
Abstract
Background
This study assessed the potential utility of GATA3, cyclin D1, KRT20, and GLUT1 immunohistochemistry (IHC) markers for diagnosing renal epithelial tumors.
Methods
A retrospective analysis was conducted on all eligible specimens (n = 95) diagnosed at our institution between 2014 and 2024. IHC was done and the staining intensity and distribution of selected IHC markers were assessed.
Results
Among 95 specimens, 26% were clear cell renal cell carcinoma, 21% were chromophobe RCC, and 17% were papillary RCC. Less frequent subtypes included TFE3-rearranged RCC, clear cell papillary renal cell tumor (CCPRT), papillary renal neoplasm with reverse polarity (PRNRP), and eosinophilic solid and cystic RCC (ESC-RCC). Clear cell RCC and CCPRT were consistently positive for cyclin D1 and GLUT1, and negative for GATA3/KRT20. CCPRT showed strong, diffuse GLUT1, unlike the limited staining in papillary RCC. PRNRP was positive for GATA3, cyclin D1, and GLUT1, and negative for KRT20. While chromophobe RCC exhibited variable GATA3 and GLUT1 expression with weak to moderate cyclin D1 positivity, oncocytomas were strong cyclin D1 positive, with negative GATA3, KRT20, and GLUT1. All 3 ESC-RCC specimens were KRT20 positive.
Conclusions
Our findings validate many previously reported observations and characterize adjunctive patterns of these less commonly used markers across renal tumor subtypes. It suggests GATA3 as a potential diagnostic tool for PRNRP, while GLUT1 demonstrates differential expression patterns for papillary RCC and CCPRT, aiding in distinguishing papillary renal tumors. Similarly, cyclin D1 appears to be a valuable adjunct in differentiating oncocytoma from chromophobe RCC. Also, KRT20 shows high specificity for ESC-RCC.
Keywords
Introduction
The precise diagnosis and subtyping of kidney tumors can be challenging due to their inherent biological heterogeneity, and significant overlap in morphologic and immunohistochemical (IHC) features. In recent years, renal tumor diagnostics have been refined by incorporating molecular markers alongside traditional morphology and IHC features. The 2022 World Health Organization (WHO) classification of renal tumors has embraced this integrated approach, to improve the accuracy of diagnosis and refine classification schemes. Consequently, new tumor categories have been defined, and the terminology for certain established categories has been updated. 1
Despite advancements, diagnostic challenges persist, and ongoing research is contributing to a fuller understanding of their characteristics and behavior. As our understanding of these tumors’ characteristics and behavior evolves through ongoing research, investigators explore novel IHC markers. These markers target key aspects of neoplastic cell biology, such as cell growth, differentiation, and metabolic adaptations, to enhance the characterization of differentiating features. Understanding these markers and their expression patterns will enable pathologists to improve diagnostic accuracy, leading to more effective treatment strategies and improved patient outcomes. 2
GATA3, a transcription factor of the GATA family, has emerged as a potential IHC marker in various cancers, including urothelial carcinomas. Notably, it has been reported to demonstrate high sensitivity and specificity for clear cell papillary renal cell tumor (CCPRT), formerly known as clear cell papillary renal cell carcinoma (RCC). This has aided in differentiating CCPRT from morphologically similar entities. 3 Furthermore, GATA3 has been implicated in the characterization of papillary renal neoplasm with reverse polarity (PRNRP), an emerging category in the 2022 WHO classification. 4 Accurate distinction between these entities is crucial due to their different molecular alterations, because PRNRN has recurrent mutations of KRAS. 5
Mechanistically, tumors exhibiting increased GATA3 expression have been shown to demonstrate enhanced cyclin D1 transcription. 6 Cyclin D1, a key cell cycle regulator implicated in various malignancies, including urinary bladder cancer, 7 also plays a significant role in renal tumor diagnostics. A strong cyclin D1 expression is characteristic of clear cell RCC, especially when others markers such as PAX8 and carbonic anhydrase 9 (CA9) are included to support the diagnosis. In fact, cyclin D1 staining intensity also can aid in differentiating renal tumor subtypes. 8 It also helps diagnose biphasic squamoid alveolar RCC (BSARCC), a rare, distinct morphological variant of papillary RCC.
Malignant cells, to sustain their rapid proliferation and meet their high energy demands, often exhibit metabolism, such as increased glucose uptake. This can be attributed to the Warburg effect and a heightened reliance on glucose transporter 1 (GLUT1; official name solute carrier family 2 member 1, SLC2A1), resulting in increased GLUT1 expression.. 9 Similarly, tumor cells also tend to fight the high oxidative stress resulting partly due to high metabolic activity, such as by inducing enzymes like carbonic anhydrase 9 (CA9). In fact, it is known that carbonic anhydrase 9 (CA9) and GLUT1 (SLC2A1) are both part of the same hypoxia inducible factor-1a (HIF1a) pathway and are also related to the pathogenesis of von Hippel-Lindau disease. 10 Interestingly, cyclin D1, a key cell cycle regulator, has been shown to promote GLUT1 expression, 11 further contributing to the enhanced glucose uptake observed in malignant tissues. Additionally, recent research suggests that GATA3 plays a role in nutrient-induced regulation of transcription factors. 12 Therefore, the expression patterns of GLUT1, cyclin D1, and GATA3 in renal tumors may reflect the tumors’ metabolic adaptations and proliferative activity.
KRT20 is an intermediate filament present in many epithelial tissues as part of the intracytoplasmic cytoskeleton and has been used in differentiating metastatic and local neoplasia as well as a prognostic marker. 13 KRT20 expression has also been found closely linked to GATA3 expression. Thus GATA3, cyclin D1, and GLUT1 may collectively determine the high cell growth supported by adjusting the energy needs. Adding KRT20 would impart additional prognostic value.
This study investigates the potential diagnostic utility of IHC markers GATA3, cyclin D1, KRT20, and GLUT1 in a diverse cohort of renal epithelial tumors, including emerging entities and characterize adjunctive patterns of a selected group of markers across renal tumor subtypes. The study aims to clarify the expression patterns of these markers, adding to the existing markers and to assess their potential role in differentiating morphologically similar tumor subtypes.
Methods
Study Design and Patient Selection
This retrospective study was conducted at the Anatomic Pathology Section, King Faisal Specialist Hospital and Research Centre (KFSH&RC), and the Departments of Pathology, Alfaisal University, Riyadh, Saudi Arabia, from July 2023 to June 2025.
Inclusion Criteria
All 95 specimens of renal epithelial neoplasm of various types, which had their tissue samples preserved, diagnosed at the Department of Pathology and Laboratory Medicine KFSH&RC, between January 2014 and December 2024 were included. Two pathologists reviewed all the histopathology sections to reclassify them according to the WHO classification 2022.
Exclusion Criteria
All renal epithelial neoplasms which did not have their tissue samples preserved at the participating institution were excluded. All other types of renal neoplasia were also excluded.
Tissue Processing
Formalin-fixed, paraffin-embedded tissue samples were processed using standard histological techniques. Sections of 3–4 µm thickness were cut, mounted on positively charged slides, and dried. Slides were then deparaffinized in xylene and rehydrated through a graded ethanol series.
IHC Staining
Heat-induced epitope retrieval was performed using Tris-EDTA buffer (pH 9.0) in a microwave oven (450 W) for 16 min, followed by gradual cooling and washing. Endogenous peroxidase activity was blocked by incubating the sections with 3% hydrogen peroxide for 10 min. The sections were then incubated with the following primary antibodies for 30 min at room temperature: GATA3 (clone L50-823, Roche), cyclin D1 (clone SP4, Ventana Roche), KRT20 (clone SP33, Ventana Roche), and GLUT1 (clone SPM498, Ventana Roche). All antibodies were used at ready-to-use concentrations, without further dilution.
Immunodetection was performed using a 2-step polylabeling method (Envision System, Ventana) with diaminobenzidine (DAB) as the chromogen. Hematoxylin was used as the counterstain, and slides were mounted with distrene-plasticizer-xylene (DPX). IHC staining was carried out on a Ventana BenchMark ULTRA automated slide stainer, according to the manufacturer's instructions.
IHC Interpretation
Nuclear brown staining was considered positive for GATA3 and cyclin D1. Membranous brown staining was considered positive for KRT20 and GLUT1. For all markers, sections exhibiting >1% positive tumor cells (either nuclear or membranous, as appropriate) were scored as positive, while >50% positivity was regarded as strongly positive.
Statistical Analysis
Data analysis was performed using SPSS version 23.0 (IBM Corp., Armonk, NY). Categorical variables are presented as frequencies and percentages.
Results
In our retrospective cohort of 95 renal epithelial tumors, the average age of patients was 49 years (SD = 17), ranging from 5 to 83 years. The average age was 51 years for male patients and 44 years for female patients. Male patients made up 65% of the cohort (n = 62) and female patients made up 35% (n = 33), with a male-to-female ratio of 1.9:1. Of note, in the TFE3-rearranged RCC subtype, 4 of the 6 patients were under 20 years old (ages 5, 6, 11, and 13), and 4 of the 6 were female patients.
Table 1 details the baseline demographic and clinical characteristics of the study population clear cell RCC was the most frequent diagnosis at 26%, followed by chromophobe RCC at 21%, and papillary RCC at 17%. TFE3-rearranged RCC made up 6% of specimens. Several less frequent tumor types were also identified, including CCPRT, PRNRP, eosinophilic solid and cystic RCC (ESC-RCC), tubulocystic RCC, mucinous tubular and spindle cell carcinoma (MTSCC), and oncocytoma. Additionally, a single specimen from each of the rare subtypes were observed: medullary, FH-deficient, fibromyomatous RCC, and eosinophilic vacuolated tumor. Finally, 8 RCCs could not be classified into any other category and were designated RCC-not otherwise specified (RCC-NOS). Figure 1 presents H&E-stained sections for 4 distinct renal tumor subtypes highlighting their characteristic cellular and structural features. It is noteworthy that both PRNRP and CCPRT have an indolent clinical behavior.

Representative hematoxylin and eosin (H&E) stained tissue sections of renal neoplasms at 200× magnification. (A) Clear cell RCC. (B) Papillary renal neoplasm with reverse polarity. (C) TFE3-rearranged RCC. (D) Eosinophilic solid and cystic RCC.
Baseline Demographic and Clinical Characteristics of the Study Population (n = 95).
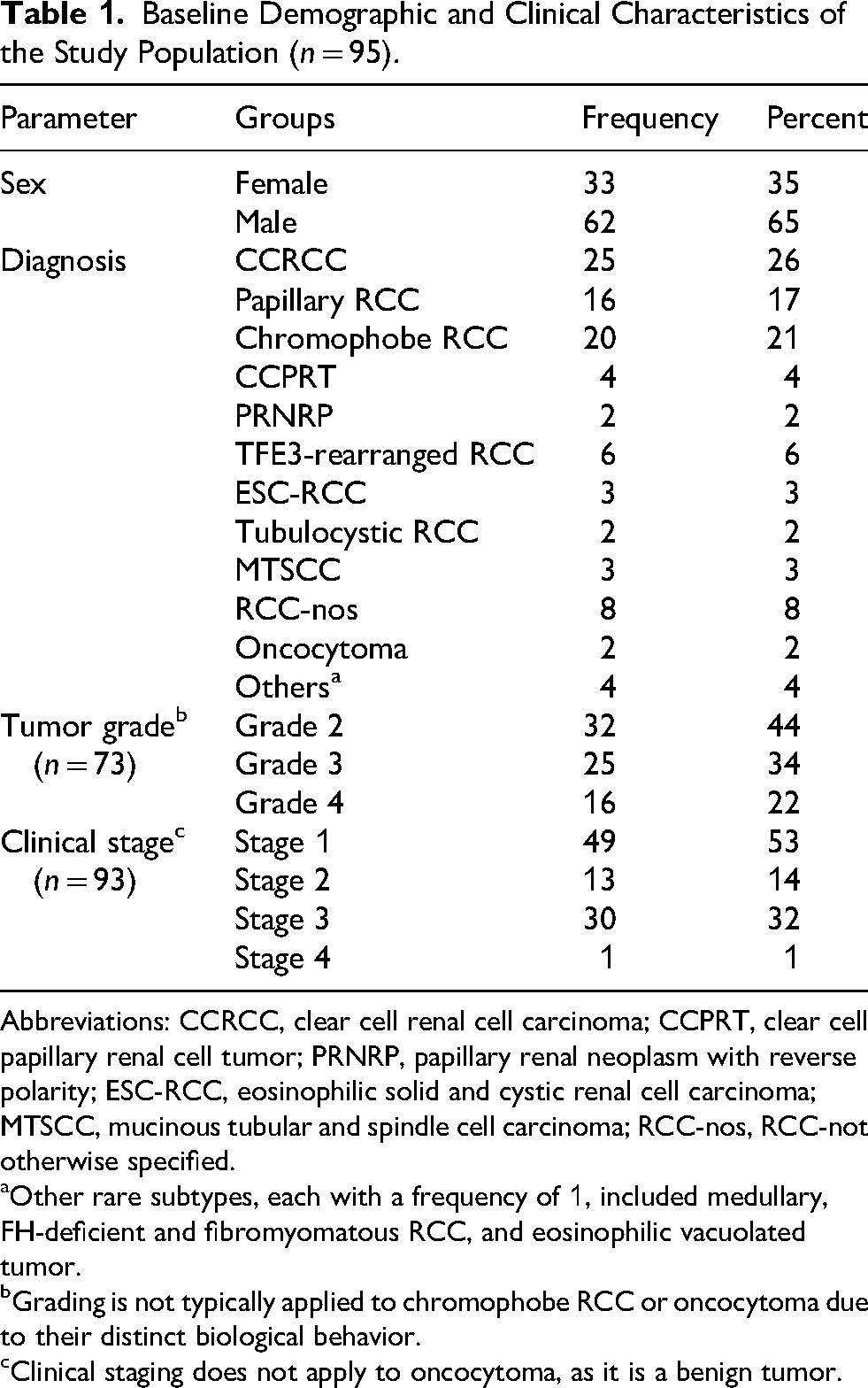
Abbreviations: CCRCC, clear cell renal cell carcinoma; CCPRT, clear cell papillary renal cell tumor; PRNRP, papillary renal neoplasm with reverse polarity; ESC-RCC, eosinophilic solid and cystic renal cell carcinoma; MTSCC, mucinous tubular and spindle cell carcinoma; RCC-nos, RCC-not otherwise specified.
Other rare subtypes, each with a frequency of 1, included medullary, FH-deficient and fibromyomatous RCC, and eosinophilic vacuolated tumor.
Grading is not typically applied to chromophobe RCC or oncocytoma due to their distinct biological behavior.
Clinical staging does not apply to oncocytoma, as it is a benign tumor.
Histological grading was performed for all the neoplasia except chromophobe RCC and oncocytoma. Among the 73 specimens for which grading was performed, the most tumors were grade 2 (44%), followed by grade 3 (34%) and grade 4 (22%). Of the 93 specimens with staging information, stage 1 tumors were most frequent (53%), followed by stage 3 (32%), stage 2 (14%), and stage 4 (1%). Staging did not apply to oncocytoma.
Table 2 details the IHC profiles of the kidney tumor subtypes. GATA3 positivity was limited, observed in only 6 of the 95 specimens. In comparison, cyclin D1 demonstrated high positivity, with 92 specimens positive. KRT20 expression was similarly low, with 3 positive specimens. GLUT1 expression was observed in 57 specimens.
Immunohistochemical Profile of Renal Epithelial Tumors (n = 95).
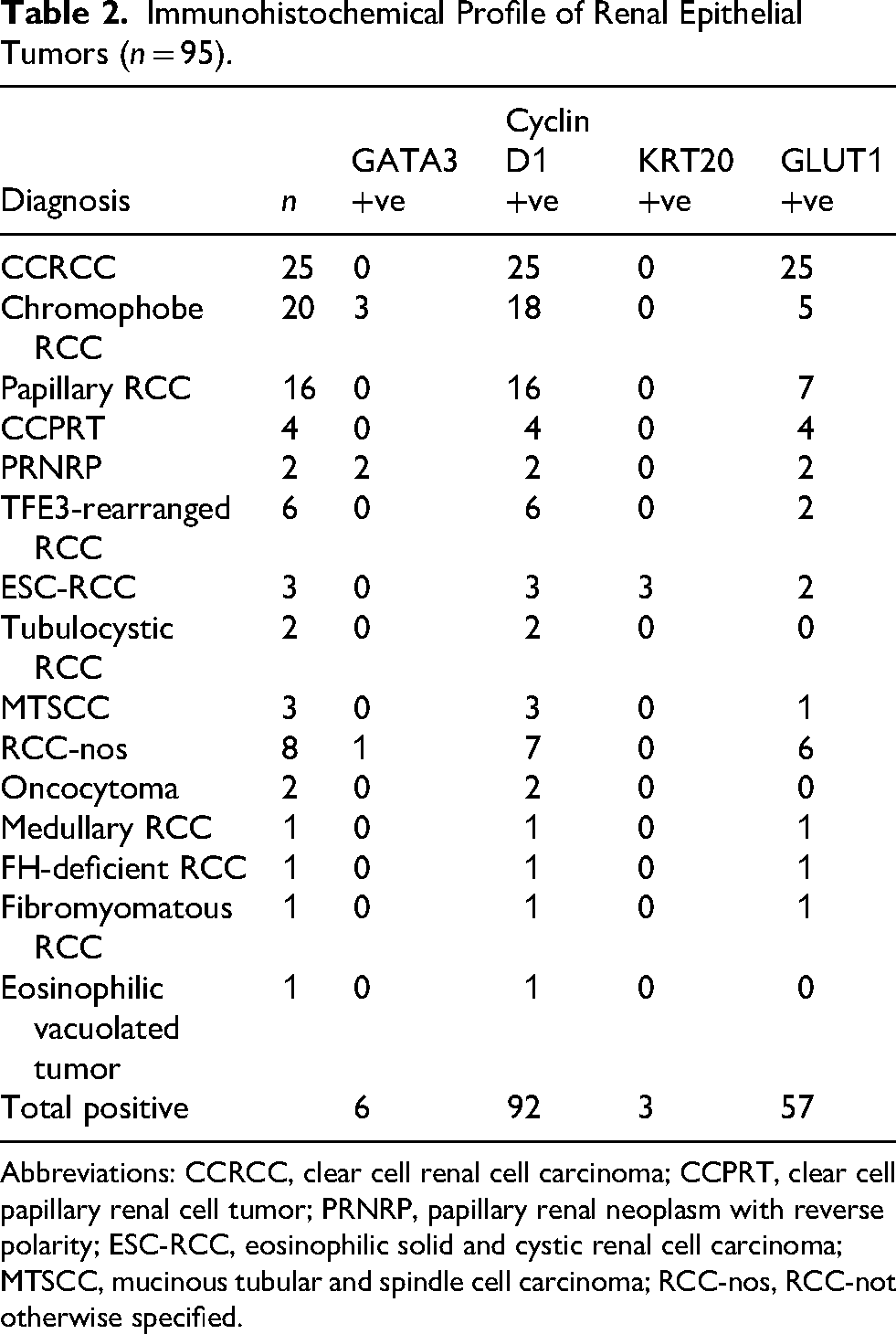
Abbreviations: CCRCC, clear cell renal cell carcinoma; CCPRT, clear cell papillary renal cell tumor; PRNRP, papillary renal neoplasm with reverse polarity; ESC-RCC, eosinophilic solid and cystic renal cell carcinoma; MTSCC, mucinous tubular and spindle cell carcinoma; RCC-nos, RCC-not otherwise specified.
Specifically, clear cell RCC displayed consistent cyclin D1 and GLUT1 positivity, and absence of GATA3 and KRT20. Similarly, papillary RCCs were GATA3-negative, with all 16 specimens positive for cyclin D1. While 7 papillary RCC showed some GLUT1 positivity, this was limited to less than 5% of cells in 6 specimens (Supplementary Table 1). In contrast, CCPRT consistently demonstrated strong, diffuse GLUT1 positivity in 90%–100% of cells. Figure 2A and 2B illustrates the differential GLUT1 expression between CCPRT and papillary RCC. Furthermore, CCPRT demonstrated consistent cyclin D1 and were consistently negative for GATA3 and KRT20. PRNRP showed consistent positivity for GATA3 (Figure 2C), cyclin D1, and GLUT1, and negativity for KRT20.

Immunohistochemical staining patterns in renal neoplasms at 200× magnification. (A) Clear cell papillary renal cell tumor demonstrating strong, diffuse, predominantly membranous GLUT1 staining. (B) Papillary renal cell carcinoma showing mild, focal GLUT1 staining. (C) Nuclear GATA3 expression in papillary renal cell carcinoma with reverse polarity. (D) Membranous KRT20 staining in eosinophilic solid and cystic renal cell carcinoma.
Meanwhile, chromophobe RCC showed variable GATA3 and GLUT1 expression, while cyclin D1 was positive in most specimens, though generally with weak to moderate staining intensity limited to less than 50% of cells. In contrast, oncocytomas consistently exhibited strong cyclin D1 positivity in 80%–100% of cells and were negative for GATA3, KRT20, and GLUT1 (Supplementary Table). Similarly, TFE3-rearranged RCC displayed consistent cyclin D1 positivity, with some GLUT1 positivity and the absence of GATA3 and KRT20.
ESC-RCC was characterized by consistent positivity for cyclin D1, KRT20 (Figure 2D), and GLUT1, and negativity for GATA3. The IHC profiles of the other rare subtypes are also presented in Table 2.
Discussion
The 2022 WHO classification of renal neoplasms reflects the increasing recognition of tumor heterogeneity and incorporates morphological, IHC, and molecular data. While traditional markers like PAX8, CA9 and CD10 have been widely used, there is a growing interest in exploring additional novel IHC markers that may enhance diagnostic accuracy and prognostic stratification. Therefore, this study investigated the potential diagnostic utility of established IHC markers GATA3, cyclin D1, KRT20, and a metabolic marker GLUT1in renal tumors.
GATA3, a transcription factor of the GATA family, has been widely explored as an IHC marker across a spectrum of neoplasms. In the context of renal tumors, our study revealed strong expression of GATA3 in both IHC sections of PRNRP specimens, a finding consistent with recent reports.4,14–16 This supports GATA3's potential as a diagnostic marker for this newly recognized WHO category. Additionally, GATA3 expression in chromophobe RCCs was variable; one showing strong positivity was associated with a hybrid oncocytic/chromophobe tumor, while 2 others showed weak positivity, implying a possible association with hybrid tumors or a distinct chromophobe RCC subset, and requires further exploration. Consistent with prior studies,17,18 GATA3 was largely absent in other common subtypes, including clear cell RCC and conventional papillary RCC.
While earlier research 3 reported significant sensitivity and specificity for GATA3 in diagnosing CCPRT, previously known as clear cell papillary RCC, our cohort shows no GATA3 positivity in any CCPRT specimens. This discrepancy may stem from several factors, including differences in IHC protocols, or inherent tumor heterogeneity within our patient population. One such scenario could be presence of low-grade oncocytic tumor (LOT) of the kidney which is suggested to be a novel tumor type recently. 19 Despite similarity to oncocytoma or eosinophilic chromophobe RCC, it shows diffuse keratin 7 IHC and negative KIT (CD117), which differs from both. Since the clinical presentation did not support that the chromo/onco hybrid tumors could be associated with SDHB (succinate dehydrogenase subunit B) mutations, no further analysis was conducted in that direction, because they are generally not associated with SDHB mutations either.
In contrast, CCPRT demonstrated strong and diffuse GLUT1 positivity in all specimens, a finding consistent with recent studies.20,21 This strong, diffuse GLUT1 expression was also observed in all PRNRP specimens. Conversely, GLUT1 staining remained negative or weakly positive in papillary RCC. Consequently, the combined use of GATA3 and GLUT1 possesses a potential diagnostic utility in differentiating papillary renal tumors.
Cyclin D1, a highly conserved protein required for cell cycle progression, is often associated with various malignancies, including urinary bladder cancer. 7 It demonstrated high positivity (in 92 out of 95 renal tumors) in this study, where only 2 specimens of chromophobe RCC and 1 RCC-nos were negative. Notably, oncocytomas exhibited strong, diffuse staining in 80%–100% of cells, while chromophobe RCCs showed weak to moderate staining in less than 50% of cells. This distinction is in agreement with a recent report showing negative cyclin D1 in chromophobe RCC and positive in oncocytoma. 8 Thus, our study supports that cyclin D1 can be a valuable addition to the diagnostic workup of renal tumors, especially when differentiating oncocytoma from chromophobe RCC as argued by earlier reports.8,22 Rather than just presence or absence, the distribution of staining, whether focal or diffuse, seems more important for interpretation.
KRT20 expression was largely absent across the renal tumors examined, with the notable exception of ESC-RCC. In these ESC-RCC specimens, all 3 samples demonstrated KRT20 positivity, with 2 showing strong, diffuse staining in 100% of cells, a finding consistent with the observations of Lobo et al, 23 thus supporting the notion that KRT20 can be useful for differentiating ESC-RCC from other renal tumors, such as oncocytoma and chromophobe RCC. Another study found that roughly one-third of ‘unclassified’ RCCs with eosinophilic cytoplasm in younger patients were reclassified as ESC-RCC, highlighting the importance of KRT20 IHC in young patients of oncocytic tumors. 24 It is noteworthy that another eosinophilic renal tumor called TFEB-altered RCC (both rearranged and amplified) also expresses KRT20, but was not present in our samples.
This study has several limitations. Firstly, as a retrospective single-institution analysis, selection bias is inherent in its design. Secondly, the extended study period, while necessary to gather sufficiently large cohort, may have introduced diagnostic variability due to evolving practices. Furthermore, the limited sample size, particularly for rare tumor subtypes, restricted statistical analysis to descriptive methods and thus limited our ability to analyze subgroup differences.
Future studies should prioritize a combined approach of molecular and integrated IHC analysis. Comprehensive molecular profiling, particularly through next-generation sequencing (NGS), is essential for accurate classification and a deeper understanding of renal tumor biology. By identifying specific genetic alterations associated with distinct kidney carcinoma subtypes, we can further refine the interpretation and application of IHC markers.
Conclusion
In conclusion, this study characterizes the IHC expression of GATA3, cyclin D1, KRT20, and GLUT1 in renal tumors, highlighting distinct patterns, largely in conformity to other such reports. Specifically, GATA3 demonstrates diagnostic potential for PRNRP, and GLUT1 shows differential expression between papillary RCC and CCPRT. Together, these markers offer significant clinical utility in subtyping papillary renal tumors. Besides, cyclin D1 may be a valuable adjunct marker to differentiate oncocytoma from chromophobe RCC, exhibiting strong, diffuse staining in oncocytomas and weak, focal staining in chromophobe RCCs. Additionally, KRT20 shows positivity in ESC-RCC, further validating its utility in distinguishing this subtype (and TFEB-altered RCC) from other RCC having mimicking morphology such as oncocytoma and chromophobe RCC. Further studies should focus on larger, multi-institutional cohorts to validate these findings. Also, future studies should investigate the molecular basis of these tumors and its correlation with a broader set of IHC findings.
Supplemental Material
sj-xlsx-1-ijs-10.1177_10668969261442121 - Supplemental material for Diagnostic Value of Immunohistochemical Markers GATA3, Cyclin D1, KRT20, and GLUT1 in Renal Neoplasms
Supplemental material, sj-xlsx-1-ijs-10.1177_10668969261442121 for Diagnostic Value of Immunohistochemical Markers GATA3, Cyclin D1, KRT20, and GLUT1 in Renal Neoplasms by Muhammad Abrar Barakzai, Shoukat Ali Arain, Nasir Ali Afsar, Yara Obaeda Alsouss and Turki Al-Hussain in International Journal of Surgical Pathology
Footnotes
Acknowledgments
The authors thank Mr Roy Abraham for his excellent technical support to conduct the experiments at KFSH&RC, Riyadh, Saudi Arabia.
ORCID iDs
Ethical Approval
The study was conducted after approval from Research Ethics Committee, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia (RAC No. 2251303).
Author Contributions
Muhammad Abrar Barakzai planned and conducted the study, obtained the research grant, wrote the manuscript and managed the project at the participating institution. Shoukat Ali Arain analyzed the data and contributed to manuscript writing. Nasir Ali Afsar analyzed the data and wrote the manuscript. Yara Obaeda Alsouss executed literature review and data collection. Turki Al-Hussain planned and conducted the study, wrote the manuscript, and supervised the project at the participating institution.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant (IRG No.22311) from Alfaisal University, Riyadh, Saudi Arabia.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.