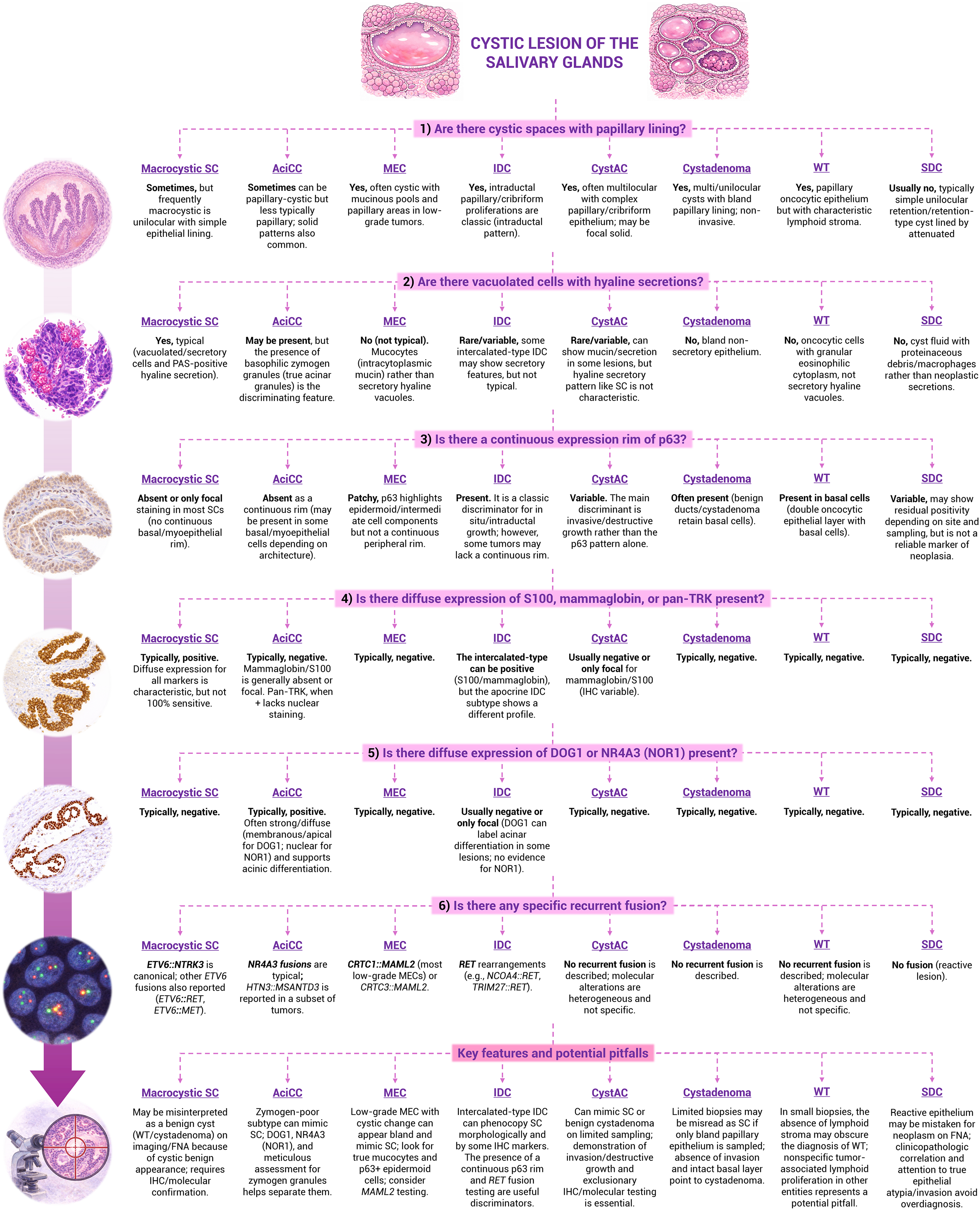
Proposed integrated diagnostic algorithm for cystic lesions of the salivary glands based on morphologic, immunohistochemical, and molecular features. This schematic summarizes a stepwise diagnostic approach integrating morphologic assessment, immunohistochemical profiling, and molecular alterations to aid in the differential diagnosis of cystic salivary gland lesions. The algorithm begins with evaluation of architectural features, including the presence of papillary epithelial lining and cystic complexity, followed by assessment of cytologic characteristics such as vacuolated cells and hyaline secretions. Subsequent steps incorporate key immunohistochemical markers, including p63 (continuous peripheral rim vs patchy expression), S100, mammaglobin, pan-TRK, DOG1 (ANO1), and NR4A3 (NOR1), which assist in distinguishing secretory carcinoma, acinic cell carcinoma, mucoepidermoid carcinoma, intraductal carcinoma, cystadenocarcinoma, cystadenoma, Whartin tumor, and salivary duct cyst. When indicated, evaluation of recurrent gene fusions (eg, ETV6::NTRK3, CRTC1/3::MAML2, RET rearrangements, and alterations involving NR4A subfamily genes) further refines diagnostic categorization. Key diagnostic pitfalls are highlighted, including morphologic overlap among low-grade cystic neoplasms and the importance of correlating immunophenotypic and molecular findings with architectural context. This proposed algorithm is intended as a practical diagnostic framework rather than a prescriptive guideline. Abbreviations: SC, secretory carcinoma; AciCC, acinic cell carcinoma; MEC, mucoepidermoid carcinoma; IDC, intraductal carcinoma; CystAC, cystadenocarcinoma; WT, Warthin tumor; SDC, salivary duct cyst; IHC, immunohistochemistry; PAS, periodic acid-Schiff; TRK, tropomyosin receptor kinase.
The therapeutic implications of accurate diagnosis are significant. Complete surgical excision with margin assessment remains the core management for SC. Adjuvant radiotherapy is typically reserved for tumors with high-risk features such as positive margins, perineural invasion, or nodal disease. 9 Notably, the identification of ETV6::NTRK3 fusion has direct therapeutic relevance, having the use of TRK inhibitors such as larotrectinib and entrectinib demonstrated high response rates in patients with advanced or unresectable SC, reinforcing the necessity of precise molecular characterization. 10
In conclusion, awareness of the macrocystic presentation of SC and its immunophenotypic profile is essential to avoid misdiagnosis. The proposed algorithm provides a reproducible diagnostic framework that may improve accuracy in routine practice, while broader access to immunohistochemical and molecular testing is expected to facilitate earlier recognition and appropriate therapeutic stratification, including targeted therapy when available.
Footnotes
Acknowledgments
São Paulo State Research Foundation (FAPESP, São Paulo, Brazil, grant numbers 22/07410-9; 23/14770-4).
Ethical Approval
Consent form was obtained. Ethical approval of the School of Medical Sciences of the Universidade Estadual de Campinas, Brazil (Approval number: 6.950.832).
Author Contributions
GSV and MWAG contributed to conceptualization, data curation, formal analysis, investigation, writing—original draft, and writing—review & editing. EFVS, CTC, AAT, and AA contributed to writing—original draft and Writing—review & editing. FVM contributed to conceptualization, data curation, formal analysis, investigation, writing—original draft, and writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundação de Amparo à Pesquisa do Estado de São Paulo, (grant number 22/07410-9).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.