
Abstract
Paratesticular mesothelioma is rare with limited data on its clinicopathologic and molecular characteristics. BRAF p.V600E mutation is exceptionally rare in mesotheliomas and has been reported in 5 pleural mesotheliomas to date. Herein, we reported the first paratesticular mesothelioma harboring a BRAF V600E mutation. A 44-year-old man with a history of asbestos exposure presented with painless right testicular swelling. Orchiectomy revealed a 1.5-cm biphasic mesothelioma composed of 80% sarcomatoid component admixed with 20% epithelioid component. The sarcomatoid component consisted of spindle cells in fascicular to haphazard patterns within a myxoid to collagenous stroma, while the epithelioid component showed predominantly tubulopapillary architecture. The biphasic mesothelioma expressed mesothelial markers with intact expression of BAP1, MTAP, and Merlin. Next-generation sequencing identified BRAF V600E mutation, which was also confirmed by immunohistochemistry for BRAF V600E. The patient received adjuvant chemotherapy and remained free of disease at 11 months of follow-up. This report expands the histomorphologic and molecular spectrum of paratesticular mesothelioma with the novel identification of a BRAF V600E mutation.
Introduction
Paratesticular mesotheliomas account for less than 1% of all mesotheliomas. 1 They arise from the tunica vaginalis and can infiltrate the testis and adjacent paratesticular soft tissues. Mesotheliomas are histologically classified into epithelioid, sarcomatoid (including desmoplastic), and biphasic types. 2 Biphasic mesotheliomas comprise approximately 23% of paratesticular mesotheliomas 3 and are defined by at least 10% of both epithelioid and sarcomatoid components in resection specimens. 2
BRAF p.V600E mutation is exceptionally rare in mesotheliomas and has been reported in 5 pleural mesotheliomas to date.4–6 To our knowledge, BRAF V600E mutation has not previously been described in paratesticular mesotheliomas. We herein report the first paratesticular mesothelioma harboring a BRAF V600E mutation.
Patient Presentation
A 44-year-old man presented with a 5-month history of painless right testicular swelling. The patient reported occupational asbestos exposure during his work as an electrician 14 years prior to the onset of testicular symptoms. His father, a shipyard worker, had a history of asbestosis. Scrotal ultrasonography demonstrated a large right hydrocele causing mass effect on the testis. A right hydrocelectomy performed at an outside institution revealed a malignant spindled and epithelioid neoplasm consistent with biphasic mesothelioma. Immunohistochemical (IHC) staining performed at the outside institution showed that the tumor was positive for pan-keratin AE1/AE3, WT1, calretinin (rare cells), and SMA (focal), with retained expression of BAP1, MTAP, Merlin (NF2-encoded protein), and INI1. The tumor was negative for ALK (5A4 clone), ROS1, desmin, D2-40, ERG, and SOX10.
The patient subsequently underwent orchiectomy with resection of the residual hydrocele sac at our institution one month later. Gross examination revealed a 12.5 × 10.0 × 7.5 cm cyst filled with translucent serous fluid. Adjacent to the testis was a 1.5 × 1.0 × 0.3 cm firm, white lesion. Histologically, the tumor demonstrated biphasic morphology, composed of 80% sarcomatoid component admixed with 20% epithelioid component (Figure 1A–D) within a fibrous stroma (Figure 1B, C; Figure 2C, D). The sarcomatoid component formed variably sized nodules (Figure 1A, C) and consisted of spindle cells with hyperchromasia and abundant eosinophilic cytoplasm arranged in a fascicular to haphazard pattern within a myxoid to collagenous stroma (Figure 1B–D; Figure 2A, B). Focally, the spindle cells were concentrically layered, imparting an “onion-skin” appearance (Figure 1C). The nuclei of the spindle cells ranged from bland (Figure 1D) to irregular with occasional nuclear pseudoinclusions (Figure 2A). The epithelioid component showed predominant tubulopapillary architecture (Figure 1C, D; Figure 2C, D) and was composed of cuboidal cells with minimal eosinophilic cytoplasm, oval-to-round nuclei, vesicular chromatin, and frequent nucleoli (Figure 1D). Some tubules were lined by flattened mesothelial cells (Figure 2C). Occasional signet-ring-like cells with cytoplasmic vacuoles displacing the nuclei were identified (Figure 2B, C). Vacuoles were present within the myxoid stroma (Figure 2A), and myxoid to mucinous material was focally observed within the tubule lumens (Figure 2C). Scattered psammomatous calcifications were present (Figure 2C). No mitotic figures, tumor necrosis, or lymphovascular invasion was identified. The tumor involved the tunica vaginalis, tunica albuginea, testicular parenchyma (Figure 2D), epididymis, and soft tissue adjacent to the recurrent hydrocele.

The tumor demonstrated biphasic morphology (A, 5×), composed predominantly of a sarcomatoid component (arrows in B-C, 100×, and D, 400×) admixed with epithelioid areas (B–D, arrowheads) within a fibrous stroma (B, C). The sarcomatoid component formed variably sized nodules (A, C) and consisted of spindle cells with abundant eosinophilic cytoplasm arranged in a fascicular to haphazard patterns within a myxoid to collagenous stroma (B-D, arrows). Spindle cells were focally concentrically layered, imparting an “onion-skin” appearance (C, asterisk). The epithelioid component showed predominant tubulopapillary architecture, composed of cuboidal cells with scant eosinophilic cytoplasm, oval-to-round nuclei, vesicular chromatin, and frequent nucleoli (D, arrowhead).

The sarcomatoid component showed focal nuclear pleomorphism (A, 400×, arrowheads) and occasional nuclear pseudoinclusions (A, arrows). Occasional signet-ring-like cells with cytoplasmic vacuoles displacing the nuclei were identified (arrows in B, 400×, and C, 200×). Vacuoles were also focally present within the myxoid stroma (A, asterisk). Myxoid to mucinous material was focally observed within the tubular lumens of the epithelioid component (C, triangle). Some tubules were lined by flattened mesothelial cells (C, arrowhead). Psammomatous calcifications were present (C, asterisk). The tumor exhibited fibrous stroma (C; D, 100×) and involved testicular parenchyma (D).
IHC staining performed at our institution showed that tumor cells were positive for pan-keratin AE1/AE3/CAM5.2, WT1, calretinin, and BRAF V600E (cytoplasmic) (Figure 3), with stronger expression in the epithelioid component than in the sarcomatoid component. BRAF V600E IHC staining was performed retrospectively following next-generation sequencing (NGS) results. The tumor was negative for ERG, CAMTA1, MDM2, ALK, and pan-TRK. Expression of BAP1, MTAP, and Merlin were retained in both components. Overall, the findings were characteristic of biphasic mesothelioma.

The tumor cells were positive for pan-keratin AE1/AE3/CAM5.2 (A, 400×; inset, 100×), WT1 (A), calretinin (B, 400×), and BRAF V600E (C, 400×, sarcomatoid component; D, 400×, epithelioid component; cytoplasmic).
Targeted DNA-based NGS assay, which targeted the full coding sequence of 185 cancer-associated genes, was performed on a tumor block containing both sarcomatoid and epithelioid components and revealed a pathogenic BRAF p.V600E mutation (variant allele frequency, 15%; Figure 4) and a FLT4 p.S239L variant of uncertain significance. The tumor mutation burden was low (2.5 mutations/Mb). No alterations in NF2, BAP1, or CDKN2A were identified. Targeted RNA-based NGS assay, which covered 137 commonly rearranged genes, did not detect any reportable gene fusions.
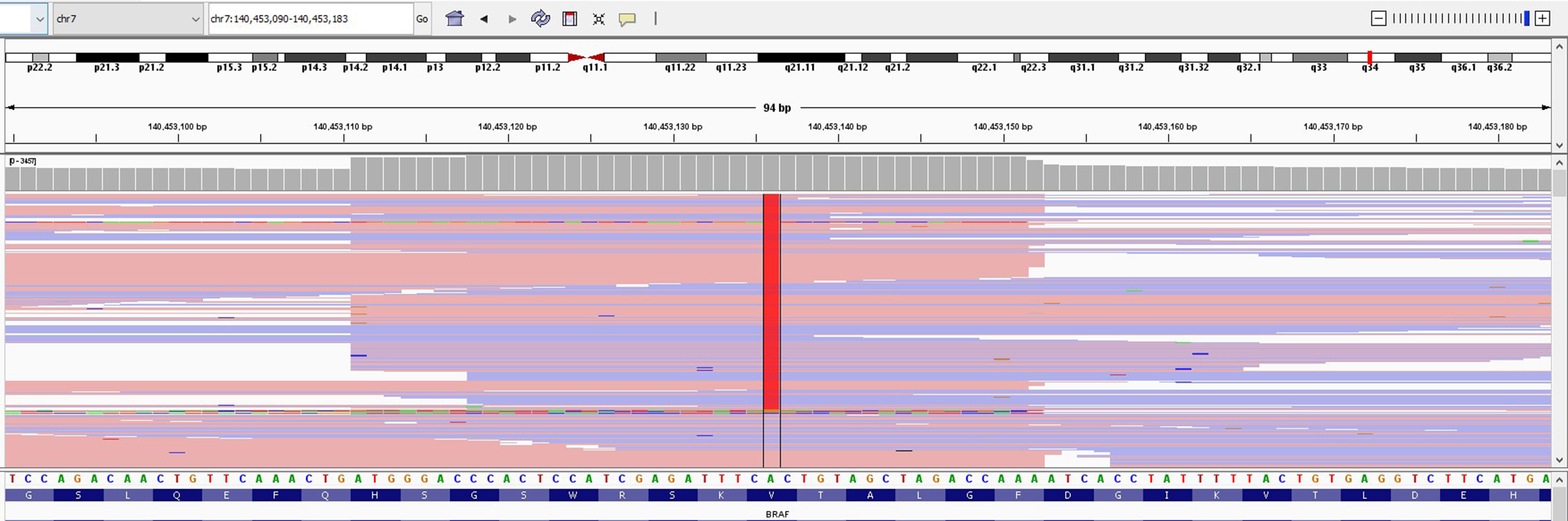
A BRAF p.V600E variant was detected by next-generation sequencing, with sequencing results at the BRAF p.V600 hotspot locus visualized here using the integrative genomics viewer (Broad Institute, Cambridge, MA, USA). Each horizontal bar represents a sequencing read, with the red bar in the center of the figure representing detection of the variant allele in those respective reads, supporting the identification of a BRAF p.V600E variant in this tumor.
The patient was treated with adjuvant chemotherapy (cisplatin and pemetrexed) after surgery. At 11 months of follow-up, he remained well with no evidence of disease.
Discussion
Paratesticular mesothelioma most commonly presents in older men. Asbestos exposure, present in the current patient, was reported in 38%, whereas smoking was reported in 4%. 3 Approximately 33% of patients died, and 9% were alive with disease at a median follow-up of 20 to 21 months. 3 Invasion of the spermatic cord or scrotum was the only identified risk factor for local recurrence, 3 and neither was observed in the present patient. Risk factors associated with metastasis included age ≥ 42 years, tumor size ≥ 49 mm, presence of necrosis, high mitotic index, angiolymphatic invasion, and local recurrence. 3 The current patient lacked all these adverse prognostic features, except for age.
BRAF V600E is a well-established oncogenic driver in several malignancies, including melanoma, colorectal carcinoma, and thyroid carcinoma, but appears to be exceptionally rare in mesotheliomas. In a cohort of 77 pleural mesotheliomas, BRAF V600E mutation was identified in only 3 tumors (3.9%; 2 epithelioid and one biphasic). 4 However, other larger genomic studies of pleural and peritoneal mesotheliomas have not reported BRAF V600E mutation.7,8 Therapeutically, a pleural biphasic mesothelioma harboring a BRAF V600E mutation demonstrated a marked clinical and radiographic response to combined BRAF and MEK inhibition with dabrafenib and trametinib, respectively, including regression of osseous metastases. 6 In another report, a patient with pleural epithelioid mesothelioma carrying a BRAF V600E mutation responded to the BRAF inhibitor vemurafenib. 5 Beyond oncogenic point mutations, rare co-amplification of BRAF have also been reported in BAP1-intact peritoneal mesotheliomas. 9
In paratesticular mesotheliomas, NF2 alterations appear to be more common, whereas BAP1 and CDKN2A alterations appear less frequently compared with pleural or peritoneal mesotheliomas.10,11 To date, BRAF V600E mutation or amplification has not been reported in paratesticular mesotheliomas. We report the first paratesticular mesothelioma harboring a BRAF V600E mutation. No alterations in NF2, BAP1, or CDKN2A were identified. The presence of oncogenic BRAF alterations in this paratesticular mesothelioma may suggest the use of BRAF-targeted therapy as a potential treatment option if there is tumor recurrence/metastasis. In diagnostically challenging paratesticular mesotheliomas, NGS-based genomic profiling may provide additional information to assist in diagnosis and guide therapeutic decision-making. BRAF IHC staining may also be helpful in the diagnostic workup when the morphology is suggestive of paratesticular mesothelioma, but Merlin and BAP1 expression are retained.
Nearly 7% of human cancers harbor BRAF alterations, more than 90% of which involve the BRAF p.V600E. 12 The BRAF V600E mutation substitutes valine at codon 600 with a negatively charged glutamate, stabilizing the activation loop and αC helix in an active conformation through formation of a Glu600-Lys507 salt bridge and resulting in a RAS-independent, constitutively active kinase monomer. 13 This alteration drives chronic MAPK/ERK signaling and induces rewiring of transcriptional programs, cellular metabolism, and telomerase regulation, collectively promoting proliferation, survival, and aggressive biology across multiple cancer types.14,15 Although the mechanistic data of BRAF V600E in mesotheliomas are limited, it likely drives tumorigenesis through mechanisms similar to those observed in other cancer types.
Among the 5 reported pleural mesotheliomas harboring BRAF V600E mutation,4–6 histologic images were available for only one tumor, which demonstrated epithelioid histology. 5 Given the limited number, it remains unclear whether mesotheliomas harboring BRAF V600E mutation are associated with characteristic morphologic features.
The most common histotype of paratesticular mesothelioma is epithelioid, followed by biphasic. 3 A higher proportion of biphasic tumors (45%) demonstrated metastatic behavior compared with epithelioid tumors (23%) in paratesticular mesotheliomas. 3 Mesotheliomas with prominent myxoid stroma, defined as comprising at least 50% of the tumor and often associated with a relatively favorable outcome, 16 represent a rare morphologic variant predominantly in epithelioid mesotheliomas, characterized by tumor cell clusters floating within myxoid pools. 17 Hyaluronic acid crystals have been identified within tumor cells of mesotheliomas with myxoid stroma by electron microscopy, supporting the concept that these tumors may retain the secretory activity of normal mesothelium. 17 Mesotheliomas with myxoid stroma may mimic other tumors including myxofibrosarcoma, 18 pseudomyxoma peritonei, 19 and ovarian sex cord-stromal tumors, 20 posing diagnostic challenges. In the current patient, the stroma associated with the sarcomatoid component was myxoid to collagenous, with the myxoid component accounting for less than 50% of the tumor. Areas of this paratesticular biphasic mesothelioma with myxoid stroma could prompt consideration of paratesticular SMARCB1/INI1-deficient epithelioid and myxoid neoplasms. 21 However, diffuse expression of mesothelial markers and retained INI1 expression excluded this differential.
The predominance of spindle cells raised the differential diagnoses of desmoplastic melanoma, inflammatory myofibroblastic tumor, and dedifferentiated liposarcoma. Although the patient had no history of melanoma, the detection of a BRAF V600E mutation raised melanoma as an important differential diagnosis. However, negative staining for SOX10, ALK/ROS1, and MDM2, the absence of detectable fusion transcripts or MDM2 amplification, together with positive WT1 and calretinin staining and the presence of tubulopapillary architecture, argued against these entities.
Occasionally present in mesotheliomas, psammomatous calcifications have been reported more frequently in peritoneal than pleural tumors, where they may mimic serous carcinoma.22,23 Psammomatous calcifications have only rarely been reported in paratesticular mesothelioma. 24 Paratesticular mesotheliomas with psammomatous calcifications such as this tumor should be distinguished from the rare paratesticular serous carcinoma with psammomatous calcifications, 25 which may also show tubulopapillary architecture and WT1 positivity. In contrast, the presence of a sarcomatoid component, as observed in the current tumor, would be unusual, and calretinin expression is typically absent in paratesticular serous carcinomas.
Cords of tumor cells with abundant eosinophilic cytoplasm embedded in a myxoid stroma, accompanied by occasional cytoplasmic vacuoles, may also mimic epithelioid hemangioendothelioma. However, IHC staining for ERG and CAMTA1 was negative; RNA-based fusion assay did not identify any reportable fusion transcripts; and the tubulopapillary architecture would be highly unusual in epithelioid hemangioendothelioma.
In conclusion, we report the first paratesticular mesothelioma harboring a BRAF V600E mutation. This tumor expands the histomorphologic and molecular spectrum of paratesticular mesothelioma and importantly, offers a clinically actionable target in this patient if recurrence or metastasis occur.
Footnotes
Ethical Approval
Approval for this study was granted by the Massachusetts General Brigham Institutional Review Board.
Informed Consent
The IRB determined that this research involved minimal risk and approved a waiver for informed consent.
Author Contributions
Project conceptualization and planning were done by TZ and MEM. Interpretation of pathology data was done by MEM, TZ, and YPH. Manuscript preparation was done by TZ. Manuscript editing were done by YPH, MEM, and TZ. Molecular figure and figure legend were done by ASF. All authors read and approved the final paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
Not applicable, because this article does not contain any clinical trials.