
Abstract
Aims
Our study investigated the clinical and pathological features of gastric solid-type poorly differentiated adenocarcinoma (PDA) along with the prognostic significance of ARID1A (AT-rich interactive domain 1A), SMARCA4, and epithelial-mesenchymal transition (EMT) markers in it.
Methods
We retrospectively evaluated 116 patients with primary gastric solid-type PDA, and patients were categorized according to deficient or proficient mismatch repair (MMR) status (51 and 65 patients, respectively). The expression of ARID1A, SMARCA4, and EMT markers (E-cadherin, β-catenin, vimentin, and SNAI1) was analyzed via immunohistochemistry, and the levels were assigned to the aberrant/retained or normal expression groups. The associations between the expression of ARID1A, SMARCA4, and EMT markers, clinicopathological characteristics, and prognostic impact were examined.
Results
Proficient MMR was associated with ARID1A-retained status (P < .001), negative E-cadherin and β-catenin, and positive SNAI1 (P = .033, P = .003, and P = .008, respectively) in contrast to deficient MMR. Log-rank analysis revealed that the combination of ARID1A-retained and SMARCA4-aberrant status indicated significantly lower disease-free survival and overall survival rates than ARID1A-aberrant and SMARCA4-retained group (P < .001, P < .001, respectively). Multivariate analysis revealed that the combination of ARID1A-retained and SMARCA4-aberrant status was an independent indicator of unfavorable prognosis (hazard ratio = 4.784, P < .001).
Conclusions
ARID1A-retained status and expression of aberrant EMT markers (E-cadherin, β-catenin, and SNAI1) are more frequently observed in proficient-MMR in solid-type PDA. ARID1A-retained and SMARCA4-aberrant status can be considered a useful indicator of unfavorable prognosis in gastric solid-type PDA.
Keywords
Introduction
Solid-type poorly differentiated adenocarcinoma (PDA) is a subtype of gastric cancer (GC) according to the Japanese Classification of GC. 1 Histologically, solid-type PDA is characterized by proliferation of cancer cells organized in solid- or sheet-like patterns with scanty stroma. Solid-type PDA has distinct clinicopathological and molecular features that include a lower-third location, expansion in growth pattern, presence of tumor-infiltrating lymphocytes, and frequent microsatellite instability (MSI).2–7 Recently, the clinicopathological characteristics and prognostic significance of the SWItch/sucrose nonfermentable (SWI/SNF) chromatin remodeling complex and epithelial-mesenchymal transition (EMT) in GC have been noticed.5–8 However, these phenomena have not been sufficiently explored in solid-type PDA.
SWI/SNF chromatin remodeling complex represents a multiprotein assembly that plays a significant role in the regulation of various functions, such as differentiation, proliferation, and DNA repair. 8 This complex comprises several submits such as SWI/SNF related BAF chromatin remodeling complex subunit ATPase 4 (SMARCA4/BRG1), SWI/SNF-related, matrix-associated, actin-dependent regulator of chromatin, subfamily B, member 1, SWI/SNF related BAF chromatin remodeling complex subunit C2, and ARID1A (AT-rich interactive domain 1A). 9 Of note, ARID1A is the most frequently detected altered chromatin remodeler gene in several types of cancer and is an integral part of gene expression regulation that promotes oncogenesis or tumor suppression.10,11 Several reports have revealed that ARID1A expression loss or downregulation is associated with cancer progression and poor prognosis in GC.12–16 However, a few reports have shown that ARID1A expression loss was not correlated with prognosis, 17 or a favorable prognosis, conversely. 18 Another SWI/SNF chromatin remodeling complex, SMARCA4/BRG1, was identified as a tumor suppressor gene that is involved in the regulation of cellular proliferation and indicates poor prognosis. 19 In GC, SMARCA4-lost GCs were associated with it because of deeper invasion. 20
EMT involves a cellular lifecycle stage, in which epitheliocytes transform into mesenchymal-like cells, leading to tumor progression. 21 EMT facilitates the downregulation of epithelial markers, such as E-cadherin, decreased membranous β-catenin expression, and aberrant upregulation of mesenchymal markers, such as vimentin. These pathways are promoted by zinc-finger transcriptional repressors such as Snail family transcriptional repressor 1 (SNAI1). 22 The loss of membranous expression of E-cadherin and abnormalities in the expression of vimentin and SNAI1 were proven to be indicative of tumor progression.22–25 Our group reported the prognostic significance of ARID1A and SMARCA4,4,5 as well as EMT markers 5 ; however, the number of patients was limited; thus, it was not sufficiently investigated on a large scale. This study aimed to elucidate the clinicopathological and prognostic significance of ARID1A, SMARCA4, and EMT markers in patients with solid-type PDA.
Materials and Methods
Patient Selection
We retrospectively recruited 116 patients with primary solid-type PDA who had been diagnosed between 2006 and 2023 and underwent surgical resection at the Department of Anatomic Pathology, including the same patients in our previous reports.4–7 We defined solid-type PDA based on the criteria of the Japanese Cancer Genome Atlas (2017) classification: cancer cells of solid-type PDA arranged in solid- or sheet-like patterns with scant stroma. Some patients exhibited secondary components, such as poorly cohesive/nonsolid-type (20/116), mucinous (5/116), papillary (3/116), and tubular adenocarcinoma (87/116), located in the tumor surface or invasive front area. The exclusion criteria were as follows: tumors with signet ring cells and special histological types, such as hepatoid adenocarcinoma and neuroendocrine carcinoma; pretreatment with neoadjuvant chemotherapy and/or radiotherapy; and Lynch syndrome. Some patients received postoperative adjuvant chemotherapy; however, none received immune checkpoint inhibitors.
Molecular Subtyping Based on The Cancer Genome Atlas Classification
The 116 patients were categorized into deficient-mismatch repair (dMMR) and proficient-MMR (pMMR) solid-type PDA. Immunohistochemistry (IHC) detection of MMR proteins (mutL homolog 1 [MLH1], postmeiotic segregation increased 2 [PMS2], mutS homolog 2 [MSH2], and mutS homolog 6 [MSH6]), multiplex polymerase chain reaction (PCR), and Epstein-Barr encoding region (EBER) in situ hybridization (ISH) were performed, according to The Cancer Genome Atlas (TCGA) molecular classification. The patients were divided into 51 dMMR and 65 pMMR, of whom none had the Epstein-Barr virus (EBV) subtype.
IHC Analysis and Evaluation
IHC staining of 4 MMR proteins (MLH1, PMS2, MSH2, and MSH6), Human Epidermal Growth Factor Receptor 2(HER2), ARID1A, SMARCA4, and EMT markers (E-cadherin, β-catenin, vimentin, and SNAI1) was performed. Supplemental Table 1 presents the primary antibodies used. IHC was performed as previously described. 7 Four MMR proteins (MLH1, PMS2, MSH2, and MSH6) were considered as “complete loss” when nuclear staining in tumor cells was completely absent. The internal positive control was stromal cells. dMMR was defined as one or more MMR proteins with complete loss in tumor cells. pMMR was defined as retention of all 4 MMR proteins. HER2 expression with strong complete or basolateral membranous staining in ≥10% of the neoplastic cells was considered as positive.
For the immunostaining of ARID1A and SMARCA4, the proportion of nuclear staining of cancer cells was evaluated and compared with that of infiltrating lymphocytes, fibroblasts, vascular endothelial cells, and the control represented by normal gastric epithelial cells. Staining proportions were graded as complete loss (0%-4%), partial loss (5%-49%), or retained (50%-100%), where the former 2 were outlined as “aberrant” expression, as previously described.4,5 Figure 1A to F show the representative images of ARID1A (A, complete loss; B, partial loss; and C, retained) and SMARCA4 (D, complete loss; E, partial loss; and F, retained).

Representative immunohistochemical images of ARID1A (A, complete loss [0%-4%]; B, partial loss [5%-49%]; and C, retained [50%-100%]) and SMARCA4 (D, complete loss [0%-4%]; E, partial loss [50%-100%]; and F, retained [50%-100%]) in solid-type PDA. Abbreviations: ARID1A, AT-rich interactive domain 1A; PDA, poorly differentiated adenocarcinoma.
For immunostaining of EMT markers (E-cadherin, β-catenin, vimentin, and SNAI1), distinct membranous staining for E-cadherin and β-catenin, cytoplasmic staining for vimentin, and nuclear staining for SNAI1 were analyzed based on previously reported criteria. 5 In assessing the membranous expression of E-cadherin, the expression proportion was classified into 2 groups according to grading: negative (0%-66%) and positive (>66%). The membranous expression of β-catenin and E-cadherin was evaluated, with negative (0%-66%) and positive (>66%) grades. For vimentin, cytoplasmic expression proportions were categorized into 2 grades: negative (0%-9%) and positive (≥10%). For SNAI1, nuclear expression proportions were categorized into 2 grades: negative (0%-19%) and positive (≥20%). We also evaluated the combinations of these 4 EMT markers. The combination of positive E-cadherin and β-catenin along with negative vimentin and SNAI1 was outlined as the “normal” pattern, whereas others were defined as “aberrant” patterns. Supplemental Figure 1G to N present the representative images of E-cadherin (G, negative and H, positive), β-catenin (I, negative and J, positive), vimentin (K, negative and L, positive), and SNAI1 (M, positive and N, negative). Each sample was subjected to blind analysis by 3 independent pathologists (SU, DK, and KK). In case of disagreement, the slides were re-evaluated by the 3 pathologists to reach a final decision.
Microsatellite Instability Analysis for Multiplex PCR
Microsatellite status was assessed by analyzing DNA extracted from formalin-fixed, paraffin-embedded tumor tissue sections using an MSI Analysis Kit (FALCO) (FALCO biosystems) with 5 mononucleotide repeat markers (BAT25, BAT26, NR21, NR24, and MONO27). PCR was performed by a Veriti thermal cycler (Life Technologies), and the PCR amplicon was diluted by distilled water and applied to a 3130xl Genetic Analyzer (Life Technologies). Fragment analysis was carried out by using GeneMapper software (Life Technologies). Tumors showing markers outside the corresponding Quasi-Monomorphic Variant Region were defined as MSI. We classified MSI-High if 2 or more of the 5 markers showed MSI, and negative (MSI-Low or MSS) if one marker or less showed MSI.
Statistical Analysis
All statistical analyses were performed using JMP Statistical Discovery Software (version Pro 17; SAS Institute, Cary, NC, USA). Pearson chi-square, Fisher exact, or Wilcoxon tests were used to analyze the obtained data. Disease-free survival (DFS) was defined as the period from the time of surgery to the date of detection of a new lymph node, distal metastasis, or last follow up, eliminating 5 patients, in which pathological stage IV was diagnosed. Overall survival (OS) was defined as the period from the time of surgery until the last follow up or death from GC. Survival curves were constructed using Kaplan-Meier analysis and were statistically analyzed using the log-rank test. The Cox proportional hazards regression model was developed for univariate and multivariate analyses of the factors associated with OS and DFS. P-values <.05 were used to denote statistical significance.
Results
Molecular Subtyping of Solid-Type PDA Based on TCGA Classification
IHC of the 4 MMR proteins (MLH1/PMS2/MSH2/MSH6), multiplex PCR, and EBER-ISH revealed 2 GC subtypes in all 116 patients (dMMR solid-type PDA [n = 51] and pMMR solid-type PDA [n = 65]) according to MMR expression status, with no EBV-subtype present. Supplemental Table 2 presents the outcomes of IHC of MMR proteins and EBER-ISH. All 51 dMMR patients were characterized by a concomitant loss of MLH1/PMS2. The expression of MSH2 and MSH6 was maintained in all patients. Multiplex PCR revealed that 42 of the 51 dMMR patients were MSI-high. Overall, in 9 of the 51 patients, multiplex PCR could not be applied because of low DNA quality or the level of PCR amplification.
Correlation Between MMR Status and Clinicopathological Characteristics/Prognosis
To validate the clinicopathological significance of MMR status, we investigated the correlation between MMR status and clinicopathological characteristics/prognosis. A significant correlation was found between dMMR status and older age (P < .001), female sex (P < .001), lower third location (P < .001), no vascular invasion (P = .005), HER2 negativity (P = .034), and absence of postoperative adjuvant chemotherapy (P = .024) (Supplemental Table 3). The log-rank test revealed that patients with pMMR status had significantly lower DFS (P = .005) and OS (P = .004) rates than those with dMMR (Supplemental Figure 2A and 2B).
Differences in ARID1A, SMARCA, and EMT Markers According to MMR Status
The expression of ARID1A, SMARCA4, and EMT markers (E-cadherin, β-catenin, vimentin, and SNAI1) was compared between the dMMR and pMMR groups (Table 1). The pMMR group had a significantly more frequently retained ARID1A expression than the dMMR group (P < .001). The expression of SMARCA4 did not significantly differ between the dMMR and pMMR groups (P = .101). Regarding the EMT markers, the pMMR group exhibited a significantly higher frequency of negative E-cadherin and β-catenin along with positive SNAI1 (P = .033, P = .003, and P = .008, respectively) than the dMMR group.
Association Between MMR status and ARID1A, SMARCA4, E-Cadherin, β-Catenin, Vimentin, and SNAI1 of 116 Solid-Type Poorly Differentiated Adenocarcinomas.
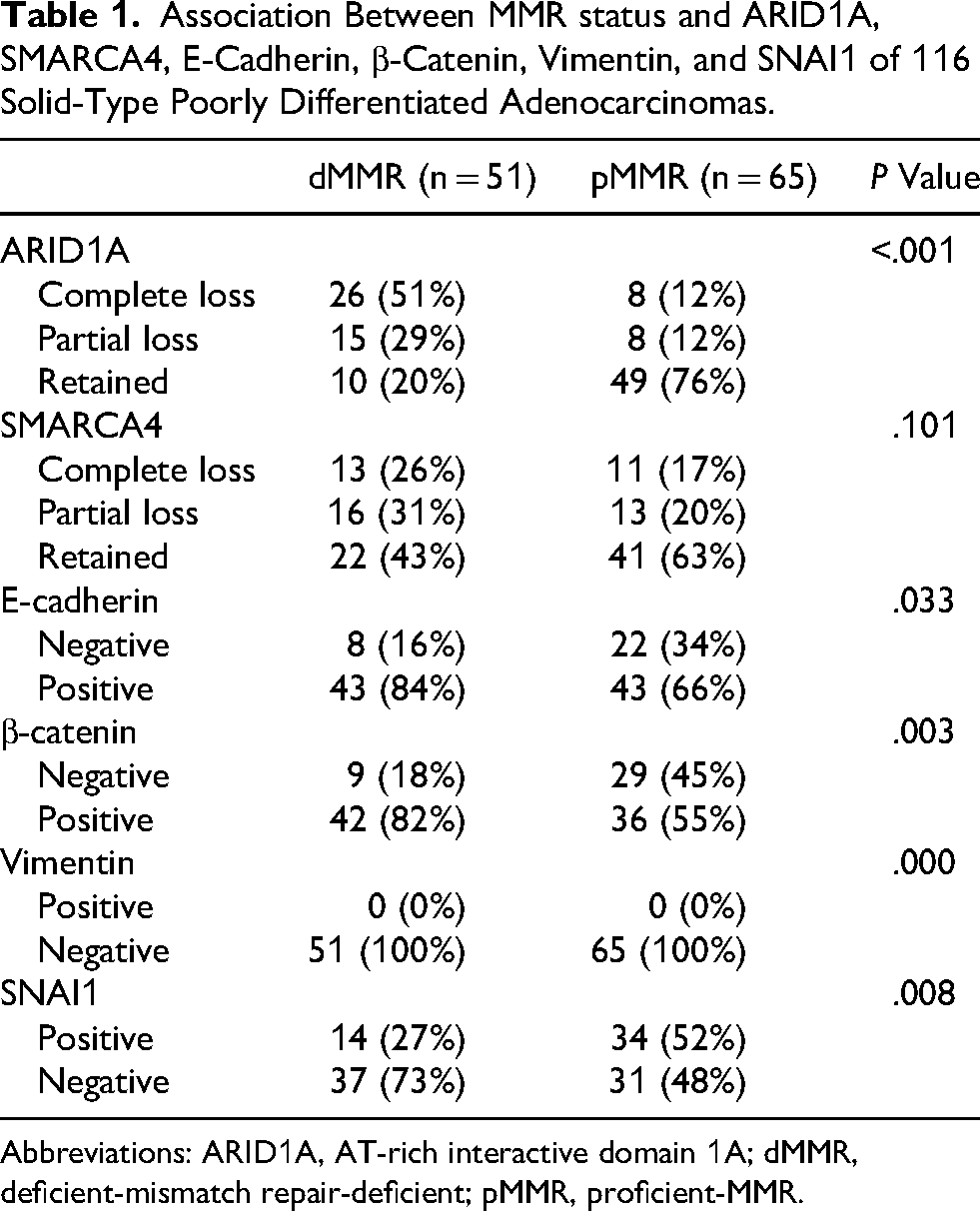
Abbreviations: ARID1A, AT-rich interactive domain 1A; dMMR, deficient-mismatch repair-deficient; pMMR, proficient-MMR.
Association Between Clinicopathological Characteristics/Prognosis and ARID1A or SMARCA4 Status
The association between ARID1A and SMARCA4 status and clinicopathological characteristics/prognosis was evaluated. We found that ARID1A-retained status was positively correlated with younger age (P = .046), male sex (P = .008), middle and upper locations (P = .023), presence of vascular invasion (P = .015), and postoperative adjuvant chemotherapy in medical anamnesis (P = .015) (Supplemental Table 4). The log-rank test revealed that ARID1A-retained status was significantly associated with lower OS rate than ARID1A-aberrrant status (P = .002) (Figure 2A). We also detected that SMARCA4-aberrant status was associated with a higher pathological stage (P = .007) (Supplemental Table 5). The log-rank test revealed a significant correlation between SMARCA4-aberrant status and lower OS (P = .037) (Figure 2B).
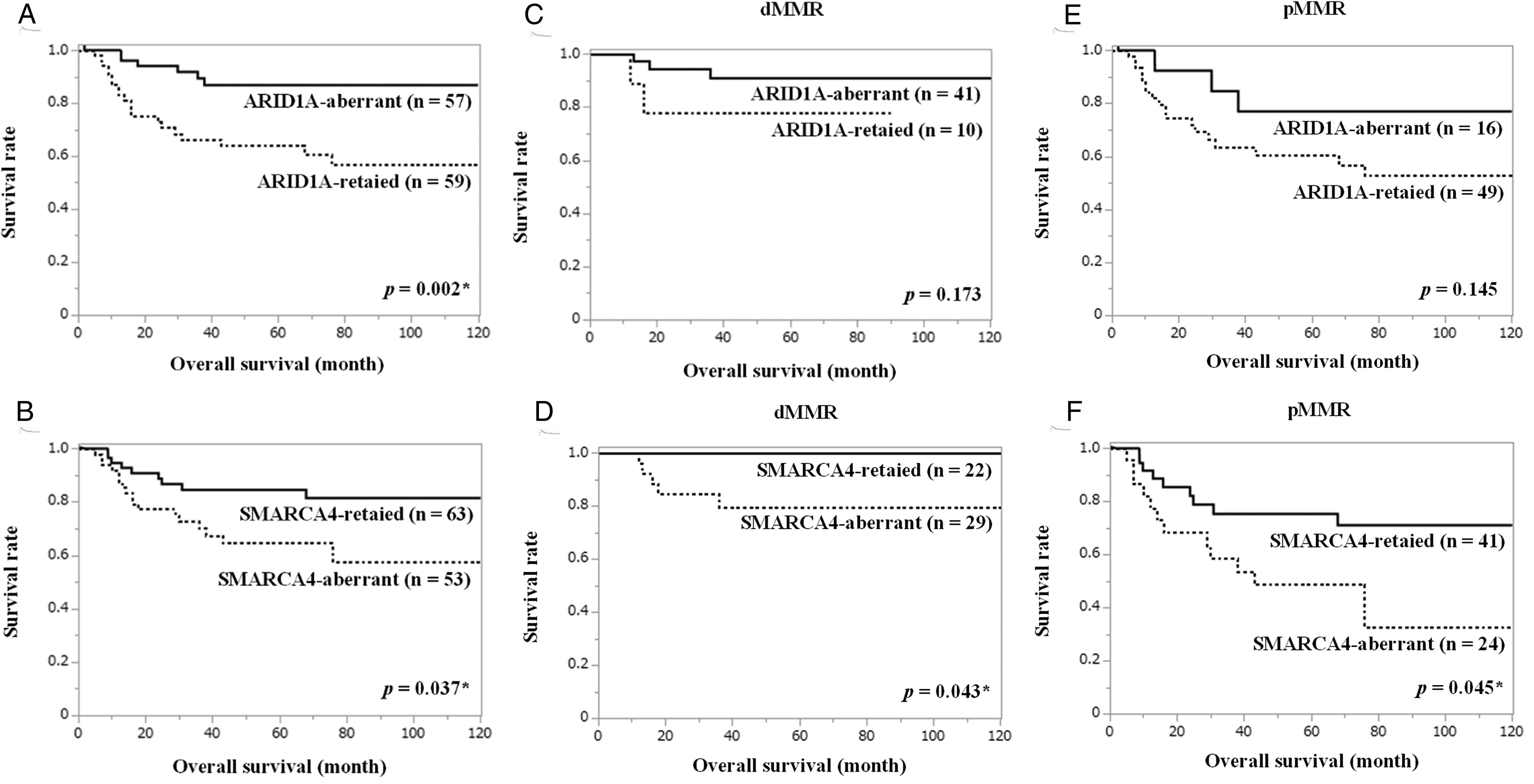
Kaplan-Meier curves of overall survival in ARID1A (A, C, and E) and SMARCA4 (B, D, and F) status in the dMMR (C and D) and pMMR (E and F) groups in solid-type PDA. (A) ARID1A-retained status was associated with significantly lower OS than ARID1A-aberrant status (P = .002). (B) SMARCA4-aberrant status was more significantly correlated with lower OS than SMARCA4-retained status (P = .037). (C) In the dMMR group, no significant association was observed between ARID1A-retained and ARID1A-aberrant status (P = .173). (D) In the dMMR group, SMARCA4-aberrant status was more significantly correlated with lower OS than SMARCA4-retained status (P = .043). (E) In the pMMR group, no significant association was observed between ARID1A-retained and ARID1A-aberrant status (P = .145). (F) In the pMMR group, SMARCA4-aberrant status was more significantly associated with lower OS than SMARCA4-retained status (P = .045). Abbreviations: ARID1A, AT-rich interactive domain 1A; dMMR, deficient-mismatch repair; OS, overall survival; PDA, poorly differentiated adenocarcinoma; pMMR, proficient-MMR.
Association Between EMT Markers Status and Clinicopathological Characteristics/Prognosis
The association between EMT markers (E-cadherin, β-catenin, and SNAI1) and clinicopathological characteristics/prognosis was examined. No correlation was observed between E-cadherin status and clinicopathological characteristics (Supplemental Table 6). The log-rank test revealed no significant differences in OS between E-cadherin-positive and E-cadherin-negative patients (P = .673) (Figure 3A). Negative β-catenin and male sex were significantly associated (P = .005) (Supplemental Table 7). The findings of the log-rank test revealed that OS rates did not differ significantly between β-catenin-positive and β-catenin-negative patients (P = .131) (Figure 3B). SNAI1 status and clinicopathological characteristics were not associated (Supplemental Table 8). The log-rank test revealed no significant differences between SNAI1-positive and SNAI1-negative patients in terms of OS (P = .685) (Figure 3C).
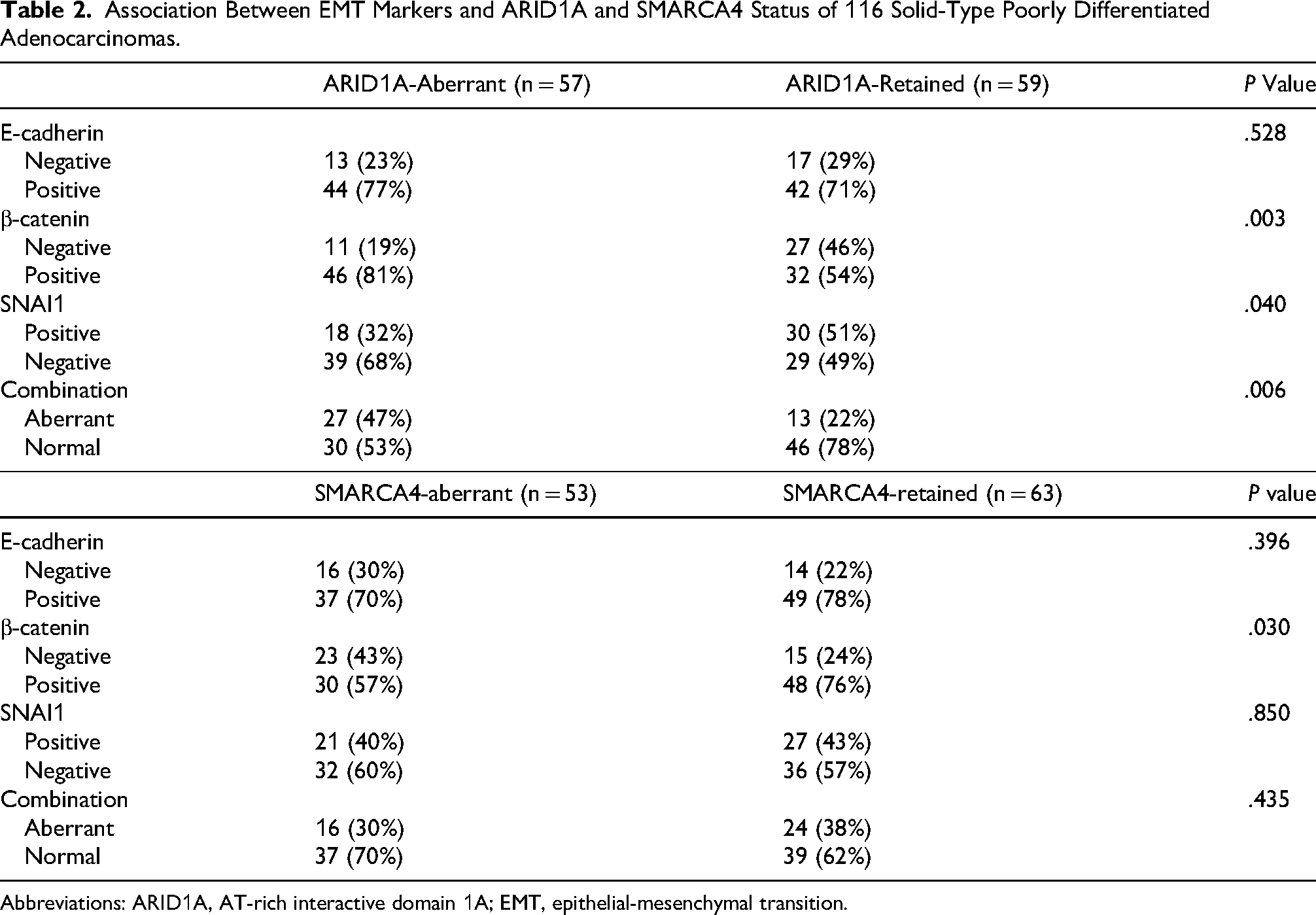
Association Between EMT Markers and ARID1A- and SMARCA4-Aberrant/Retained Status in Solid-Type PDA
Correlations were comparatively evaluated between EMT markers (E-cadherin, β-catenin, and SNAI1) and ARID1A- and SMARCA4-aberrant/retained status (Table 2). The ARID1A-retained group exhibited a higher prevalence of negative β-catenin, positive SNAI1, and aberrant combination patterns of EMT markers (P = .003, P = .040, and P = .006, respectively) than the ARID1A-aberrant group. The SMARCA4-aberrant group exhibited a higher frequency of negative β-catenin (P = .030).
Survival Analysis of the ARID1A and SMARCA4 Status in the dMMR and pMMR Groups
The prognostic significance of ARID1A and SMARCA4 in the dMMR and pMMR groups was compared. The log-rank test revealed no significant correlation between OS and ARID1A status in the dMMR (P = .173) and pMMR (P = .145) groups (Figure 2C and E). SMARCA4-aberrant status was significantly associated with a lower OS rate than SMARCA4-retained status in the dMMR (P = .043) and pMMR groups (P = .045) (Figure 2D and F).
Survival Analysis of the EMT Markers Status in the dMMR and pMMR Groups
The prognostic significance of EMT markers (E-cadherin, β-catenin, and SNAI1) in the dMMR and pMMR groups was investigated. The log-rank test revealed that OS was not significantly correlated with E-cadherin in the dMMR (P = .767) and pMMR (P = .740) groups (Supplementary Figure 3A and B), with β-catenin in the dMMR (P = .878) and pMMR (P = .587) groups (Supplementary Figure 3C and D), or with SNAI1 in the dMMR (P = .141) and pMMR (P = .573) groups (Supplementary Figure 3E and F).
Survival Analysis of the Combination of ARID1A and SMARCA4 Status
The association between the combination of ARID1A and SMARCA4 and prognosis was evaluated. The log-rank test revealed that the DFS and OS rates of ARID1A-retained/SMARCA4-aberrant patients were significantly lower than those of ARID1A-aberrant/SMARCA4-retained patients (P < .001, P < .001, respectively) (Figure 4A and B).
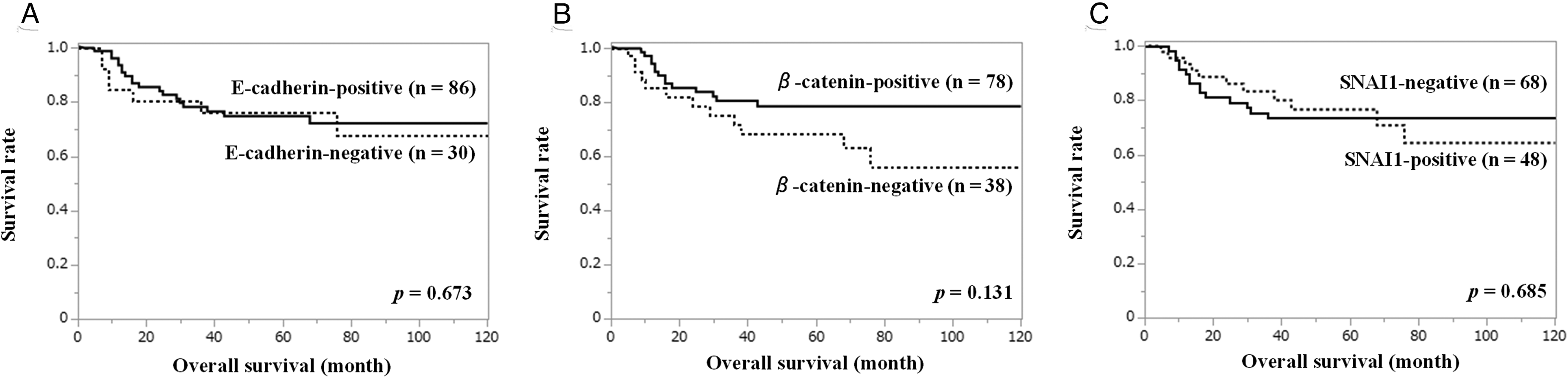
Kaplan-Meier curves of overall survival constructed based on E-cadherin (A), β-catenin (B), and SNAI1 (C) status of patients with solid-type PDA. (A) No significant correlation was observed between E-cadherin-negative and E-cadherin-positive status (P = .673). (B) No significant association was observed between β-catenin-negative and β-catenin-positive status (P = .131). (C) No significant correlation was observed between SNAI1-positive and SNAI1-negative status (P = .685). Abbreviations: PDA, poorly differentiated adenocarcinoma.
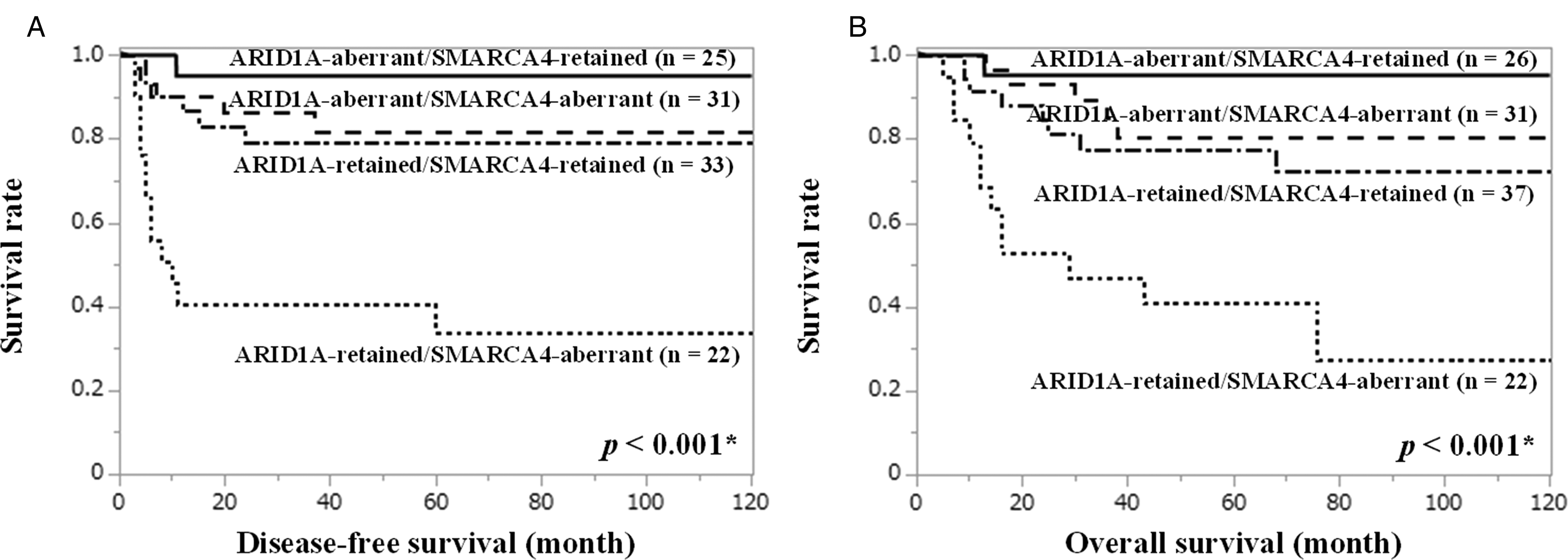
Survival analysis of the combination of ARID1A and SMARCA4 status in patients with solid-type PDA. (A) ARID1A-retained/ARID1A-aberrant status was significantly associated with lower disease-free survival than ARID1A-aberrant/SMARCA4-retained status (P < .001). (B) ARID1A-retained/ARID1A-aberrant status was significantly associated with lower overall survival than ARID1A-aberrant/SMARCA4-retained status (P < .001). Abbreviations: ARID1A, AT-rich interactive domain 1A; PDA, poorly differentiated adenocarcinoma.
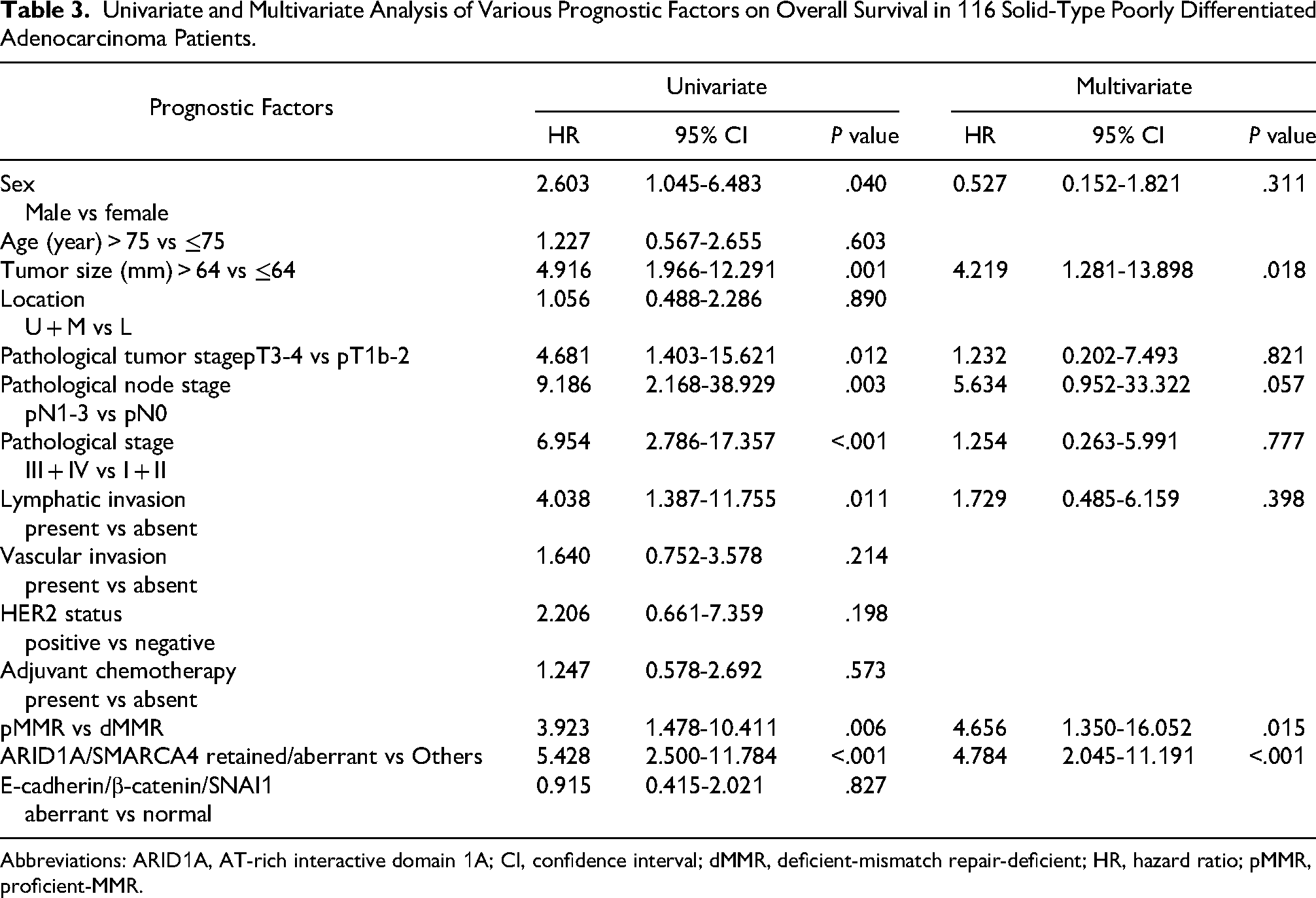
Outcomes of Univariate and Multivariate Analyses
To determine independent predictors of solid-type PDA, univariate and multivariate analyses were performed. The univariate analysis revealed a significant association between decreased OS and male sex, tumor size, high pathological tumor stage, pathological node stage, pathological stage, lymphatic invasion, pMMR status, and ARID1A-retained/SMARCA4-aberrant status. The multivariate analysis revealed that tumor size (hazard ratio = 4.219, P = .018), pMMR status (hazard ratio = 4.656, P = .015), and ARID1A-retained/SMARCA4-aberrant status (hazard ratio = 4.784, P < .001) had a significant effect on OS (Table 3).
Association Between EMT Markers and ARID1A and SMARCA4 Status of 116 Solid-Type Poorly Differentiated Adenocarcinomas.
Abbreviations: ARID1A, AT-rich interactive domain 1A; EMT, epithelial-mesenchymal transition.
Univariate and Multivariate Analysis of Various Prognostic Factors on Overall Survival in 116 Solid-Type Poorly Differentiated Adenocarcinoma Patients.
Abbreviations: ARID1A, AT-rich interactive domain 1A; CI, confidence interval; dMMR, deficient-mismatch repair-deficient; HR, hazard ratio; pMMR, proficient-MMR.
Discussion
This study demonstrated the clinicopathological and prognostic significance of ARID1A, SMARCA4, and EMT markers in solid-type PDA. We exhibited that ARID1A-retained status was significantly more frequently observed in the pMMR group than in the dMMR group. The prevalence of negative E-cadherin and β-catenin and positive SNAI1 was significantly higher in the pMMR group than in the dMMR group. Aberrant expression of EMT markers was more prevalent in the ARID1A-retained and SMARCA4-aberrant groups than in the ARID1A-aberrant and SMARCA4-retained groups. The log-rank test proved that ARID1A-retained and SMARCA4-aberrant status were associated with significantly lower OS rates than ARID1A-aberrrant and SMARCA4-retained status. The specific combination of ARID1A and SMARCA4 status was also detected to be important, with ARID1A-retained/SMARCA4-aberrant status being associated with significantly lower OS rates than ARID1A-aberrant/SMARCA4-retained status. To the best of our knowledge, this is the first report to show that ARID1A-retained/SMARCA4-aberrant status is an independent indicator of unfavorable prognosis in patients with solid-type PDA. Therefore, the evaluation of ARID1A and SMARCA4 expression in cancer cells is important to determine a reliable prognosis in this category.
This study exhibited that aberrant expression of ARID1A was detected in 49% of the 116 solid-type PDA patients. The proportion of aberrant expression of ARID1A was higher than that in previous reports (between 8% and 27% of GC).17,26,27 This is believed to be associated with the high prevalence of dMMR status, which leads to a high mutation burden. 11 Furthermore, the proportion of SMARCA4-aberrant status was higher (46% of the 116 solid-type PDA patients) than that observed in previous reports (2%-10% in GC).20,28,29 The possible reason is that ARID1A mutations affect SMARCA4 alterations. 20 However, the mechanism underlying aberrant SMARCA4 expression in solid-type PDA remains unclear and requires further investigation.
The observed prognostic significance of ARID1A was consistent with that observed in our previous report,4,5 in which patients with ARID1A-retained status had poor prognosis. However, in other study groups, the retained expression of ARID1A in GC was associated with favorable prognosis.13–15 This difference can be explained by the specificity of our study cohort, which was characterized by a high proportion of pMMR status in ARID1A-retained patients (Table 1). In GC, pMMR status was more indicative of unfavorable prognosis than dMMR in general, 7 and this may have led to poor clinical outcomes in ARID1A-retained solid-type PDA.
We exhibited for the first time that SMARCA4-aberrant patients were associated with poor prognosis compared with SMARCA4-retained patients and the dMMR and pMMR groups in solid-type PDA. The prognosis of patients with GC expressing SMARCA4 has rarely been reported in small cohorts. Altered SMARCA4 expression was reported to be an unfavorable prognostic factor,20,30 which is consistent with the outcomes of our study.
These data support the results that the combination of ARID1A-retained/SMARCA4-aberrant status is a predictor of unfavorable prognosis in solid-type PDA. In clinical practice, investigating ARID1A and SMARCA4 together is important for predicting prognosis. In ARID1A-retained/SMARCA4-aberrant status, more careful follow-up and intensified treatment will be desired compared to the other status of ARID1A and SMARCA4.
We examined the relationship between EMT markers and prognosis of solid-type PDA. Our study exhibited for the first time that EMT marker abnormalities were significantly more frequent in the pMMR group than in the dMMR group, which may be associated with higher malignancy in the pMMR group. Furthermore, we investigated the relationship between the expression of EMT markers and the expression of ARID1A and SMARCA4. Previous study showed the correlation between ARID1A and E-cadherin down regulation and subcellular redistribution of β-catenin, enhancing GC cell migration. 31 In our report, ARID1A-retained and SMARCA-aberrant status are associated with aberrant expression of EMT markers, which is almost consistent with a previous report. 5 These findings indicate that EMT contributes to tumor aggressiveness in pMMR, ARID1A-retained, and SMARCA4-aberrant solid-type PDA.
This study has several limitations that should be considered. In addition to the retrospective study design, we could not evaluate DNA alterations or the mRNA expression of ARID1A and SMARCA4 using molecular biological methods. We could not evaluate the expression of the nonsolid components because of the smaller range compared with the solid components. In the future, comparing the gene expression of ARID1A-retained/SMARCA4-aberrant status and the other status will be desirable.
Conclusions
ARID1A-retained status and aberrant expression of EMT markers (E-cadherin, β-catenin, and SNAI1) are more frequently observed in proficient-MMR than in deficient-MMR in solid-type PDA. ARID1A-retained and SMARCA4-aberrant status can be a useful prognostic indicator of unfavorable outcomes in solid-type PDA.
Supplemental Material
sj-tif-1-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-tif-1-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Supplemental Material
sj-tif-2-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-tif-2-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Supplemental Material
sj-tif-3-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-tif-3-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Supplemental Material
sj-docx-4-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-docx-4-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Supplemental Material
sj-docx-5-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-docx-5-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Supplemental Material
sj-docx-6-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-docx-6-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Supplemental Material
sj-docx-7-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-docx-7-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Supplemental Material
sj-docx-8-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-docx-8-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Supplemental Material
sj-docx-9-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-docx-9-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Supplemental Material
sj-docx-10-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-docx-10-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Supplemental Material
sj-docx-11-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-docx-11-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Supplemental Material
sj-docx-12-ijs-10.1177_10668969261449480 - Supplemental material for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study
Supplemental material, sj-docx-12-ijs-10.1177_10668969261449480 for ARID1A-Retained and SMARCA4-Aberrant Gastric Solid-Type Poorly Differentiated Adenocarcinoma and Prognosis: A Retrospective Cohort Study by Shinya Umekita, Daisuke Kiyozawa, Shinichiro Kawatoko, Taisuke Sasaki, Eikichi Ihara and Kenichi Kohashi in International Journal of Surgical Pathology
Footnotes
Acknowledgments
We thank all the technical staff of the Department of Pathology, Kyushu University, for assisting with the study.
Ethical Consideration
All procedures were followed in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. The study was approved by the Medical Human Investigation Committee of Kyushu University (institutional Review Board no. 2020-476).
Consent to Participate
Informed consent to be included in the study, or the equivalent, was obtained from all the patients.
Author Contributions
SU conducted the research and wrote the paper. DK and KK contributed to the research design and slide review. SK, TS, and EI contributed to the sample collection and research design. SK designed the research and provided the final approval of the manuscript. All authors critically reviewed and approved the manuscript. SK, who is the guarantor, is responsible for the overall content of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by JSPS KAKENHI (grant number: 21K06887).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data generated in the present study may be requested from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.