
Abstract
Objective
Lung squamous cell carcinomas (LSCC) currently lack a standardized histopathological grading system, unlike their adenocarcinoma counterparts. In this retrospective study, we examined the prognostic significance and classification value of tumor budding (TB), single-cell invasion, tumor budding nest size (TBNS) grading system, and spread through airspaces (STAS).
Methods
About 268 patients who underwent surgical resection for LSCC between November 2011 and December 2021 were evaluated. TB was assessed in hematoxylin and eosin-stained sections at ×200 magnification from the area showing the most prominent budding activity. A 3-tier TBNS grading system was established by combining the number of tumor buds and the size of tumor cell nests. STAS presence was also evaluated.
Results
Our analysis revealed significant associations between high TBNS scores and adverse pathological features, including higher tumor stage, pleural and lymphovascular invasion, increased stromal fibrosis, and lymph node metastasis. Furthermore, survival analysis demonstrated that high TB, single-cell invasion, elevated TBNS scores, and the presence of STAS were all linked to reduced overall and disease-free survival (P < .005).
Conclusion
These findings suggest that TB, TBNS, and STAS are valuable histopathological markers that may offer additional prognostic insight beyond traditional staging parameters. Incorporating a standardized assessment of these features into routine pathology reports could improve prognostic stratification and inform clinical decision-making in patients with LSCC.
Keywords
Introduction
Lung carcinomas are the most common types of cancer that lead to death in men and women. 1 In the current World Health Organization (WHO) classification of lung carcinomas, squamous cell carcinomas (SCC) are classified as keratinizing, nonkeratinizing, and basaloid subtypes; nevertheless, these have not been shown to have prognostic or other clinical significance. 2 The latest WHO classification provides a classification for lung adenocarcinomas based on histological subtypes that are important for prognosis. A universally accepted grading system for lung SCC is still not available. The prognosis of lung adenocarcinomas is largely guided by the predominant histological growth patterns, as recommended by the International Association for the Study of Lung Cancer (IASLC). 2 Additional prognostic factors, such as spread through airspaces (STAS), have also been recognized and are increasingly included in histopathological reports. 3
In lung SCC, tumor size and lymph node status are staged according to the 8th edition of the American Joint Committee on Cancer (AJCC) staging system. 4 However, given the heterogeneity in clinical outcomes, there is increasing interest in identifying additional histopathological features that could serve as prognostic indicators. Among these, tumor budding and tumor cell nest size have recently gained attention. 5
Tumor budding is defined as the presence of isolated single tumor cells or small clusters composed of fewer than 4 tumor cells at the invasive tumor front. 6 Initially described and validated in colorectal cancers through the International Tumor Budding Consensus Conference (ITBCC) in 2016. 6 Tumor budding has since been studied as a prognostic marker in various malignancies, with several publications confirming its adverse prognostic impact.7–9
In addition, studies on different solid organ tumors such as oral SCC, 10 pancreatic adenocarcinoma, 11 gastric adenocarcinoma, 12 and cervical SCC13,14 have shown that tumor budding is an important prognostic feature, indicating low survival rate and early disease recurrence.
Our aim in this study is to evaluate the presence of keratinization, degree of fibrosis, tumor budding and severity, tumor cell nests in the tumor that we can use for histological grading, and to compare these findings with other clinicopathological parameters such as diameter, age, tumor diameter, perineural and lymphovascular invasion, and lymph node involvement, presence of STAS.
Material and Methods
Patient Selection and Data Collection
In this study, a total of 283 patients who underwent surgical resection of lung tumors and were diagnosed with SCC between June 2011 and May 2020 were included. Fifteen patients with unavailable slides or clinical data were excluded, and finally, a total of 268 patients were evaluated. All available hematoxylin and eosin (H&E) stained slides were reviewed by 2 pathologists (NU and NAF) who were blinded to clinicopathological and clinical information, using an Olympus BX46 microscope (Olympus, Tokyo, Japan) with a standard 22-mm-diameter eyepiece.
The degree of fibrosis of the tumor stroma was assessed in the mild (<25% of the whole tumor area), moderate (25%-50%), and severe (>50%) groups. 15 It was determined microscopically whether there is STAS (Figure 1D). The clinicopathological parameters were obtained from the archive and re-examined under a light microscope.

Parameters and Examples of Their Levels in Histopathological Examination of Patients. (A) Low Tumor Budding (H&E, ×200). (B) High Tumor Budding (H&E, ×200). (C) Single Cell Invasion (Cells—Arrow, H&E, ×200). (D) Spread Through Airspaces (STAS) in AQ8 Patients With Squamous Cell Carcinoma (STAS—Arrow, H&E, ×200).
Tumor Budding and the Cell Nest Size
The tumor budding was defined as a single tumor cell or a group of ≤4 tumor cells present at the infiltrating edge of the malignant tumor and divided into 3 groups: without (1 point), low (1-14 budding, 2 points) (Figure 1A), and high (≥15 budding, 3 points) (Figure 1B). Tumor budding was assessed in 10 fields of 0.24 mm2 each. 1-2 points were indicated as low activity, and 3 points as high budding activity. The highest bud counts were analyzed individually within a single field (0.24 mm2). All evaluations were performed using a field area of 0.24 mm2 at ×400 magnification. The cell nest size was defined as a minimal size of invasive tumor cell nests and divided into 4 groups: large (>15 cells, 1 point), medium (5-15 cells, 2 points), small cell nests (2-4 cells, 3 points), and single cell invasion (4 points) (Figure 1C).
Tumor budding and cell nest size were evaluated for each patient, and the total score derived from these 2 parameters was used to assign a grade according to a 3-tiered system, herein referred to as the “tumor budding and nest size” (TBNS) grading system.14,16 Then, the total scores were derived by adding tumor budding activity (1-3 points) and cell nest size (1-4 points) scores. This grading system was categorized as G1 (well differentiated, total score 2 or 3), G2 (moderately differentiated, total score 4 or 5), and G3 (poorly differentiated, total score 6 or 7).
For evaluation of tumor budding, all slides were reviewed independently by 2 experienced Pathologists (NÜ, NAF).
STAS
STAS in non-small cell lung cancer (NSCLC), introduced into the 2015 WHO classification, is defined as the spread of micropapillary cluster, solid nest, and/or single cancer cells into airspaces in the lung parenchyma beyond the edge of the primary tumor. 17 A large number of independent studies have confirmed that STAS is a predictor of recurrence and poor survival in lung adenocarcinoma.18–20
The International Association for the Study of Lung Cancer Staging stated that STAS should be included as a histological descriptor in the 9th Edition of the TNM classification of lung cancer. 20
The presence of STAS is an easier and more understandable definition for the subtypes of lung adenocarcinomas. However, in the literature, a small number of studies have studied STAS in lung SCC.20–23
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics, Version 22.0 (SPSS Inc., Chicago, USA). Correlation between groups for categorical variables was assessed using Chi-square (Pearson Chi-square) and Fisher's Exact Test. Clinicopathological prognostic variables were investigated using univariate and multivariate Cox regression analysis to estimate disease-free survival and overall survival. The Kaplan-Meier method was used for survival analysis and evaluated with the log-rank test. A P-value of < .05 was accepted as statistically significant.
Ethical Approval
This study was approved by the Clinical Research Ethics Committee of the Istanbul Yedikule Chest Disease and Thoracic Surgery Training and Research Hospital (2021-94).
Results
Clinicopathological Characteristics
The ages of the 268 patients included in the study ranged from 40 to 81 years, with an average age of 62.4 years. About 253 (94.4%) of the patients were male, and 15 (5.6%) were female. Tumor diameters were 1 to 12 cm, and the average diameter in resection materials was 4.6 cm. Histopathological evaluation of the tumors reported 10 (3.7%) basaloid SCC, 84 (31.3%) nonkeratinizing, and 174 (65%) keratinizing SCC. Pleural invasion was detected in 60 (22.4%) (PL1 n = 29 (48.3%), PL2 n = 7 (11.7%), PL3 n = 24 (40%)), lymphovascular invasion was detected in 156 (58.2%) patients, perineural invasion in 98 (36.6%) patients, and necrosis in 181 (67.5%) patients. High budding activity was observed in 149 patients (55.6%), while single cell invasion was observed in a total of 104 patients (38.8%). Lymph node involvement was detected in 124 (46.2%) patients, and STAS were detected in 186 (69.4%) patients. When evaluated according to the degree of fibrosis, mild fibrosis was detected in 25 (9.3%) patients, moderate fibrosis in 108 (40.3%) patients, and severe fibrosis in 135 (50.4%) patients. The other clinicopathological features of the patients are summarized in Table 1.
Correlation of Tumor Budding, Cell Nest Size, and TBNS System With Clinicopathological Parameters in Lung Squamous Cell Carcinoma.
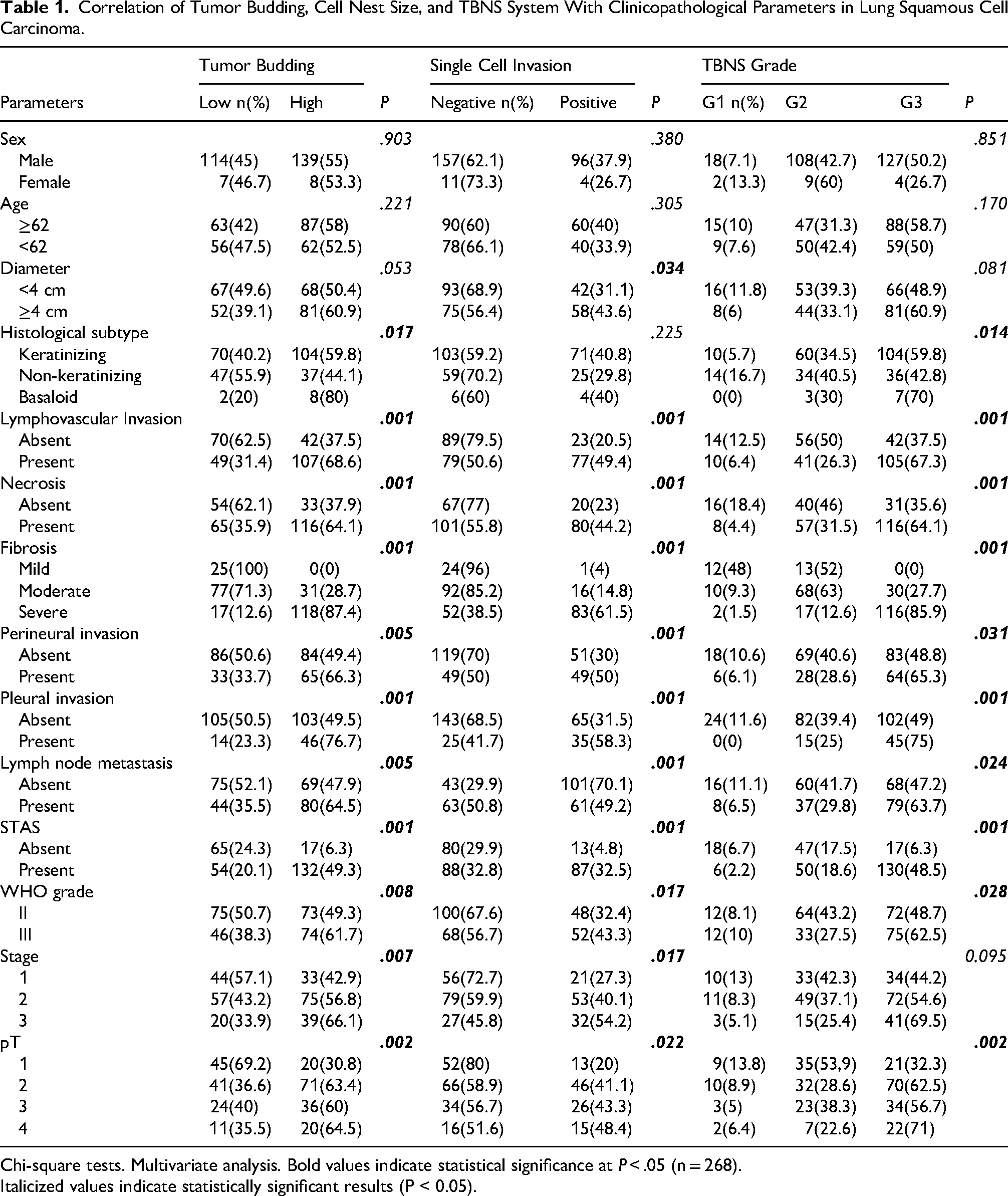
Chi-square tests. Multivariate analysis. Bold values indicate statistical significance at P < .05 (n = 268).
Italicized values indicate statistically significant results (P < 0.05).
Tumor Budding and TBNS
High tumor budding was detected in 107 (39.9%) patients with lymphovascular invasion, 116 patients with necrosis, 117 patients with severe fibrosis, 46 patients with pleural invasion, and 80 patients with lymph node metastasis. Single cell invasion was detected in 77 patients with lymphovascular invasion, 80 patients with necrosis, 83 patients with severe fibrosis, 35 patients with pleural invasion, and 61 patients with lymph node metastasis. Of the 149 patients with high tumor budding, 104 were single cell invasion. According to the TBNS system, as the score increased (G3), lymphovascular invasion (105, 67.3%), severe fibrosis (116, 85.9%), pleural invasion (45, 75%), and STAS (130, 48.5%) were observed at higher rates.
In the high-tumor-budding group, 104 patients (59.8%) were classified as keratinizing SCC, while 37 patients (44.1%) were identified as non-keratinizing SCC. According to the TBNS grading system, 104 patients (59.8%) within the G3 poorly differentiated category also corresponded to the keratinizing SCC subtype.
STAS
STAS were identified in 186 (69.4%) patients, among which high-grade tumor budding was observed in 132 (49.3%) patients. Single-cell invasion was detected in 87 (32.5%) patients. According to the TBNS system, STAS-positive 130 (48.5%) patients were classified as grade 3 (G3), while 50 (18.6%) were classified as grade 2 (G2). In 102 (54.8%) of the STAS-positive patients, the tumor diameter exceeded 4 cm. A total of 122 (65.6%) patients were histologically diagnosed as keratinizing type SCC. Pleural invasion was noted in 47 (25.3%) patients, and lymph node metastasis was present in 84 (45.2%) patients. The follow-up period for the 105 (56.4%) STAS-positive patients was less than 41 months. In addition, STAS-positive tumors were more frequently associated with advanced pathologic stages (P = .001).
Survival and Clinicopathological Analysis
When tumor budding and clinicopathological features were analyzed, the presence of high-grade tumor budding was significantly associated with poor overall survival (P = .005) (Figures 2 and 3), single-cell invasion (P = .001), presence of STAS (P = .001), high TBNS grade (P = .001), and pleural invasion (P = .001). Similarly, when disease-free survival was evaluated, high-grade tumor budding correlated with shorter disease-free survival (P = .001), single-cell invasion (P = .001), presence of STAS (P = .005), high TBNS grade (P = .001) (Figures 2 and 3), pleural invasion (P = .001), advanced pathological tumor stage (pT stage) (P = .001), and lymph node metastasis (P = .002). No significant association was found between other clinicopathological parameters and either overall survival or disease-free survival (Table 2).
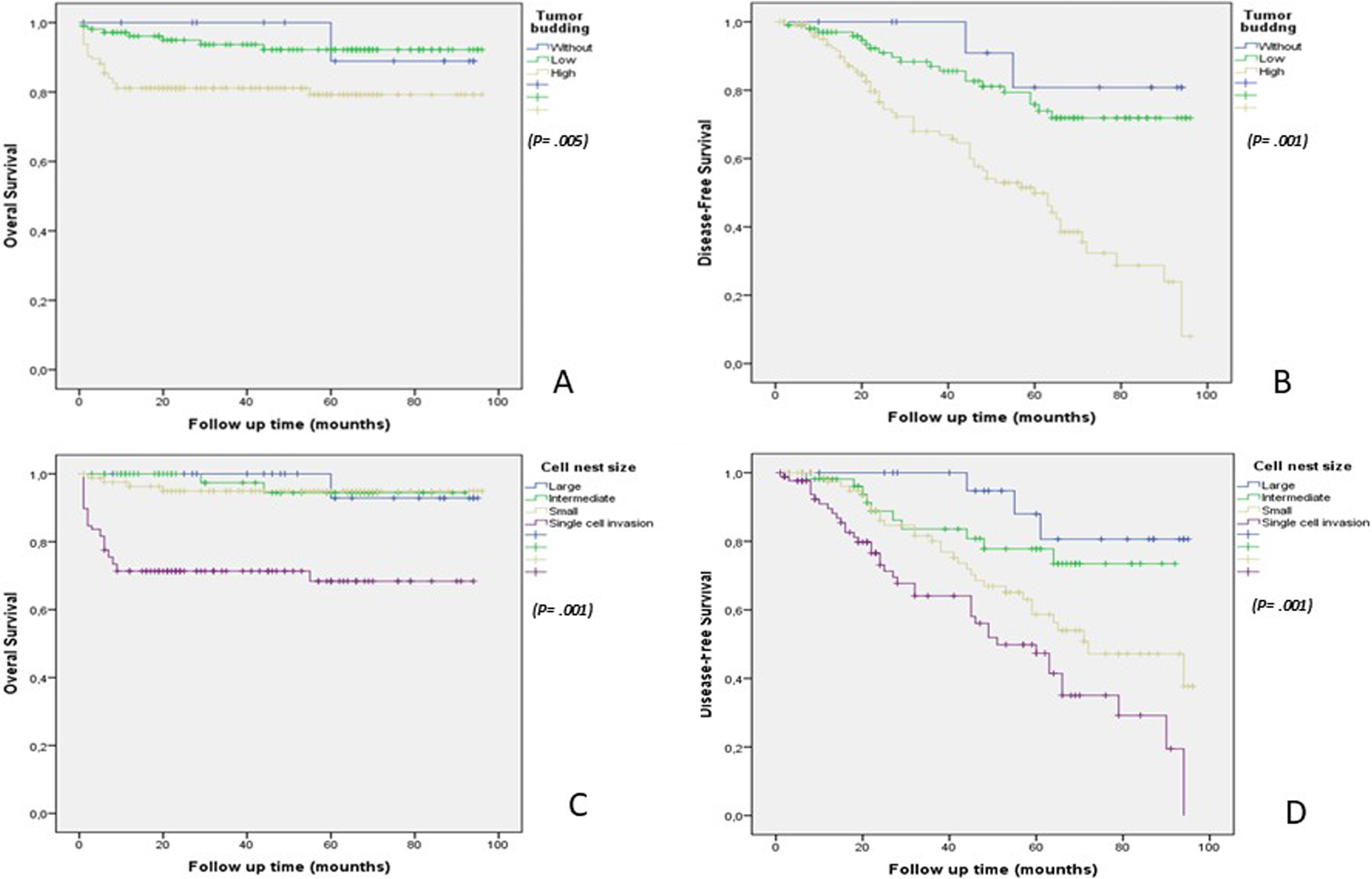
Association of the Lung SCC Tumor Budding and Cell Nest Size With Overall Survival (A, C) and Disease-Free Survival (B, D) in the Test Cohort.
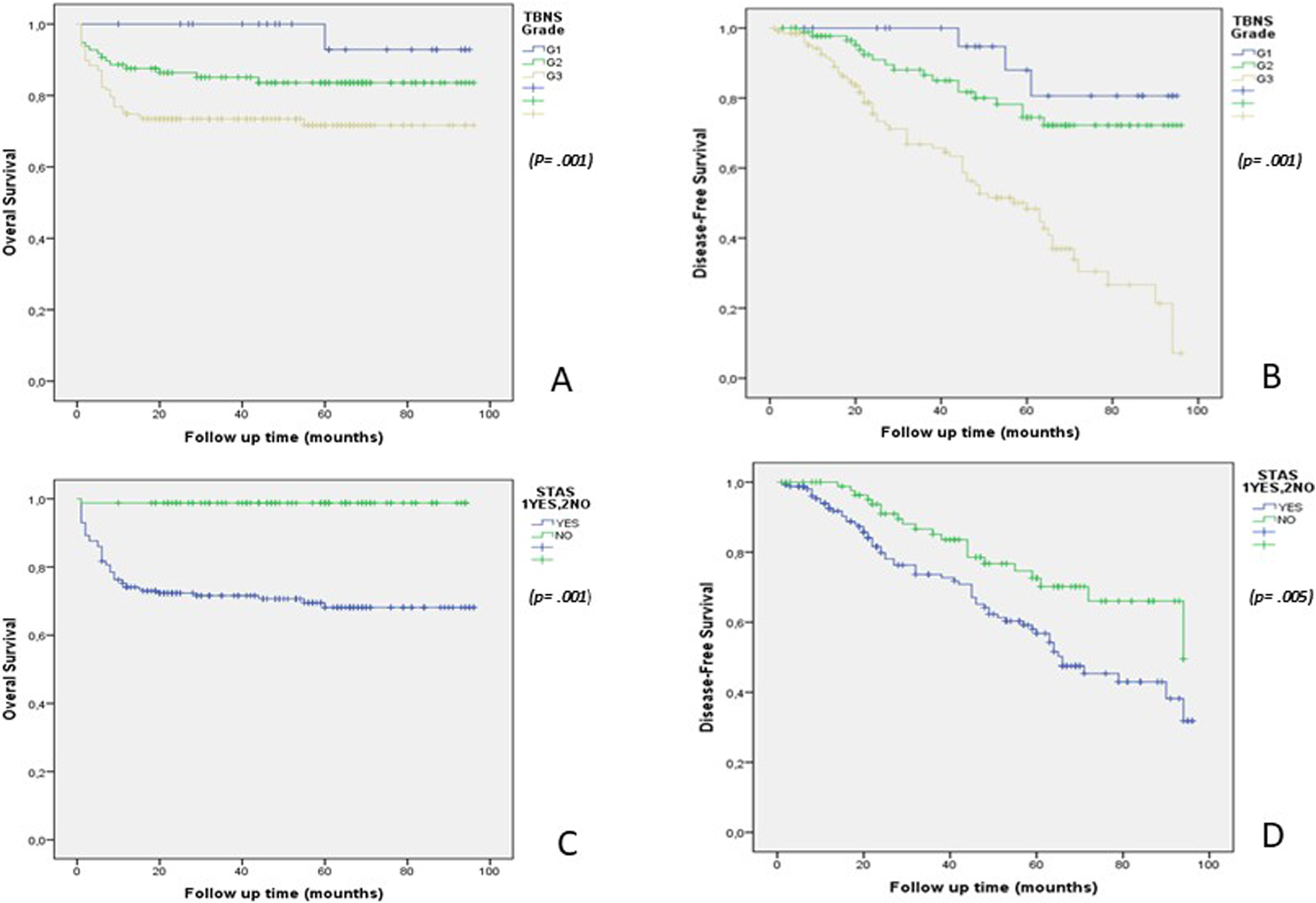
Association of Tumor Budding and Cell Nest Size (TBNS) Grading System and Spread Through Airspaces (STAS) in Lung SCC With Overall Survival (A, C) and Disease-Free Survival (B, D) in the Test Cohort.
Multivariate Analysis for Overall Survival and Disease-free Survival in Lung Squamous Cell Carcinoma.
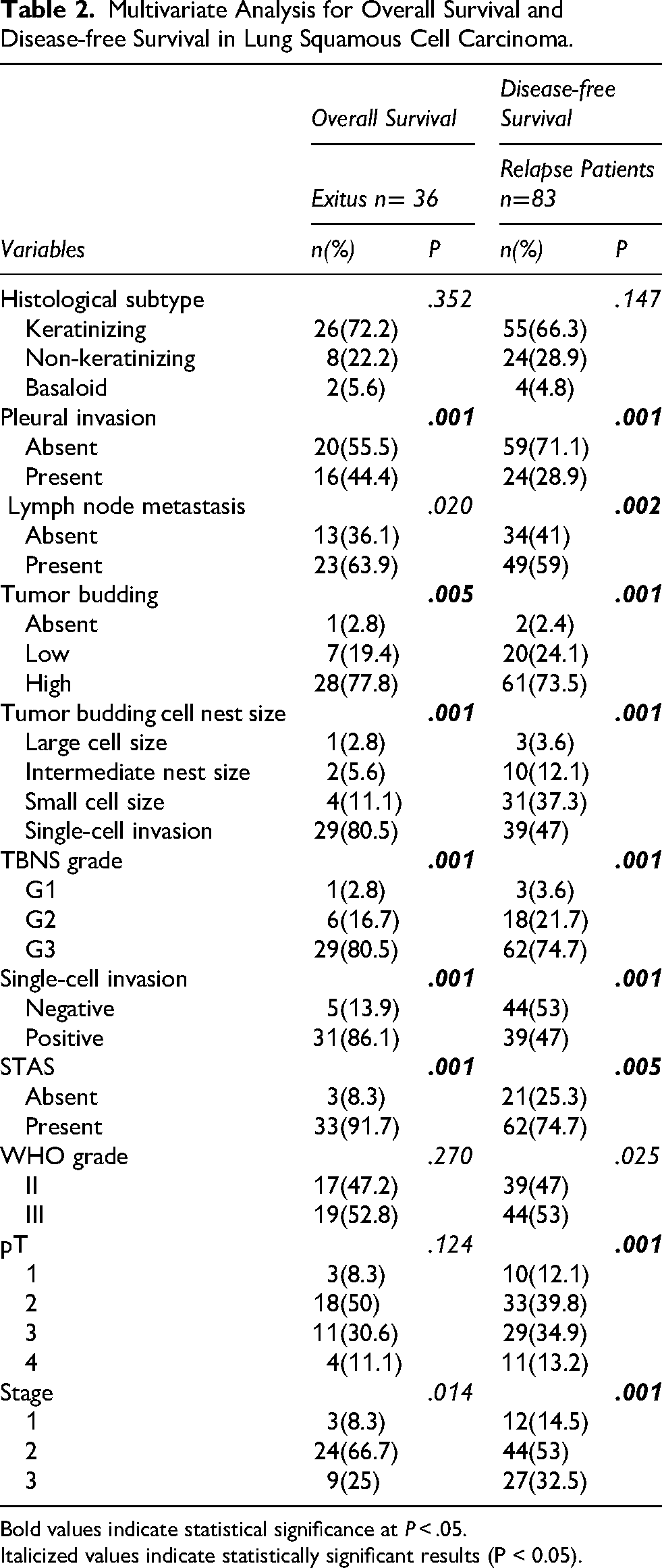
Bold values indicate statistical significance at P < .05.
Italicized values indicate statistically significant results (P < 0.05).
Discussion
Lung cancer is the most common cancer group worldwide and is also the leading cause of cancer death (18.7% of total cancer deaths). 1 The most important reason for this is that the majority of patients are in advanced stages at the time of diagnosis (70%). 2 The majority of lung cancer types are NSCLC. 2 The most common tumor types within NSCLC are adenocarcinoma and SCC. 2 A grading system was established for adenocarcinomas in 2011 by the IASLC, American Thoracic Society (ATS), and European Respiratory Society (ERS) groups, which groups them according to the predominant histological pattern. 24
It is not completely clear whether similar histological parameters have prognostic significance in lung SCC. Therefore, in recent years, various histological features have been investigated to better predict the prognosis of lung SCC. Among these parameters, high tumor budding, single cell invasion, and presence of STAS have attracted attention as an indicator of aggressive behavior and poor prognosis in lung SCC.25,26 Studies by Taira et al 27 and Masuda et al 28 have demonstrated that high-grade tumor budding is significantly associated with adverse prognostic features such as lymph node metastasis, pleural invasion, and advanced tumor stage. Similarly, Gürel et al 29 reported that tumor budding correlated with shorter disease-free and overall survival in SCC patients. In our study, consistent with the literature, high-grade tumor budding was significantly associated with single-cell invasion, higher TBNS grade, presence of STAS, pleural invasion, and poor survival outcomes.
STAS has also been evaluated as a poor prognostic indicator in lung tumors.29,30 Kutlay et al 31 and Lu S et al 32 showed that STAS presence in pulmonary SCC was significantly correlated with lymph node metastasis and poor survival. Our findings align with these results, showing that STAS-positive tumors tended to have larger diameters, higher tumor budding, pleural invasion, lymph node metastasis, and shorter survival.
The presence of STAS was significantly associated with adverse pathological features, including larger tumor size (P = .005), higher tumor budding (P = .001), pleural invasion (P = .001), and lymph node metastasis (P = .001) (P < .05 for all comparisons). Patients with STAS-positive tumors demonstrated a shorter follow-up duration, suggesting a poorer overall survival compared to STAS-negative patients (P = .001). Furthermore, the frequent detection of STAS in patients with advanced pathological stage supports the hypothesis that STAS may contribute to more aggressive tumor behavior and could serve as a prognostic indicator in lung SCC. These findings emphasize the importance of evaluating both STAS and tumor budding in routine pathological assessment to better stratify patients’ prognoses and guide postoperative management strategies.
Kadota et al 16 emphasized that tumor budding is associated with stromal activation, suggesting a more invasive phenotype in lung SCC. Additionally, studies by Uruga et al 33 and Eguchi et al 34 in lung adenocarcinomas highlighted the prognostic impact of STAS, suggesting that its evaluation could influence surgical decisions and postoperative management.
Taken together, these findings emphasize the importance of integrating both tumor budding and STAS evaluation into routine histopathological assessment to stratify patients more accurately according to their prognosis and to tailor more effective postoperative management strategies.
Conclusion
In conclusion, our study demonstrates that both high-grade tumor budding, single cell invasion and the presence of STAS are independently associated with adverse clinicopathological features and poor survival outcomes in lung SCC. These histopathological parameters can serve as valuable prognostic indicators, and their routine evaluation should be encouraged to optimize treatment planning and follow-up strategies.
Footnotes
Ethical Approval
This study was approved by the Clinical Research Ethics Committee of the Istanbul Yedikule Chest Disease and Thoracic Surgery Training and Research Hospital (2021-94).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.