
Abstract
Background:
Mesonephric adenocarcinoma (MA) is a non-HPV associated tumor originating from mesonephric remnants, predominantly occurring in the uterine cervix. Mesonephric-like adenocarcinoma (MLA) is a recently recognized rare malignancy of the female genital tract. Its histomorphology, immunohistochemistry, and molecular characteristics are similar to those of MA. However, unlike MA, MLA is not associated with mesonephric remnants.
Summary:
Histologically, MLA can present various patterns including tubule-like, glandular, papillary, solid, sex cord-like, trabecular, retiform, cribriform, glomeruloid, and spindle cell patterns. Immunohistochemically, most MLAs show negative or focal weak positive expression for ER, while being positive for TTF-1, CD10, and GATA3. Molecularly, these tumors often harbor KRAS gene mutations. This article summarizes the research progress on MLA, aiming to enhance the understanding of this tumor type among clinicians and pathologists.
Definition, Clinical Characteristics, and Pathogenesis of MLA
Mesonephric-like adenocarcinoma (MLA) is a recently defined special type of adenocarcinoma occurring in the ovary and endometrium. Most patients are postmenopausal women, and the most common clinical presentation is abnormal vaginal bleeding. MLA progresses rapidly, is prone to metastasis, and patients have a poor prognosis.1–3 MLA shares “overlapping” features with mesonephric adenocarcinoma (MA) of the cervix in terms of histomorphology, tumor cell immunohistochemical phenotype, and molecular genetics. However, MA is primarily associated with mesonephric remnants and/or hyperplasia, while MLA is mainly associated with Müllerian lesions such as endometriosis.4–6 According to the 2020 WHO Classification of Female Genital Tumors, MLA is categorized under “Other Endometrial Carcinomas (EC)” with an ICD-O code of 9111/3. 7
Epidemiologically, MLA is a rare tumor, accounting for 1% of all endometrial carcinomas. 7 Approximately 100 patients of uterine MLA and fewer than 50 patients of ovarian MLA have been reported in the current literature. Some MLAs are associated with related Müllerian-derived lesions.1–6 The clinical presentation of MLA is not significantly different from other types of endometrial carcinomas and/or ovarian cancer. It is often asymptomatic in early stages, with late-stage symptoms including pain, abnormal uterine bleeding, postmenopausal irregular bleeding, and abdominal distension. 8
Regarding pathogenesis, during early embryonic development, the Wolffian (mesonephric) ducts and Müllerian ducts coexist. In male patients, Wolffian duct remnants form the epididymis and vas deferens, and testosterone drives the Müllerian ducts to form the epididymis, vas deferens, and seminal vesicles. The absence of testosterone in women leads to regression of the Wolffian ducts; however, small remnants or inclusions may persist, typically located deep within the lateral cervical stroma, and can also be found in the ovarian hilum, broad ligament, uterine corpus, and vaginal wall. In women, the absence of testosterone leads to regression of the Wolffian ducts. Due to the lack of anti-Müllerian hormone (AMH) in women, the Müllerian ducts are not inhibited and therefore develop into the fallopian tubes, uterus, cervix, and upper third of the vagina. 9 Unlike MA of Wolffian origin, MLA tumors lack embryonic mesonephric duct remnants. The current mainstream view holds that MLA originates from the Müllerian ducts. The coexistence of ovarian MLA with Müllerian-derived lesions, including endometriosis, serous borderline tumors, and low-grade serous carcinoma (SC), supports the notion that Müllerian lesions may be the origin of MLA.10,11 Furthermore, when MLA coexists with Müllerian-derived tumors, both share the same driver gene (KRAS/NRAS) mutations and genomic copy number variations, while also having distinct molecular alterations. Based on morphological and molecular genetic analyses, two main hypotheses exist: first, that MLA may directly originate from the Müllerian duct with transdifferentiation towards a Wolffian direction; second, that MLA and Müllerian-derived tumors are closely related in origin, possibly arising from the same early stem cell, undergoing malignant transformation driven by KRAS/NRAS mutations, and differentiating towards Müllerian and/or Wolffian directions under the influence of differential molecular changes.10,11
Histological and Immunohistochemical Characteristics of MLA
Histologically, MLA exhibits various growth patterns under the microscope, including tubule-like (Figure 1), cribriform (Figure 2), glandular (pseudoendometrioid), papillary (Figure 3), solid (Figure 4), sex cord-like, trabecular, retiform, glomeruloid, and spindle cell patterns.12–14 These patterns often coexist within the same specimens (Figure 5), with pseudoendometrioid, tubule-like, and papillary patterns being the most common. Intraluminal eosinophilic secretions are a typical feature of MLA, seen focally in over 90% of tumors.12–14 Tumor cells can be flat, cuboidal, or columnar, often with scant, eosinophilic cytoplasm. Rarely, tumor cells may have clear cytoplasm 12 (Figure 6). Tumor cells show mild to moderate atypia; in very few tumors, they exhibit high-grade atypia. Nuclei are oval, with vesicular or clear chromatin (Figure 7). Some tumors show nuclear grooves or overlapping, resembling the nuclear features of thyroid papillary carcinoma 12 (Figure 8). Hobnail-like tumor cells are rarely seen. 15 Intracellular mucin, squamous metaplasia, and mesonephric remnants are absent in MLA.12–15 Additionally, it is important to note that MLA can coexist with other tumors. In endometrial tumors, MLA is often mixed with atypical endometrial hyperplasia and/or endometrioid adenocarcinoma. In extrauterine (mainly ovarian) tumors, reported components mixed with MLA are more diverse, including endometrioid neoplasia (borderline and carcinoma), low-grade serous neoplasia (borderline and low-grade SC), high-grade SC, mucinous borderline tumor, clear cell carcinoma, neuroendocrine carcinoma, and germ cell tumors (teratoma, mixed germ cell tumor). Besides its association with mixed histology, extrauterine MLA is also strongly associated with endometriosis. Some scholars propose including MLA in the list of endometriosis-associated cancers.16–19

MLA tumor cells are arranged in a tubular pattern. Hematoxylin & eosin stain, 20X magnification.

MLA with cribriform growth pattern. Hematoxylin & eosin stain, 20X magnification.

MLA tumor cells form complex papillary structures. Hematoxylin & eosin stain, 20X magnification.

MLA tumor cells exhibit a solid arrangement, with necrosis visible. Hematoxylin & eosin stain, 20X magnification.

In MLA, different morphologies are seen mixed together: tumor cells on the left exhibit a glomeruloid pattern, while those on the right form solid structures. Hematoxylin & eosin stain, 20X magnification.
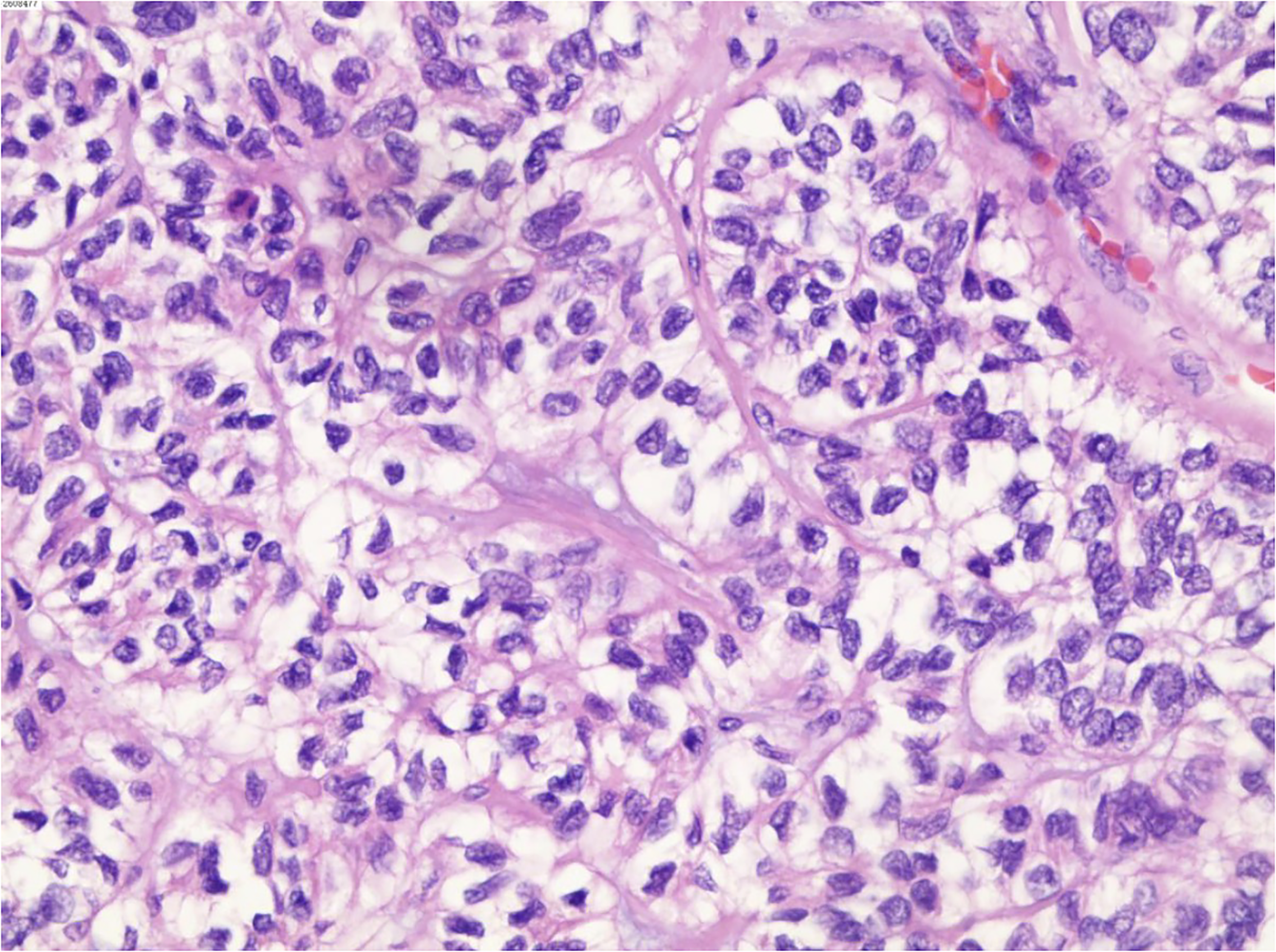
High magnification of the tumor cells in the lower right of Figure 5. The tumor cells show a solid arrangement with clear cytoplasm. Hematoxylin & eosin stain 40X magnification.

The tumor cells are cuboidal in shape, have eosinophilic cytoplasm, and possess round nuclei with prominent nucleoli. They are surrounded by proliferative connective tissue composed of coarse fibers. Hematoxylin & eosin stain 20X magnification.

The tumor cells exhibit moderate atypia, characterized by nuclear atypia and nuclear overlapping. Scattered nuclear grooves can be observed, similar to those seen in papillary thyroid carcinoma. Hematoxylin & eosin stain 40X magnification.
Kim et al. 8 compared the clinicopathological differences between uterine MLA and other types of endometrial carcinomas [endometrioid adenocarcinoma (EAC), SC, carcinosarcoma (CS)], revealing several clinicopathological features of MLA significantly different fromendometrioid adenocarcinoma, SC, and carcinosarcoma . MLA patients are older than EAC patients, MLA tumors are larger than EAC tumors, and the frequencies of deep myometrial invasion, lymphovascular space invasion (LVSI), FIGO stage III‒IV disease, and coagulative necrosis are higher in MLA than in endometrioid adenocarcinoma. Morphological clues for diagnosing MLA include: the coexistence of multiple growth patterns within the same tumor; tumor cells showing nuclear features similar to thyroid papillary carcinoma (such as nuclear grooves, overlapping, and open chromatin); the presence, at least locally, of dense eosinophilic intraluminal secretions within tubular structures (these secretions are positive for periodic acid–Schiff (PAS)); tumor cells lacking significant nuclear atypia and pleomorphism; and the absence of definite squamous differentiation.12–15 However, it is important to note that low-grade endometrial carcinomas with mesonephric-like differentiation (EC-MLD) can also exhibit growth patterns including solid, papillary, sex cord-like, and even tubular, and can have eosinophilic intraluminal secretions. 16 Therefore, the diagnosis of MLA and its differentiation from other tumors require the assistance of immunohistochemistry and molecular genetic techniques.
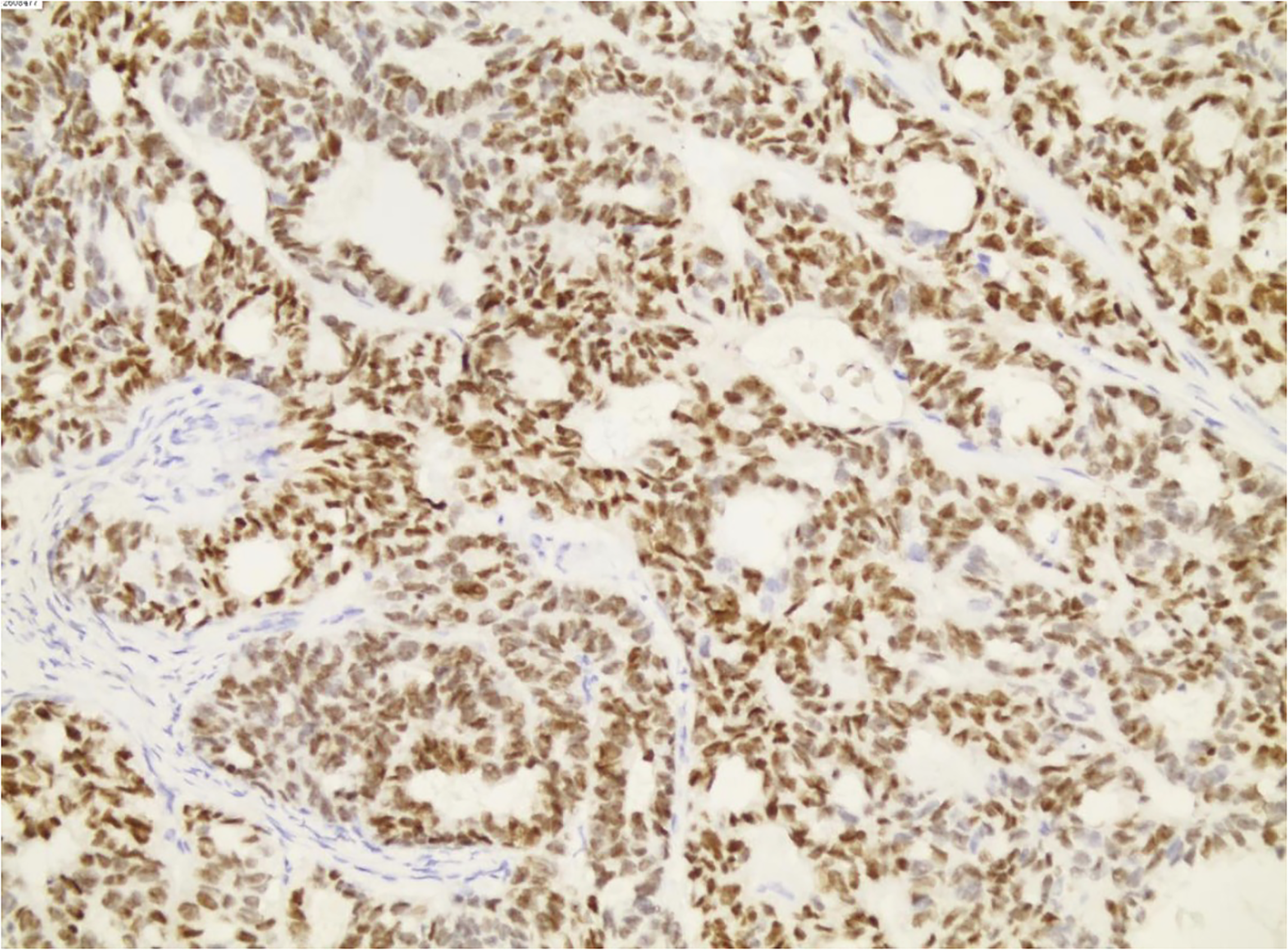
Immunohistochemistry is crucial for diagnosing MLA. When morphological findings suggest MLA, a frontline antibody panel (TTF-1, GATA3, ER, PR) can be used to help confirm the diagnosis. The typical immunophenotype of MLA is PAX8 /TTF-1(Figure 9)/GATA3 (Figure 10) positive and ER (Figure 11)/PR (Figure 12) negative. Additionally, p53 and mismatch repair protein immunohistochemistry should be performed. When tumor morphology is atypical, markers such as CD10, PAX2, and SOX17 can be considered. Existing studies show that MLA is typically positive for TTF-1 and/or GATA3 to some extent, while hormone receptor staining should be negative or only focally positive.17–20 PAX8 is consistently positive in MLA; if this marker is not diffusely positive, the diagnosis of MLA should be questioned. Luminal CD10 positivity and nuclear PAX2 positivity have also been reported in most MLA specimens.17–20 Furthermore, SOX17 has become a potentially useful stain; its negative expression helps differentiate MLA from other Müllerian tumors. However, not all MLA tumors are SOX17 negative. Additionally, p53 staining in MLA is typically wild-type, mismatch repair proteins are intact, and PTEN is mostly preserved.4,20–23

TTF-1 is positively expressed in MLA tumor cells. 20X magnification.
GATA3 is positively expressed in MLA tumor cells. 20X magnification.
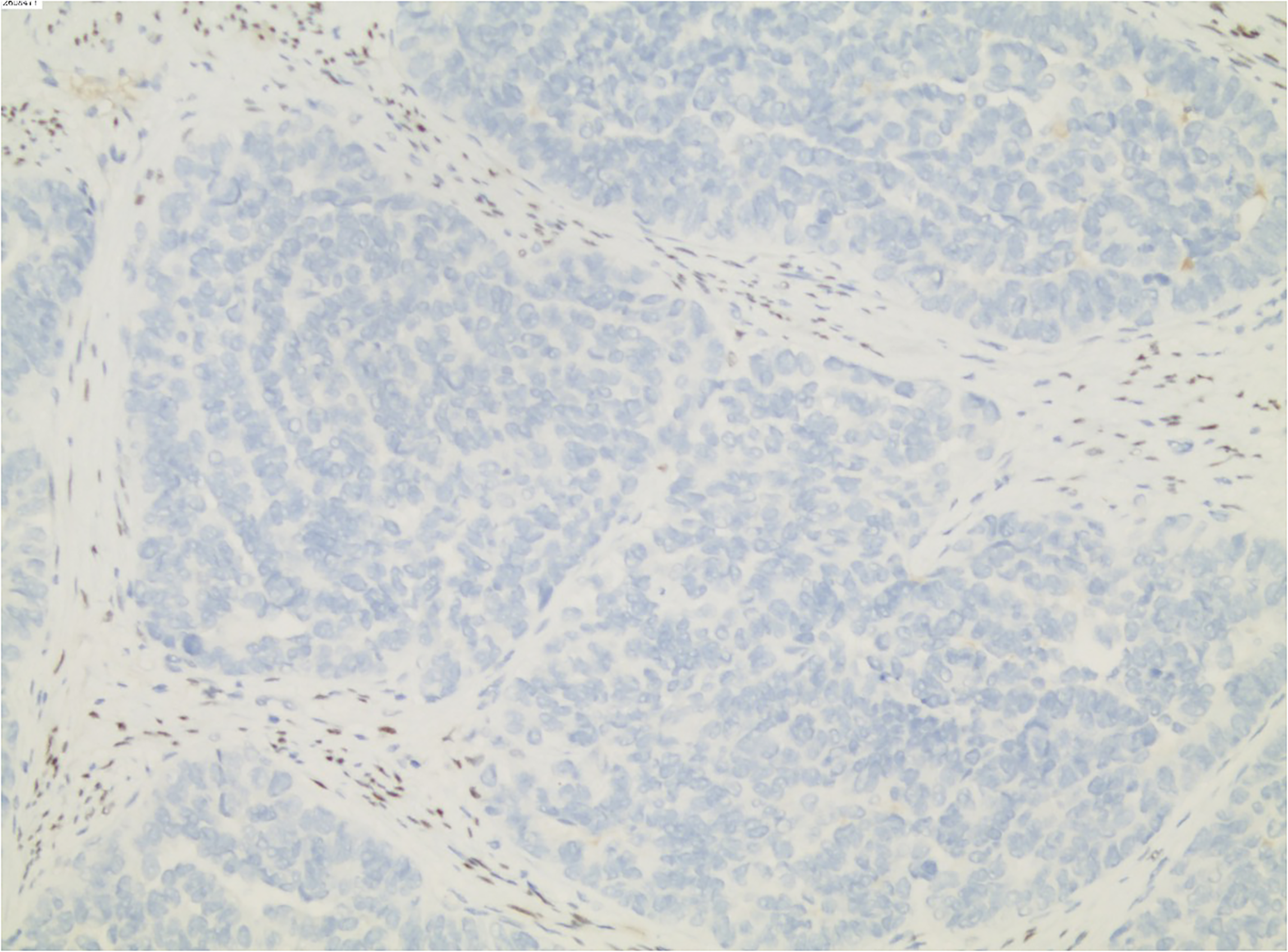
ER is negatively expressed in MLA tumor cells. 20X magnification.
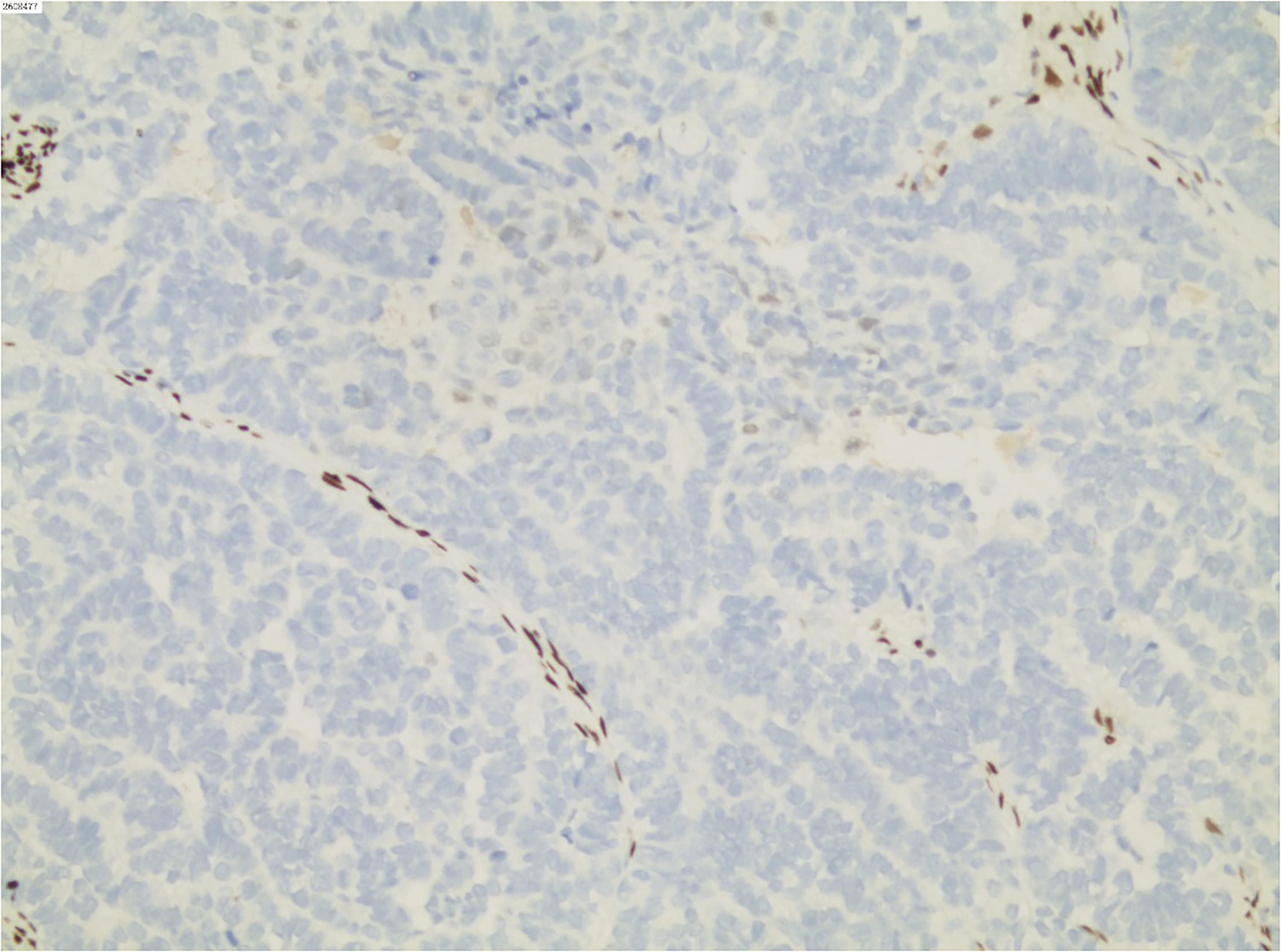
PR is negatively expressed in MLA tumor cells. 20X magnification.
Pors et al. 22 compared the sensitivity and specificity of GATA3, TTF-1, CD10, and calretinin in diagnosing MLA and found that GATA3 was the marker with the best sensitivity and specificity. However, its staining intensity in MLA was weak to moderate and could be positive in only a few cells (<10%). Euscher et al. 4 studied the immunohistochemical expression characteristics of 23 endometrial MLA specimens and obtained similar results. In their study, 15/16 (94%) and 11/16 (69%) of tumors expressed GATA3 and TTF-1, respectively. In most tumors, the staining intensity and number of positive cells for GATA3 were higher than for TTF-1. Furthermore, while MLA is typically negative for ER, some MLAs can show focal ER positivity. Therefore, focal ER positivity cannot rule out MLA. Euscher et al. 4 revealed that approximately 30% of MLAs showed focal ER positivity (usually <10% of tumor cells expressing ER). However, PR is almost always negative in MLA. In MLA, p53 shows a wild-type expression pattern, p16 is patchy positive, and WT1 is negative. SRY-box transcription factor 17 (SOX17) is a key factor in embryonic development. Recent studies have explored SOX17 expression in MLA: Tahir et al. 23 performed SOX17 immunohistochemistry on 17 confirmed MLA specimens and found that SOX17 staining in all MLAs was either negative (n = 10) or showed focal weak/moderate staining (n = 7). Compared to the diffuse strong staining of SOX17 in other endometrial carcinomas subtypes, SOX17 staining in MLA is weak and limited. Therefore, Tahir et al. 23 suggest that SOX17 immunohistochemistry has potential application value in distinguishing MLA from other endometrial carcinomas subtypes.
Molecular Genetic Characteristics of MLA
Molecularly, the vast majority of MLAs harbor KRAS mutations. According to the study by da Silva et al., 24 92% of uterine MLAs and 87% of ovarian MLAs carry somatic KRAS mutations affecting hotspot codons 12 and 13 (G12D, G12 V, G12C, G12A, and G13D). Endometrial MLAs can also harbor PTEN, CTNNB1, and ARID1A gene mutations, while ovarian MLAs can also have CTNNB1, PTEN, NOTCH3, NRAS, and PIK3CA gene mutations. The vast majority of MLA specimens lack TP53 mutations, POLE exonuclease domain hotspot mutations, and microsatellite instability, belonging to the “no specific molecular profile” (NSMP) subgroup within endometrial carcinomas.24,25
Furthermore, MLA exhibits a moderate level of genomic instability, that is, copy number variations (CNVs) involving whole chromosomes or chromosome arms. 25 Chromosomal segments with CNVs in MLA mainly include: 1q, 1p, 3q, 4p, 4q, 5p, 6q, Chr7-Chr12, 13q, 17p, 18p, 19p, 20q, 21q, and 22q. Among these, 1q, Chr10, and Chr12 are the most frequently amplified DNA segments. 25 Kommoss et al. 26 investigated the genome-wide DNA methylation patterns and CNVs of MLA. Through CNV analysis of 19 MLAs, they found gains in chromosome 1q (18/19, 95%), Chr10 (15/19, 79%), Chr12 (14/19, 74%), and Chr2 (10/19, 53%), and losses in chromosome 1p (7/19, 37%). Through unsupervised hierarchical clustering and t-Distributed Stochastic Neighbor Embedding (t-SNE) analysis of DNA methylation data, Kommoss et al. 26 found that MLA and MA clustered together, forming a distinct cluster. This cluster was clearly different from clusters of endometrioid adenocarcinoma, SC, clear cell carcinoma, and ovarian low-grade SC. These findings by Kommoss et al., 26 combined with known histological and immunophenotypic overlaps, support that MLA exhibits true mesonephric duct differentiation characteristics. They suggest adopting the more precise term “mesonephric-type adenocarcinoma” rather than MLA to name this tumor.
Differential Diagnosis of MLA
Although the vast majority of MLAs harbor KRAS mutations, KRAS mutation is not a necessary condition for diagnosing MLA, nor is it unique to MLA among endometrial carcinomas. Kolin et al. 5 conducted a molecular profiling study of 570 endometrial carcinomas and revealed that up to 17% (98/570) of endometrial carcinomas harbored KRAS mutations, most of which were endometrioid adenocarcinoma, followed by carcinosarcoma (9/570), SC (4/570), and MLA (4/570). Therefore, the diagnosis of MLA also requires close correlation with histology and immunohistochemistry. It needs to be differentiated from MA, endometrial carcinomas, clear cell carcinoma (CCC), SC, carcinosarcoma, etc.
MA
MLA needs to be differentiated from MA. Although MLA and MA have overlapping histological morphology and immunohistochemical phenotypes, they differ in primary site and other aspects. Specifically: The primary site of MLA is usually the endometrium and ovary. Literature reports that it is mostly associated with endometriosis and other Müllerian lesions, and lacks mesonephric duct remnants within. The primary site of MA is usually the cervix, and it is associated with mesonephric duct remnants. Additionally, some scholars point out that admixture with another tumor type may be a clue to an MLA diagnosis, as MA almost always occurs as a pure neoplasm.17–20 Furthermore, the immunophenotypes of MLA and MA are similar but not identical. Both tumor types are typically diffusely positive for PAX8 and CK7, show wild-type p53 expression, non-diffuse p16 expression, are negative for WT1, and are mismatch repair intact. Both are also often positive for TTF-1, GATA3, and CD10. However, MLA is more likely to be TTF-1 positive than MA. ER and PR staining may help distinguish between these two tumors, as MA is almost always completely negative, while a portion of MLAs show focal ER/PR positivity.17–19 Molecularly, both MLA and MA often harbor KRAS mutations and, less frequently, NRAS mutations. However, MLA is more often associated with other mutations, such as PIK3CA and PTEN, which are characteristic of Müllerian carcinomas, while MA usually lacks such alterations. 17
Endometrioid Adenocarcinoma
MLA and endometrioid carcinoma, especially FIGO grade 1–2 tumors, can be morphologically very similar. Both tumors can consist of glandular structures of varying complexity lined by moderately atypical cells. Most MLAs may be misdiagnosed as low-grade endometrioid carcinoma. Therefore, when MLA shows tubular or glandular structures under the microscope, it needs to be differentiated from endometrioid adenocarcinoma. EAC usually has a more uniform morphology, lacks intraluminal eosinophilic secretions, tumor nuclei are rod-shaped and stratified, sometimes with morular metaplasia, and is often surrounded by atypical endometrial hyperplasia/endometrioid intraepithelial neoplasia (EAH/EIN). EAH/EIN is a precursor lesion of endometrioid adenocarcinoma, but studies suggest that EAH/EIN can also coexist with MLA. 5 Therefore, the absence of EAH/EIN is more supportive of an MLA diagnosis, but its presence does not rule out MLA. Immunohistochemical markers ER, PR, CD10, TTF-1, and GATA3 help differentiate them. EAC is positive for ER, PR, and negative for CD10, TTF-1, GATA3; MLA is positive for CD10, TTF-1, GATA3, and negative for ER, PR. It should be noted that a small portion of endometrial carcinomas can be positive for GATA3. Pors et al. 22 reported that about 6% of endometrioid adenocarcinomas were positive for GATA3, and GATA3 expression was not diffuse but focal or patchy. These tumors were all negative for TTF-1. 22 Furthermore, studies have reported that a small portion of endometrioid adenocarcinomas can be positive for TTF-1, and endometrial carcinomas patients with TTF-1 expression are often associated with poorer prognosis. 5
Clear Cell Carcinoma
When MLA shows tubular or papillary growth patterns under the microscope, it needs to be differentiated from clear cell carcinoma. Histologically, clear cell carcinoma often shows clear cells and hobnail cells, which are rare in MLA. Additionally, clear cell carcinoma is positive for NapsinA, HNF-1β, AMACR, while MLA expresses GATA3 and TTF-1. In clear cell carcinoma, p53 protein often shows a mutant expression pattern and is often associated with loss of mismatch repair protein expression, while MLA p53 protein shows a wild-type pattern and reported MLA specimens show intact mismatch repair protein expression.
SC
When MLA shows papillary or slit-like growth patterns under the microscope, it needs to be differentiated from SC. SC tumor cells have more pronounced atypia, with numerous mitoses, and lack eosinophilic material in lumens. SC is often associated with mutant p53 expression, p16 shows diffuse block-like positivity, WT-1 shows diffuse nuclear positivity, and does not express TTF-1, GATA3, or CD10.
Carcinosarcoma
When MLA shows spindle cell components under the microscope, it needs to be differentiated from carcinosarcoma . Tumor cells in carcinosarcoma show significant atypia, while spindle cells in MLA are morphologically bland. Carcinosarcoma does not express TTF-1, may be weakly positive for GATA3, and generally does not harbor KRAS gene mutations.
Female Adnexal Tumor of Wolffian Origin (FATWO) and Adnexal Tumors with STK11 Alterations
FATWO most commonly occurs in the broad ligament and can be found in the ovary, mesosalpinx, paravaginal area, and peritoneum. Microscopically, it shows various histological structures such as cribriform, tubular, cystic, and slit-like patterns, usually with one pattern predominating, but several patterns can coexist. Eosinophilic secretions can be seen in lumens. Tumor cells are columnar or cuboidal, nuclei are round or oval with uniform chromatin; some tumors show nuclear grooves. These tumors are positive for ER and negative for PAX8, TTF-1, GATA3. 27 Adnexal tumors with STK11 alterations are located in the para-tubal area and also have various histological structures, with basophilic intraluminal secretions. These tumor cells are positive for inhibin, calretinin, and WT1 immunohistochemical markers and negative for PAX8, GATA3, and TTF-1. Molecularly, these tumors often harbor STK11 gene mutations.
Prognosis and Treatment of MLA
Regarding prognosis, MLA has aggressive biological behavior, is prone to recurrence and metastasis, and over half of the tumors are diagnosed at an advanced stage (FIGO ≥ stage II), with 43% of patients having LVSI. 28 The median progression-free survival (PFS) of uterine MLA patients is lower than that of EAC and SC patients (18.2 months vs 193 months and 67.1 months, respectively; P < .01). The PFS of uterine MLA patients is even significantly shorter than that of high-grade (FIGO grade 3) EAC patients (P < .001). 8 This type of tumor can metastasize, recur, and easily lead to patient death. The lungs are the most common distant metastasis site for uterine MLA, with up to 60% of MLAs developing lung metastases. 19 Additionally, MLA can metastasize to the liver, and the frequency of liver metastasis in MLA is 10 times that of EAC and 5 times that of SC.4,22 MLA can also metastasize to the brain, spleen, and vertebrae. 22 According to literature reports, large tumor volume (maximum diameter >4 cm), ill-defined borders, deep myometrial invasion, extensive necrosis, high mitotic index (>10/10 HPF), and presence of LVSI are associated with poor prognosis in MLA patients. 28
Regarding treatment, given the aggressive clinical behavior of MLA and the tendency for recurrence and metastasis even after surgery, studies suggest that uterine MLA should not be graded according to the FIGO grading system but should automatically be considered high-grade and treated according to high-grade endometrial carcinomas treatment protocols.4,22 Due to its rarity, there is no clear standardized treatment protocol for MLA. Most MLA patients undergo total hysterectomy with bilateral salpingo-oophorectomy, omentectomy, and pelvic lymphadenectomy. 29 Postoperative treatment includes chemotherapy, radiotherapy, or combined therapy. Paclitaxel combined with carboplatin is usually the first-line chemotherapy regimen for MLA patients. 29 As mentioned earlier, MLA occurring in the uterus and ovary is negative or only focally positive for ER/PR, indicating that hormone therapy may be ineffective in MLA. Yano et al. 11 reported a patient of endometrial carcinomas mixed with MLA who received PR therapy; the MLA component recurred 6 years later. Euscher et al. 4 reported a patient initially misdiagnosed as low-grade endometrial carcinomas who received hormone therapy (unspecified), with tumor recurrence in the liver after 17 months. It is worth mentioning that MLA often harbors KRAS gene mutations, so the use of KRAS-targeted inhibitors could be a potential treatment option for MLA patients. Recent literature reports the use of KRAS-targeted inhibitors for solid tumor patients, which can improve prognosis. 11 Sotorasib is a specific, irreversible inhibitor of the GTPase for tumors with p.G12C-KRAS mutation. Targeted therapy with sotorasib for p.G12C-KRAS mutation is only approved by the FDA and EMA for the treatment of lung cancer and colorectal cancer. 22 However, as there are currently no reports on the application of p.G12C-KRAS targeted inhibitors in MLA, and the p.G12C mutation accounts for <10% in endometrial and ovarian MLA, KRAS-G12C targeted inhibition may only provide a potential treatment option for a minority of female genital tract MLA patients. 27 Furthermore, as current surveillance strategies for endometrial carcinomas patients usually do not include chest imaging, some scholars suggest that, given the high risk of lung metastasis in MLA, chest imaging can be included in the surveillance strategy for MLA patients. 30
Summary
In summary, MLA histology can present various patterns, including tubular, glandular, spindle, solid, and papillary structures. Tumor cells are cuboidal or columnar, with crowded, overlapping nuclei showing grooves and open chromatin. At least locally, dense eosinophilic intraluminal secretions are visible within lumens. Tumor cells lack significant nuclear atypia and pleomorphism, and definite squamous differentiation is absent. Immunohistochemically, GATA3, TTF-1, calretinin, and CD10 show positive expression in tumor cells, P16 shows patchy expression, P53 shows wild-type expression, ER shows focal positive or negative expression, and PR shows negative expression. Molecularly, MLA often harbors KRAS mutations, is microsatellite stable, and frequently has gains in chromosome 1q (1q), with or without PIK3CA, PTEN, and CTNNB1 mutations. MLA has a high risk of recurrence and metastasis. Currently, specific treatment options for this tumor are limited, and the optimal treatment strategy has not been determined.
Footnotes
Ethical Approval
Not applicable, review article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.