
Abstract
Extrauterine presentation of Mullerian adenosarcoma is rare and thought to either arise from endometriosis or from spread from a primary uterine or ovarian origin. When accompanied by sarcomatous overgrowth, particularly when the epithelial components are limited or obscured, these tumors can be challenging to recognize as adenosarcomas and may be misdiagnosed as primary pelvic or retroperitoneal sarcomas. Diagnostic molecular testing could be valuable but also misleading, if not interpreted in the right context, as some retroperitoneal sarcomas exhibit alterations that can have overlapping molecular alterations with Mullerian adenosarcoma, such as MDM2 amplification in liposarcomas. In this report, we describe three Mullerian adenosarcomas with extrauterine presentation, all exhibiting extensive sarcomatous overgrowth and MDM2 amplification. These tumors underscore the critical importance of integrating clinical history, comprehensive tissue sampling, detailed morphologic evaluation, and molecular analysis to establish an accurate diagnosis.
Introduction
Mullerian adenosarcoma is a rare and heterogeneous biphasic neoplasm composed of benign epithelial and malignant stromal components. While adenosarcoma most commonly arises in the uterine corpus, it can also occur in the cervix, vagina, and, rarely, in extrauterine intrabdominal sites such as the ovary or peritoneum. Following exclusion of spread from a primary uterine origin, a primary extrauterine Mullerian adenosarcoma is presumed to arise from endometriosis. The behavior is more aggressive than its primary uterine counterpart.1-3 The diagnosis of adenosarcoma is typically straightforward if the classic features of the phyllodes-like pattern or periglandular stromal cuffing pattern are present. However, rare tumors may exhibit sarcomatous overgrowth and high-grade atypia that obscures the classic architectural patterns of adenosarcoma, resulting in a tumor exhibiting high-grade sarcomatous features and a broad differential diagnosis. In tumors presenting in extrauterine, intra-abdominal sites, the clinical setting may lead to consideration of a primary pelvic or retroperitoneal sarcoma, which may guide the immunohistochemical and diagnostic molecular testing strategy, without any consideration of Mullerian adenosarcoma. This may lead to further diagnostic misinterpretations as there are a few molecular alterations that overlap between Mullerian adenosarcoma and extra-Mullerian sarcomas such as liposarcomas which characteristically show MDM2 amplification.
The molecular profile of adenosarcomas is heterogeneous and may show mutations of genes within the PI3K/AKT/PTEN pathway, DICER1, ATRX, FGFR2, KMT2C and TP53, as well as amplifications of the chromosomal region 12q13-15 including the MDM2 and CDK4.4-7 Conversely, there is no specific molecular hallmark of Mullerian adenosarcoma. Based on reports of MDM2 amplification in some Mullerian adenosarcoma, we hypothesized that this may theoretically pose a diagnostic dilemma in the distinction of MDM2-amplified liposarcoma from extrauterine presentation of Mullerian adenosarcoma. Therefore, we searched our departmental archive for MDM2-amplified Mullerian adenosarcomas with extrauterine presentations. Herein, we present the clinicopathological and molecular features of three extrauterine Mullerian adenosarcoma with sarcomatous overgrowth and MDM2 amplification, highlighting the diagnostic complexities and molecular features that distinguish these unusual presentations. These tumors underscore the need for a comprehensive approach to diagnosis and management, particularly when confronted with atypical presentations and overlapping molecular profiles that may mimic other sarcomas.
Methods
The specimens were identified by a search of our departmental archive for all uterine mesenchymal tumors, and all Mullerian adenosarcomas that had undergone molecular diagnostic testing showing MDM2 amplification. Clinical information was obtained from electronic medical records (Summarized in Table 1). Hematoxylin and eosin (H&E) and immunohistochemical slides were reviewed. Immunohistochemistry was performed on 4 µm-thick sections cut from formalin-fixed and paraffin-embedded tissue as previously described. 8 Capture-based DNA next-generation sequencing (NGS) was performed using a custom assay that targets a total footprint of ∼3.5 Mb that includes all coding exons of 529 cancer-related genes, select introns and upstream regulatory regions as previously described. 6
Clinicopathologic Features of Difficult to Diagnose MDM2-Amplified Mullerian Adenosarcomas.
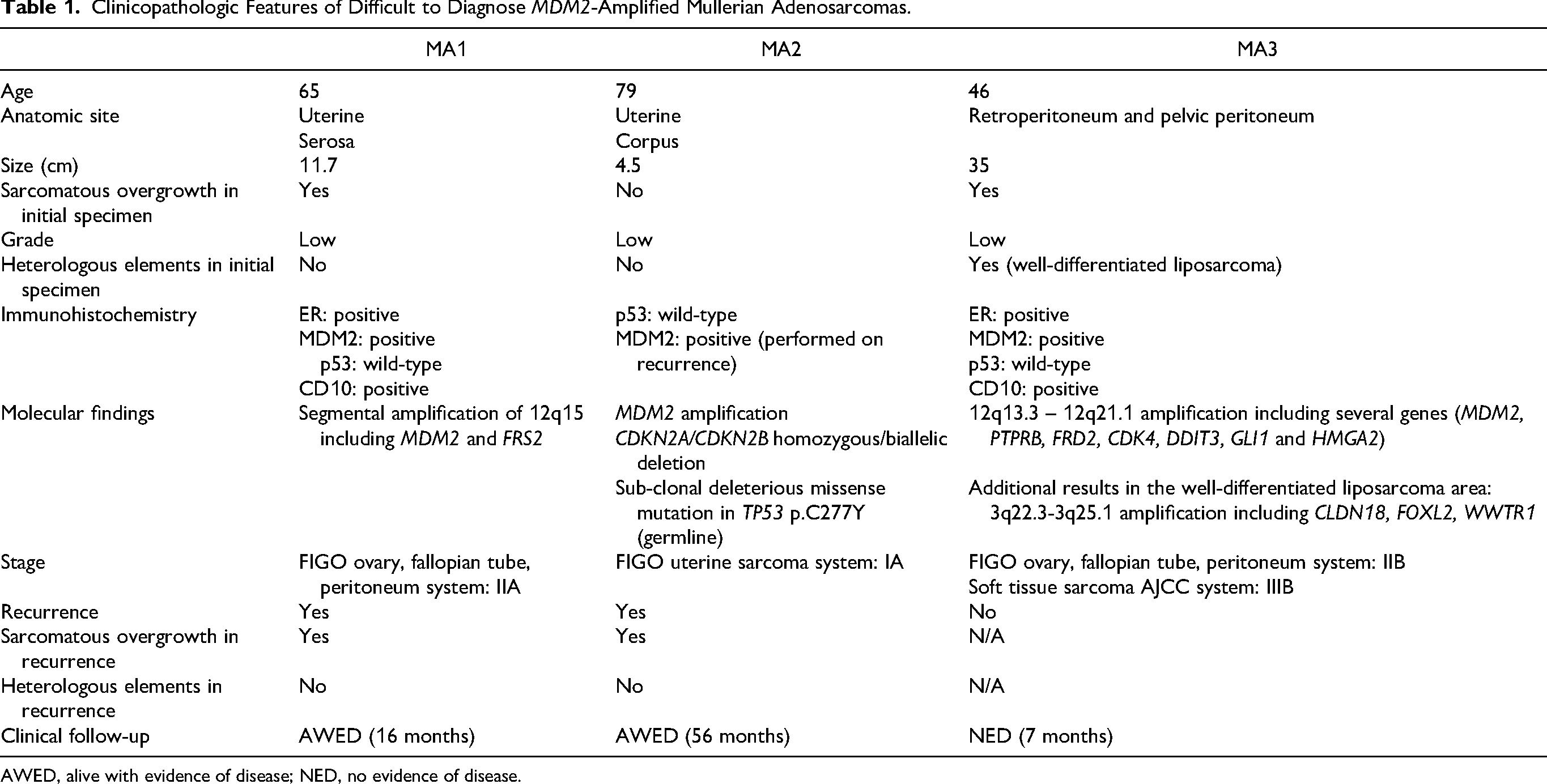
AWED, alive with evidence of disease; NED, no evidence of disease.
Case Report
Patient 1
The patient was a 65-year-old woman with an 11.7 cm posterior uterine mass who underwent resection of the mass and total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO). The mass (11.7 cm) was attached to the posterior uterine serosa and sigmoid mesentery and resected in multiple fragments (Figure 1A). The macroscopic appearance of the tumor was tan, rubbery, and solid without hemorrhage or necrosis. The endometrium, myometrium, cervix, ovaries and fallopian tubes were macroscopically normal appearing (Figure 1B).

The tumor was extensively submitted for microscopic evaluation and showed solid sheets of mild to moderately atypical plump and spindled cells with increased mitotic activity (Figure 1C). Although classic architectural features of adenosarcoma were not present, there was a small focus of benign, cystically dilated glands with irregular contours that were surrounded by hypercellular zone of atypical spindle cells. The glandular epithelium did not exhibit any other architectural abnormality or cytological atypia (Figure 1D). The left ovary contained endometriosis. The endometrium, myometrium and uterine serosa were normal.
Immunohistochemical staining showed that the spindle cells were positive for CD10 and estrogen receptor but were negative for desmin, smooth muscle actin, smooth muscle myosin, caldesmon, ALK, STAT6, DOG1 (ANO1), KIT, HMB45 and cathepsin K. The p53 stain showed a wild-type result.
As the combination of morphological and immunohistochemical features was not specific for tumor classification, NGS was performed. A segmental amplification of chromosomal region 12q15 that includes MDM2 and FRS2 was identified. MDM2 immunohistochemistry was performed which showed diffuse nuclear positivity in the spindle cell component (Figure 1E).
Overall, the tumor was classified as a FIGO stage IIA primary peritoneal adenosarcoma. The patient was planned to receive radiation therapy; however, 5 months after the initial procedure, she presented with a large heterogeneously enhancing mass (10.6 cm) in the right lower pelvis as well as multiple peritoneal nodules concerning for recurrent malignancy, and she underwent tumor debulking instead. The microscopic appearance of the mass was a spindle cell proliferation similar to the prior tumor; however, a glandular component was not identified. MDM2 immunostaining was diffusely positive.
The patient was subsequently treated with pelvic radiation and chemotherapy. Fourteen months after the initial diagnosis, the patient is alive with disease (Table 1).
Patient 2
The patient was a 79-year-old with a 4.5 cm uterine mass who underwent TAH-BSO. The macroscopic appearance was a tan-brown, fleshy mass without hemorrhage or necrosis, confined to the endometrium (Figure 2A).

Microscopically, the tumor exhibited classic features of Mullerian adenosarcoma, specifically both the phyllodes-like pattern and the periglandular stromal cuffing pattern (Figure 2B). Increased stromal cellularity was focally present but was not extensive to qualify as stromal overgrowth. There was no heterologous differentiation.
Immunohistochemical staining for p53 showed a wild-type result. NGS was performed to further assess the focal areas of increased stromal cellularity. The result showed focal deep deletion of 9p21.3 including CDKN2A/CDKN2B, focal deep deletion of RB1 and 12q15 amplification including MDM2. Overall, the tumor was classified as a FIGO stage IA primary uterine adenosarcoma. The patient underwent surveillance.
Three years later, the patient presented with a 13 cm retroperitoneal mass which was resected. The macroscopic appearance was fleshy and solid with areas of necrosis, hemorrhage and gelatinous change (Figure 2C).
Microscopically the tumor was a solid proliferation of pleomorphic spindle cells with increased mitotic activity (5/10 HPF). There was no glandular component (Figure 2D). MDM2 IHC was diffusely positive. NGS showed homozygous/biallelic deletion in CDKN2A/CDKN2B along with a low-level amplification of MDM2, similar to features observed in the primary tumor. The patient was managed by chemotherapy.
Five months after the second procedure, an MRI of the pelvis and abdomen showed recurrent disease which included a 3.5 cm mass at the resection site. The patient received chemotherapy and immunotherapy. She continued to progress and was placed in hospice care 20 months after the second procedure. The patient is alive with disease.
Patient 3
The patient was a 46-year-old with a 35 cm retroperitoneal mass concerning for liposarcoma on imaging who underwent resection of the mass along with TAH-SO. The macroscopic appearance of the tumor was predominantly fatty with scattered areas of tan-white, firm, nodular, whorled tissue (Figure 3A). Microscopically, the tumor exhibited 3 spatially demarcated components. The dominant pattern (∼80%-90% of the tumor) was a solid proliferation of mature adipocytes with occasional enlarged, hyperchromatic spindled cells (Figure 3B). The second component (∼10%-20% of the tumor) consisted of scattered nodules of bland smooth muscle (Figure 3C). The third component (∼1% of the tumor) consisted of small foci of the phyllodes-like pattern and periglandular stromal cuffing pattern of Mullerian adenosarcoma (Figure 3D). The left ovary and the fallopian tube contained endometriosis. The endometrium and myometrium were normal.

Immunohistochemical staining for MDM2 showed diffuse nuclear expression in the spindled cells of all 3 of the microscopic components of the tumor (Figure 4).
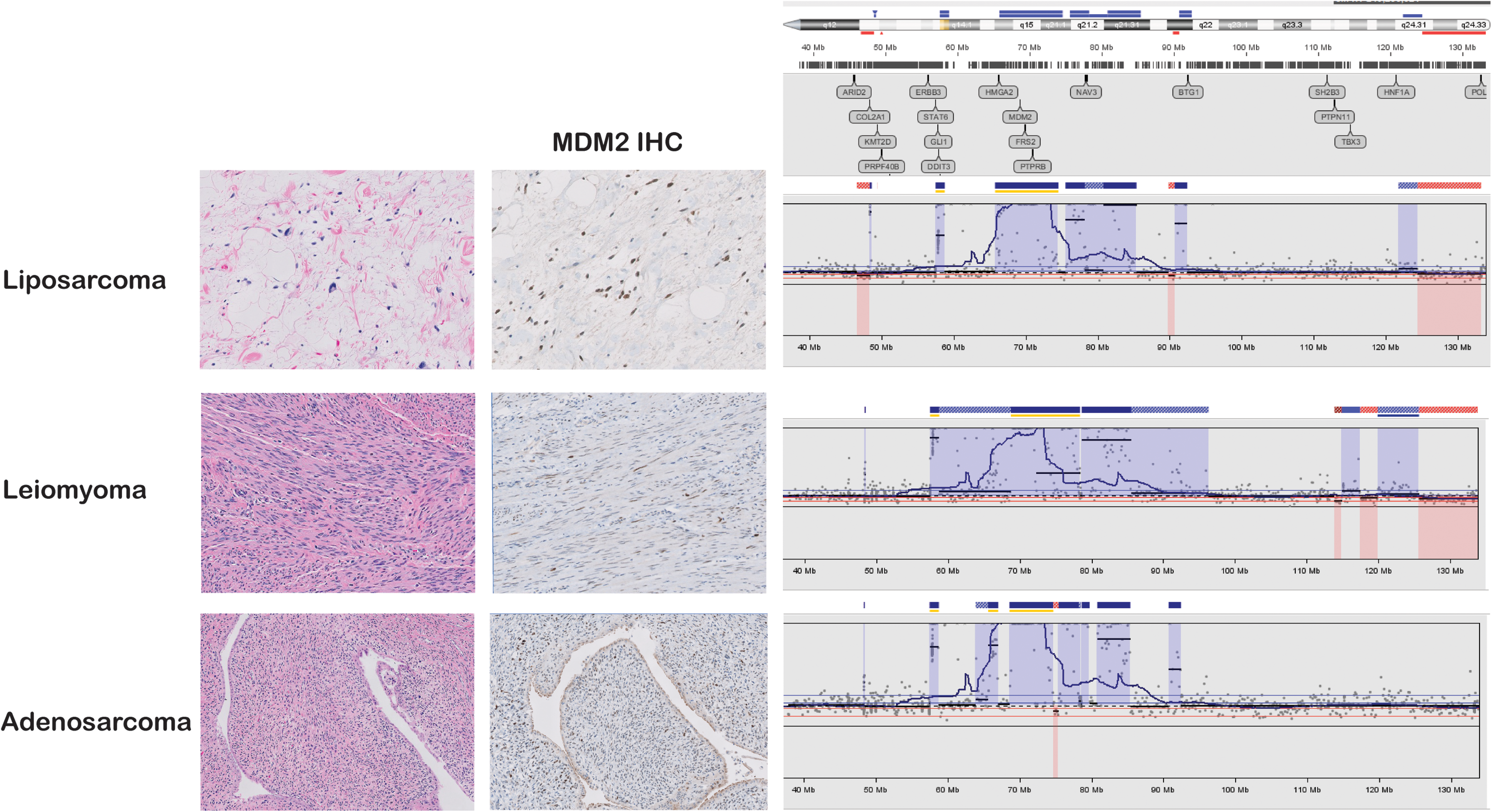
NGS was performed on each component, and the results were the same in all 3 components. There was amplification of 12q13.3 - 12q21.1 amplicon including MDM2, PTPRB, FRD2, CDK4, DDIT3, GLI1 and HMGA2 (Figure 4). The well-differentiated adipocytic component additionally showed 3q22.3-3q25.1 amplification including CLDN18, FOXL2, WWTR1.
Overall, the tumor was classified as a stage IIB primary peritoneal Mullerian adenosarcoma with heterologous differentiation of both liposarcomatous and leiomyomatous differentiation. The patient received adjuvant aromatase inhibitor therapy with letrozole. She has been alive without disease for 7 months.
Discussion
The tumors described here expand the spectrum of Mullerian adenosarcoma that may harbor MDM2 amplification. The practical significance of this finding is the potential diagnostic pitfall with other spindle cell neoplasms that harbor MDM2 amplification, particularly for tumors with extrauterine involvement, sarcomatous overgrowth and absence of classical growth patterns of adenosarcoma.
MDM2 amplification has been reported in various tumors, such as well-differentiated and de-differentiated liposarcomas, parosteal osteosarcoma, glioblastoma and some carcinomas.9-11 In the gynecologic tract, MDM2 amplification is most commonly seen in Mullerian adenosarcomas and does not necessarily indicate a poor prognostic factor. 12 In our institution's cohort of 70 molecularly sequenced uterine mesenchymal neoplasms, including smooth muscle tumors, endometrial stromal sarcomas, PEComas and Mullerian adenosarcomas, 5 showed MDM2 amplification, and all were Mullerian adenosarcomas. None of the leiomyosarcoma, PEComa, endometrial stromal sarcoma and undifferentiated sarcomas had MDM2 amplification, although MDM2 amplification is rarely reported in endometrial stromal tumors and undifferentiated sarcomas therefore other gynecologic tract mesenchymal neoplasms should still be considered in the differential diagnosis. 13
The leading diagnosis in an otherwise undifferentiated peritoneal/retroperitoneal spindle cell tumor with MDM2 amplification will often be a de-differentiated liposarcoma.14-16 For the first patient, a dedifferentiated liposarcoma is not favored for several reasons: 1) the presence of entrapped benign glands in the initial specimen would be highly unusual, 2) a well-differentiated liposarcoma component was not identified in either the initial or recurrent tumor, and 3) the degree of MDM2 copy number gain is lower than usually seen in dedifferentiated liposarcoma.17,18 For the second patient, the extrauterine recurrence was completely devoid of a glandular component. However, the recurrence showed an essentially identical molecular profile to the primary uterine tumor. Without adequate clinical history, access to the pathology and molecular features of the primary tumor, dedifferentiated liposarcoma would have been difficult to exclude in the recurrence. The tumor from Patient 3 is by far the most challenging since it demonstrates lipogenic, myogenic and undifferentiated spindle cell components. The presence of benign glandular areas, albeit rare (2 of 80 H&E sections), combined with an essentially identical 12q13-21 amplicon in all three components of the tumor (Figure 4), supported adenosarcoma with heterologous differentiation. Heterologous differentiation in adenosarcomas is not an uncommon phenomenon, and rhabdomyosarcomatous, leiomyosarcomatous or osteosarcomatous elements have been reported previously.19,20 While mature adipose tissue within Mullerian adenofibromas or adenosarcomas has been rarely described, well-differentiated liposarcomatous component has not been reported to occur as a type of sarcomatous overgrowth. 21 Apart from the liposarcomatous areas, patient 3's tumor also contained a benign smooth muscle differentiation, which was rarely reported before. 22
Extrauterine and extra-ovarian Mullerian adenosarcomas are extremely rare, with only about 45 reported to date, most arising in the pelvic peritoneum and vagina. 2 Given the rarity of Müllerian adenosarcomas overall, most molecular studies have focused on uterine tumors. Consequently, the molecular characteristics of extrauterine Mullerian adenosarcomas remain largely undefined, though they are presumed to resemble those of uterine counterparts, which frequently exhibit alterations in the PI3K/AKT/PTEN pathway and TP53 in high-grade tumors. 12 The tumors presented here did not show any mutation in these genes. Even though MDM2 amplification alone is unusual in Mullerian adenosarcomas, it has been reported. 6 However, the absence of other mutations typically associated with Mullerian adenosarcomas made the diagnosis of the tumors described here more challenging.
In summary, extrauterine adenosarcomas with extensive sarcomatous overgrowth are diagnostically challenging and may be impossible to differentiate from other retroperitoneal sarcomas if limited tissue is available. Reliance on MDM2 or 12q13-15 amplification to diagnose dedifferentiated liposarcoma in a retroperitoneal tumor in a female patient is a potential pitfall. An incorrect diagnosis may be exacerbated by inadequate clinical history, small biopsy or inadequately sampled tumor.
Footnotes
Ethics Approval
The study was approved by our institutional review board.
Consent for Publication
All authors can attest that the submitted report includes only nonidentifiable CT images, pathology images and sequencing results. The scope of this report was generated through the Institutional Review Board which does not require consent to collect this data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
This study is not part of a clinical trial.