
Abstract
With the 2022 WHO Classification of Neuroendocrine Neoplasms 1 came an important distinction between epithelial and non-epithelial neoplasms, and the possibility of composite tumor in certain organs, including the duodenum, the spine and the middle ear. In particular, the formerly termed gangliocytic paraganglioma of the duodenum has been renamed as “composite gangliocytoma/neuroma and neuroendocrine tumor (CoGNET).” We present an unusual CoGNET arising in the stomach, displaying distinctive histomorphologies in primary tumor and metastases. Additionally, we discuss diagnostic pitfalls and highlight the importance of recognizing the combined features that can be seen in this rare, potentially malignant, entity.
Keywords
Patient Presentation
A 57-year-old male patient presented with acute low back pain. Computed tomography (CT) imaging of chest, abdomen and pelvis revealed a 7.3-cm peripherally enhancing and centrally necrotic mass surrounding the stomach and the gastrohepatic ligament with an adjacent satellite nodule. An fluorodeoxyglucose-positron emission tomography (FDG PET)/CT similarly showed an intensely hypermetabolic centrally necrotic mass centered at the lesser curvature of the stomach, along with the satellite nodule. A DOTATATE PET/CT demonstrated high somatostatin receptor expression in both FDG avid masses, measuring 7 and 2 cm (Figure 1).
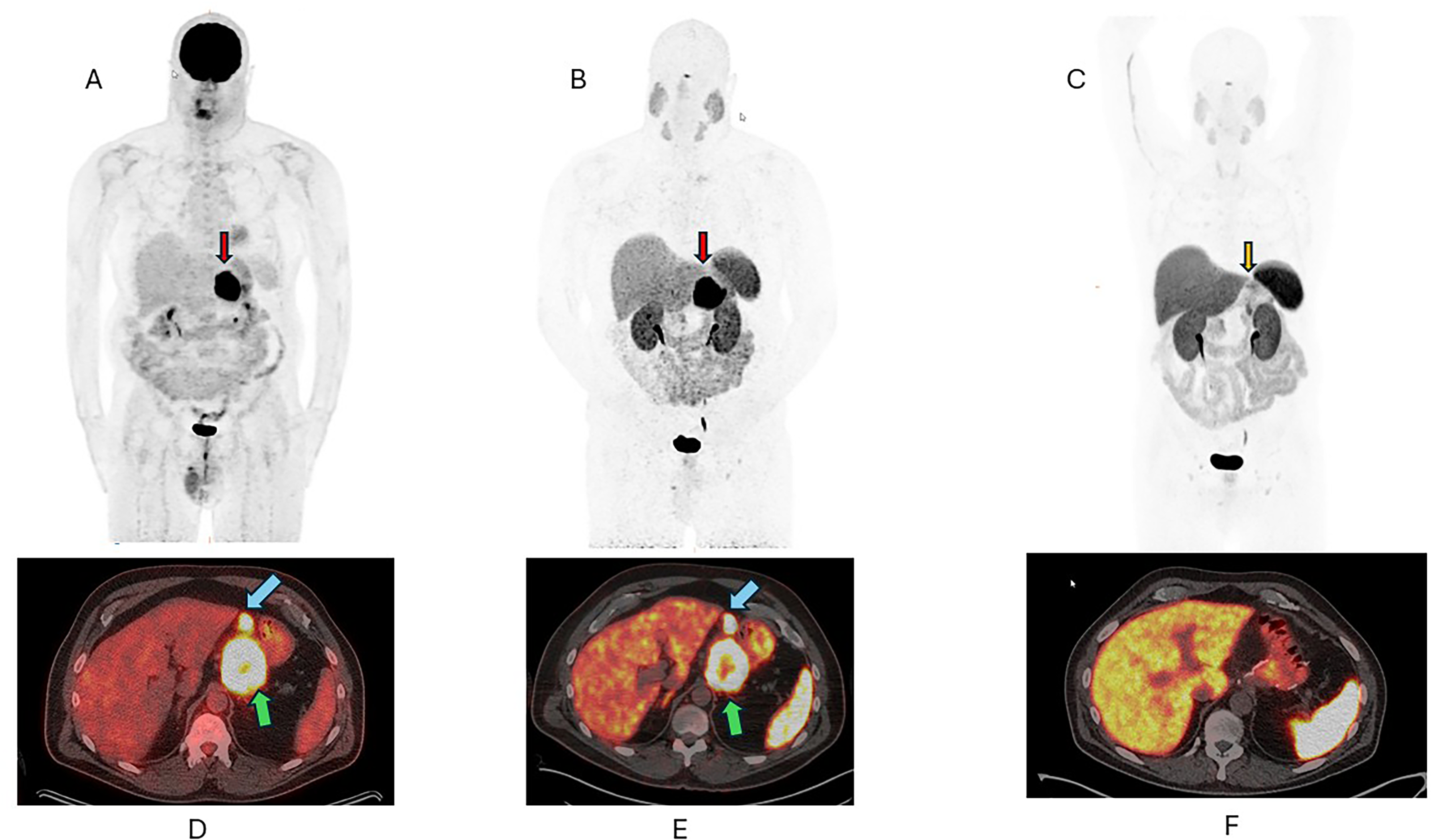
(A) Baseline FDG PET scan. (B) Baseline DOTATATE PET scan. (C) Post-operative DOTATATE PET scan. Lower panels (D, E, and F) are fused PET/CT images of (A), (B), and (C), respectively.
The patient underwent a diagnostic ultrasound guided biopsy of the gastrohepatic ligament mass, which revealed monomorphic population of ovoid tumor cells with moderate cytoplasm and finely granular nuclear chromatin, that stained diffusely for synaptophysin and chromogranin, with a Ki-67 (MKI67) index of 18%. The tumor was thus diagnosed as a well-differentiated neuroendocrine tumor (NET), Grade 2.
After multidisciplinary consultation, treatment with octreotide was initiated, followed by total gastrectomy and omentectomy two months later. Gross examination revealed three separate masses, a primary, 2.6 cm tumor arising in the lesser curvature of the gastric wall and the lesser omentum demonstrating two separate, distinctive masses, a 9-cm mass and a second, 2.5-cm grossly positive lymph node.
Representative sections of all three masses were studied histologically. Sections of the primary gastric mass showed a triphasic neoplasm composed of morphologically distinct components: (1) a spindle cell component, intermixed with (2) clusters/nests of plump epithelial cells, and (3) scattered ganglion cells (Figure 2), that involved the mucosa and submucosa of the stomach. The larger omental mass demonstrated predominantly epithelial cells resembling the biopsy (consistent with a well-differentiated NET), with focal areas showing spindle-shaped and ganglion cells. The omental lymph node also showed similar triphasic morphology. The approximate proportions of three components in the primary tumor and smaller omental lymph node were epithelial (50%), spindle cell (40%) and ganglion cells (10%); while the larger omental mass showed predominantly epithelial cells, as described above. Lymphovascular invasion was identified in the perigastric soft tissue near the omental mass. No discernible mitotic figures or evidence of necrosis were noted in the three masses.

Primary gastric mass. (A) Low power view (40×) showed primary gastric mass involving submucosa. (B) Scattered keratin immunostaining was observed in the epithelial component of the mass. (C, D) Higher power view (200×) showed the epithelial component with corresponding positive synaptophysin immunostaining. (E, F) Higher power view (200×) demonstrated the spindle cell and ganglion cell component with corresponding positive S100 immunostaining.
The epithelial cells showed variable positivity for keratin (AE1/AE3) and CAM5.2 (Figures 2 and 3) and were diffusely positive for chromogranin and synaptophysin (Figure 2). The spindle cell component was positive for S100 and SOX10, while the ganglion cells showed variable chromogranin and synaptophysin positivity. All components were negative for KIT (CD117), DOG1 (ANO1), and smooth muscle actin (SMA, ACTA2). A Ki-67 immunostain showed a low proliferation index in the main tumor (2.7%) and a higher index (18%) in the metastatic lymph node (Figure 3).

Metastatic lymph node. (A) Low power view (40×) showed residual lymphoid cells with extensive involvement by spindle cells. (B, C) Low and higher power views (40× and 200×) showed areas containing epithelial neuroendocrine cells. (D) Higher power view (200×) demonstrated vascular invasion near the omental nodule. (E) CAM5.2 immunostaining was positive in smaller metastatic lymph node. (F) The Ki-67 proliferative index was increased in smaller metastatic lymph node.
A duodenal primary CoGNET was excluded based on upper gastrointestinal endoscopy and cross-sectional imaging. Immediate postoperative imaging showed no residual or recurrent disease, and the patient was followed by observation. The patient developed multifocal liver and lymph node recurrences, identified on imaging studies, 18 months later.
Discussion
Composite gangliocytoma/neuroma and neuroendocrine tumors (CoGNETs) are well-known for their almost exclusive presence in the second part of the duodenum and periampullary region. Rare primaries have been reported in the jejunum, 2 pylorus, 3 esophagus, 4 pancreas,5,6 appendix, 7 cecum, 8 lung,9–11 nasopharynx, 12 and thymus. 13 The essence of CoGNETs and its ability to give rise to lymph nodal metastases, composed of all three components is exemplified though this particular specimen. Additionally, to the best of our knowledge, this is the first reported patient with a CoGNET arising in the stomach with metastasis.
CoGNETs are generally considered a neuroendocrine neoplasm of low malignant potential. Their reclassification from “gangliocytic paraganglioma” reflects the understanding that these are not true paragangliomas but composite tumors with epithelial and ganglioneuromatous components. 14 The origin of these tumors is still poorly understood, with some suggesting a hamartomatous proliferation of endodermal derived epithelial cells, with neuroectodermal ganglion and Schwann cells. 15
A recent systematic review 16 studied 162 papers of 263 patients of the then called “gangliocytic paragangliomas.” The mean age at diagnosis was 53.5 years (range: 15‒84 years). The male-to-female ratio was approximately 3:2. Not surprisingly, the most common site was the duodenum (89.7%) followed by the respiratory system, with a median tumor size of 25.7 mm. Clinical presentations included gastrointestinal bleeding, abdominal pain, anemia, nausea, weight loss, fatigue, jaundice, or incidental discovery. Lymph node metastases occurred in 11.4% of patients, and liver metastases in 1.1%. The most significant predictor of lymph node metastasis was tumor invasion beyond the submucosa or sphincter of Oddi (OR: 3.82; 95% CI: 1.42-10.30; p < .01).
Metastases have been reported in CoGNETs from the duodenum 17 as well as extraduodenal sites, namely the pancreas.18,19 Histologically, CoGNETs are triphasic neoplasms, composed of epithelial neuroendocrine cells, ganglion cells, and spindle-shaped cells, with variable proportions and distribution. The epithelial cells are the most easily recognizable, while the spindle cells and the ganglion cells can occasionally be challenging to find. 20 Each of the components exhibits a unique immunohistochemical profile, as was seen in the current specimen and reported in the literature. The epithelial cells stain positively for CD56, synaptophysin, neuron-specific enolase, progesterone receptor, pancreatic polypeptide, somatostatin, chromogranin, and cytokeratins. 21 In the spindle-shaped cells, S-100 protein has the highest rate of positive immunoreactivity. The ganglion cells have a more variable staining profile, that resembles the epithelial component, but have also been shown to stain positively for S-100. 16
Accurate recognition of CoGNETs is essential given their potential for metastasis, yet diagnosis can be challenging, particularly on small biopsies where one or more components may be underrepresented. Metastatic sites may also show a predominance of only one component, though some demonstrate all three. 20 In one study, the biopsy diagnosis rate prior to surgery was only 19%. 16 Among 63 patients, only 12 were correctly identified on biopsy, while others were misdiagnosed as NET, paraganglioma, or ganglioneuroma. Recent studies have suggested using progesterone marker and pancreatic polypeptide immunostains, which are both positive in CoGNETs, to help differentiate between NET and CoGNET. 16 This could be vital as conventional NETs may differ from CoGNETs in natural histories, prognostic stratification, and possibly genetics.
From a radiological standpoint, nuclear medicine is key as somatostatin receptors are overexpressed on majority of the well-differentiated NETs. DOTATATE coupled with positron emitters Ga-68 or Cu-64 allows detection of somatostatin receptors with high diagnostic accuracy. Combined with F-18 FDG PET, DOTATATE PET/CT allows in-vivo tumor characterization with respect to tumor proliferation rate as well as tumor heterogeneity.
There are no specific treatment recommendations for CoGNETs given the scarcity of data and it is not well known how the Ki-67 percentage affects survival outcomes or determines aggressiveness. 22 Therefore, in this patient, and in similar patients, options are modeled after standard treatment recommendations for neuroendocrine neoplasms and pheochromocytomas/paragangliomas. These include surgery, observation without adjuvant treatment for fully resected disease, somatostatin analogues and possibly peptide receptor radionuclide therapy (PRRT) for somatostatin receptor (SSTR) positive disease. Whether mechanistic target of rapamycin (MTOR), vascular endothelial growth factor (VEGF) targeting, immunotherapy, poly (ADP-ribose) polymerase (PARP) inhibition or standard chemotherapy can aid in treatment, remains unproven. Our patient was observed closely with regular follow-up visits. Upon disease recurrence, he initiated octreotide based on SSTR positivity on updated DOTATATE PET/CT and prior tolerance of the treatment.
Conclusion
We present a rare gastric CoGNET (>2.5 cm), involving the submucosa with large omental metastases. This specimen highlights that CoGNETs are not confined to the duodenum and can metastasize to regional lymph nodes and distant sites. Given their variable histologic spectrum, careful attention to the presence of all three cellular components and liberal use of immunohistochemistry are critical to avoid misclassification, especially on limited biopsies. Close observation and long-term follow-up are recommended as management strategies continue to evolve.
Footnotes
Ethical Approval
The study was approved by the Washington University in St. Louis Institutional Review Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.