
Abstract
Combined small cell lung carcinoma (SCLC) is not uncommon, though the combination with a second primary adenocarcinoma is less frequent. Molecular profiling can clarify clonal relationships and identify potentially actionable alterations, but interpretation requires careful integration with histologic and clinical findings. We report a 61-year-old woman with 2 synchronous right upper lobe tumors: a poorly differentiated combined SCLC with an adenocarcinoma component (cribriform 40%, acinar 30%, solid 30%) and a separate invasive adenocarcinoma (60% acinar, 40% lepidic), both staged pT1bN0M0. Core biopsy of the combined SCLC initially showed only adenocarcinoma morphology, highlighting the diagnostic limitations of undersampling in combined tumors. Molecular profiling revealed overlapping truncal alterations (TP53 C135Y, RB1 Q344, and KRAS G12C) at markedly discordant variant allele frequencies (VAF) of ∼46% in Tumor 1 versus ∼3% in Tumor 2, alongside a dominant KRAS G12V mutation unique to Tumor 2, a finding strongly associated with separate primary lung carcinomas rather than intrapulmonary metastasis. These molecular findings, interpreted in the context of field cancerization, favor independent primary tumors over clonal spread. The SCLC component dictated adjuvant cisplatin-etoposide regardless of the accompanying adenocarcinoma histology. This case report exemplifies the importance of integrated histologic and molecular evaluation, and the need to recognize potentially actionable mutations in combined SCLC. Comprehensive profiling not only clarifies clonal relationships and may guide therapeutic strategies, including in the context of recurrence or combined presentations.
Introduction
Lung cancer is a morphologically and genetically heterogeneous disease. 1 The WHO classification of thoracic tumors, fifth edition, describes combined small cell lung carcinoma (SCLC) as SCLC with an additional component of non-small cell lung carcinoma (NSCLC), including large cell neuroendocrine carcinoma (LCNEC). 2 Most commonly, the second component is LCNEC, adenocarcinoma, or squamous cell carcinoma, but it rarely consists of spindle or giant cell carcinoma. 3 In addition, a diagnosis of combined SCLC with LCNEC should specify the proportion of the tumor composed of LCNEC, which should constitute at least 10% of the total tumor volume. 4 However, although the percentage of tumors with other histologic patterns is often documented, no formal cutoff has been defined.4,5
Combined SCLC accounts for 2%–5% of SCLC patients, and adenocarcinoma represents an uncommon component, reported in only 12%–20% of patients.6,7 Synchronous primaries are reported in 0.5% of lung cancer patients, and the coexistence of a combined SCLC with a synchronous separate primary adenocarcinoma is rarer still, with prior reports limited to isolated instances with varying levels of detail. 8 Studies such as that by Simbolo et al (n = 13) have largely focused on solitary combined SCLC tumors, identifying KRAS mutations in a subset and TP53 and RB1 inactivation in all patients. 9 TP53 inactivation has been observed in 92% of SCLC patients and RB1 inactivation in 74% of SCLC patients, while KRAS mutations occur in 20%–40% of lung adenocarcinoma patients, providing a reference framework for interpreting shared versus tumor-specific alterations in synchronous presentations.10,11
We present this case report to illustrate 3 clinically important principles: the diagnostic pitfalls of biopsy undersampling in combined tumors, the interpretive complexity of shared truncal mutations between synchronous tumors with distinct histology, and the principle that the small cell component dictates therapy.
Here, we describe a 61-year-old woman with a 22-pack-year smoking history who was found to have 2 synchronous right upper lobe tumors: a combined SCLC with an adenocarcinoma component and a separate invasive adenocarcinoma.
Case Report
Clinical Presentation
A 61-year-old woman with a 22-pack-year smoking history presented to the emergency department for a femur fracture. A CT scan of the chest, abdomen, and pelvis revealed an incidental 1.2-cm spiculated nodule in the right lung apex (later designated as Tumor 1) and a 1.3-cm ground-glass nodule in the posterior right upper lobe (later designated as Tumor 2). Both nodules were monitored using surveillance imaging for approximately 1 year, during which they demonstrated interval enlargement. CT-guided core needle biopsy of the apical nodule revealed adenocarcinoma morphology, which was the only component identified at the time. MRI of the brain revealed no metastasis. The patient subsequently underwent right upper lobectomy, which identified a 1.7 × 1.5 × 1.2 cm lesion reclassified as combined SCLC with an adenocarcinoma component and a separate 1.3 × 0.7 × 0.6 cm adenocarcinoma 0.7 cm away from the combined SCLC. She completed adjuvant cisplatin–etoposide chemotherapy with an uneventful postoperative recovery. The tumor board recommended ongoing surveillance of a stable left upper lobe ground-glass nodule that remained unchanged on follow-up.
Histopathology
Tumor 1 was a poorly differentiated combined SCLC with an acinar adenocarcinoma component observed at low-power magnification (Figure 1A). At intermediate magnification (Figure 1B and C), acinar growth patterns were present in the adenocarcinoma component (30%). High magnification highlights the cribriform pattern (40%) with atypical cuboidal to columnar cells (Figure 1D) and SCLC with scant cytoplasm, finely granular chromatin, nuclear molding, brisk mitotic figures, and necrosis (Figure 1E). A solid pattern (30%) was also observed, although only the cribriform pattern was illustrated in the figures. Tumor 1 showed tumor spread through airway spaces (STAS) but no visceral pleural or lymphovascular invasion. All surgical margins and sampled lymph nodes (n = 16) were negative for metastasis. Pathologic stage: pT1bN0M0, grade 3.

Tumor 1: combined SCLC. (A) 2×, H&E; (B) 10×, H&E; (C) 20×, H&E. White arrows indicate SCLC component; arrowheads indicate adenocarcinoma component. (D) Adenocarcinoma component, 40×; (E) SCLC component, 40×.
Tumor 2 was a moderately differentiated invasive adenocarcinoma composed of approximately 60% acinar and 40% lepidic patterns (Figure 2A). A closer view shows acinar architecture with glands having a central lumen space surrounded by tumor cells within desmoplastic stroma, along with areas of lepidic growth in which tumor cells line pre-existing alveolar walls (Figure 2B). Tumor 2 showed no STAS, visceral pleural invasion, or lymphovascular invasion. All surgical margins and sampled lymph nodes (n = 16) were negative for metastasis. Pathologic stage: pT1bN0M0, grade 2.

Tumor 2: invasive acinar adenocarcinoma. (A) 4×, H&E; (B) 20×, H&E.
Both Tumor 1 and 2 were staged as separate primaries based on their invasive carcinoma size of 1.7 cm and 1.3 cm, respectively. The lepidic component size in Tumor 2 was not subtracted from the total invasive tumor size.
Immunohistochemistry
Immunohistochemistry of Tumor 1 (Figure 3) showed that tumor cells in the small cell component were positive for KRT7, chromogranin (CHGA) (Figure 3A), synaptophysin (SYP) (Figure 3D), and TTF-1 (NKX2-1) (Figure 3E). The Ki-67 (MKI67) proliferation index (Figure 3C) was high (>90%). The adenocarcinoma component was positive for KRT7 (Figure 3B) and TTF-1 (Figure 3E). The proliferation index, seen with Ki-67 (Figure 3C) was low to moderate. The carcinoma cells were negative for synaptophysin and chromogranin.

The immunohistochemical profile of the combined SCLC (adenocarcinoma left, SCLC right) shows (A) chromogranin positivity, (B) KRT7 positivity, (C) Ki-67 positivity, (D) synaptophysin positivity, (E) TTF-1 positivity.
CT-guided biopsy of Tumor 1 revealed adenocarcinoma morphology, TTF-1 and Napsin A (NAPSA) positivity, p40 (TP63) negativity, and no evidence of a small cell component. At resection, both small cell and adenocarcinoma components were identified in the tumor.
Molecular Findings
Molecular profiling was performed using FoundationOne CDx (F1CDx; Foundation Medicine, Cambridge, MA), performed exclusively as a laboratory service on the Illumina NovaSeq platform. DNA was extracted from formalin-fixed paraffin-embedded (FFPE) tumor samples using an automated DNA/RNA co-extraction methodology. The assay employs hybrid capture-based sequencing covering all coding exons of 309 cancer-related genes, 1 promoter region, 1 non-coding, and select intronic regions from 34 commonly rearranged genes.
F1CDx for Tumor 1 on the lobectomy identified KRAS G12C (variant allele frequency [VAF]: 46%), TP53 C135Y (VAF: 47%), and RB1 Q344 (VAF: 39%) mutations, with microsatellite stability and a tumor mutational burden (TMB) of 11 mutations per megabase. Comprehensive profiling of the lobectomy specimen confirmed these alterations and revealed additional alterations, including PIK3CA E542 K, PIK3CA E545 K, MYD88 S219C, and RB1 E691.
F1CDx performed on Tumor 2 demonstrated overlapping driver events with Tumor 1, particularly KRAS G12C (VAF: 3%), TP53 C135Y (VAF: 2%), and RB1 Q344 (VAF: 3%). In addition, Tumor 2 harbored distinct alterations with significant VAF: a separate KRAS G12 V (VAF: 23%), NF1 K1099 (VAF: 21%), RBM10 K383fs*102 (VAF: 23%), and SDHA S2 (VAF: 23%). Tumor 2 had a lower TMB (6 mutations per megabase) and was also microsatellite stable.
No alterations were detected in ALK, BRAF, EGFR, ERBB2, MET, RET, or ROS1 in either tumor. A complete summary of the shared and distinct molecular alterations was presented in Table 1.
Molecular Alterations Identified in Tumor 1 (Biopsy and Resection): Combined SCLC and Tumor 2 (Resection): Pure Adenocarcinoma.
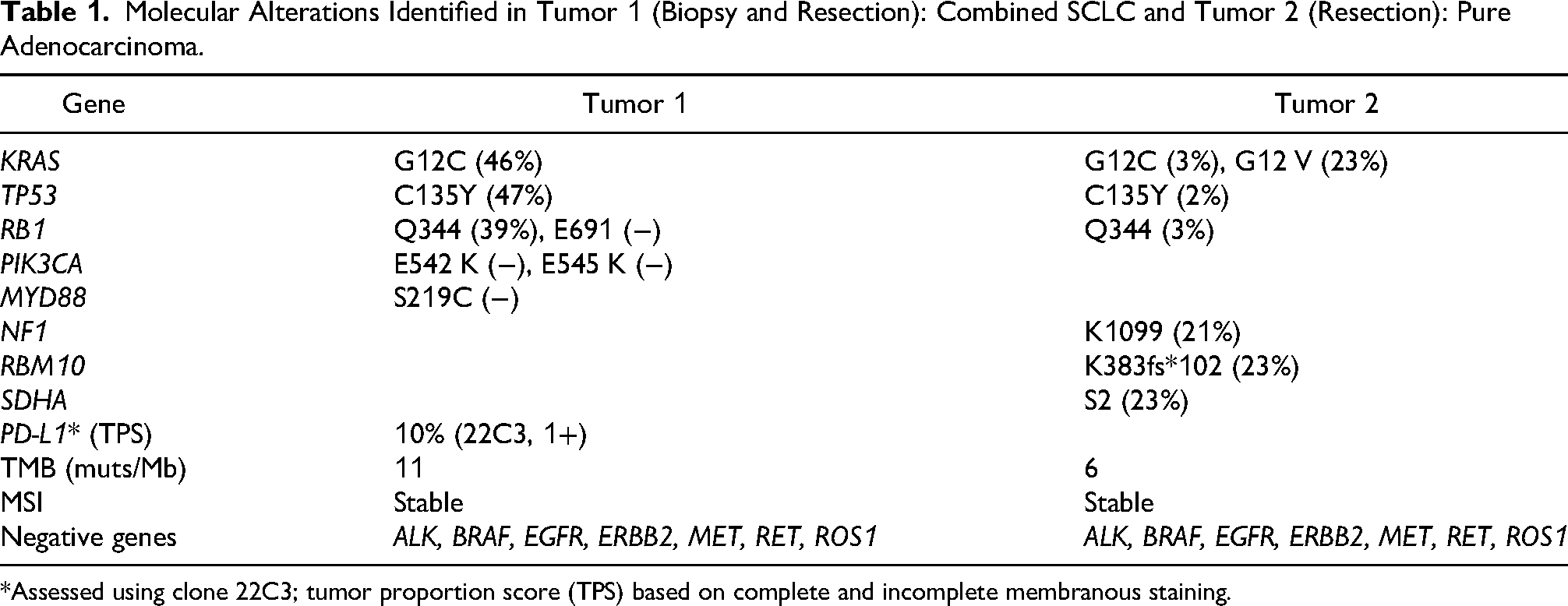
*Assessed using clone 22C3; tumor proportion score (TPS) based on complete and incomplete membranous staining.
Discussion
The molecular findings in our specimens raise the question of whether these tumors represent separate primary lung cancers (SPLC) or intrapulmonary metastases (IPM). Chang and Rekhtman proposed a stepwise algorithm integrating histologic and molecular assessment to distinguish SPLC from IPM, utilizing broad-panel next-generation sequencing (NGS). 12 Although this algorithm was developed for NSCLC-NSCLC comparisons and has not been validated for combined SCLC presentations, we applied its underlying molecular principles to assess clonal relationships in this patient. In this patient, 3 alterations were shared, which would typically suggest IPM. However, several factors argue against this classification. First, the tumors exhibited distinct histologic features. Notably, although adenocarcinoma and SCLC remain morphologically distinguishable with adequate sampling, the molecular overlap in this tumor blurs the biological distinction, underscoring the need for comparative molecular profiling beyond histology alone. Second, although KRAS G12C, TP53 C135Y, and RB1 Q344 were shared between Tumor 1 and Tumor 2, their VAF in Tumor 2 was markedly lower (∼3% vs ∼46% in Tumor 1), suggesting that these represent a minor subclone rather than the dominant tumor population. A true metastasis would be expected to carry truncal mutations at dominant VAFs. Third, Tumor 2 contained a separate KRAS G12 V at a notable VAF of 23%, discordant from the KRAS G12C mutation of Tumor 1, a finding strongly associated with SPLC rather than IPM. 13 In addition, each tumor harbored distinct private alterations not found in the other, further supporting divergent evolutionary trajectories (Table 1). Importantly, although the close proximity of the 2 tumors (0.7 cm) could raise concern for intrapulmonary spread on anatomic grounds, anatomic location alone is not a reliable criterion for distinguishing IPM from SPLC. 13
The NCCN and International Association for the Study of Lung Cancer (IASLC) Pathology committee guidelines note that shared common smoking-related mutations must be interpreted cautiously, as these may arise independently under field cancerization rather than indicating true clonal origin.14,15 These points support either monoclonal origin with branched evolution or independent primaries arising under field cancerization from smoking—models that are not mutually exclusive. This patient exemplifies the well-recognized risk of synchronous smoking-related lung cancers, in which carcinogen-induced field cancerization predisposes the entire bronchial epithelium to independent tumorigenic events, potentially yielding histologically and molecularly distinct primaries within the same lung. Transdifferentiation is less likely given the absence of EGFR mutations and no prior tyrosine kinase inhibitor exposure. 16
This case report also underscores a critical sampling pitfall. The CT-guided core biopsy of Tumor 1 revealed only adenocarcinoma morphology, with no evidence of a small cell component. This finding is consistent with reported concordance rates between biopsy and resection histology as low as 67%. 17 In our patient, the biopsy-based diagnosis of adenocarcinoma led to surgical resection, which revealed the SCLC component. Under NCCN guidelines and because the final pathologic stage was pT1bN0M0 with pathologic lymph node staging negative, the patient remained a surgical candidate with appropriate adjuvant cisplatin-etoposide. 12 However, in higher stage presentations, failure to identify a small cell component on biopsy could shift management away from concurrent chemoradiotherapy toward inappropriate surgical resection.
Regardless, accurate identification of the SCLC component is essential, as combined SCLC is treated according to SCLC protocols, even with accompanying NSCLC histology. 14 Outcomes remain poor, with 5-year survival around 40% even after surgery and chemotherapy. 7 In KRAS G12C-mutant NSCLC, selective inhibitors such as sotorasib have demonstrated clear benefit over docetaxel in the second-line setting. 18 In our patient, 1 tumor harbored KRAS G12C, which could be targetable, while the other contained KRAS G12 V, for which no approved agents exist. 19 Investigational pan-KRAS or MAP2K1/MAP2K2 (MEK)-directed therapies may eventually expand options. These findings highlight the value of comprehensive profiling in combined SCLC, both for uncovering biology and for identifying nonstandard therapeutic avenues.
A limitation of this study is that the molecular profiling of Tumor 1 was performed on bulk tissue without microdissection of the individual SCLC and adenocarcinoma components. Separate NGS testing of each would clarify whether the shared mutations are present in both components and identify component-specific subclonal alterations. While microdissection or single-cell sequencing would enhance understanding of clonal relationships, these techniques are not always feasible in routine practice and may have limited impact in immediate clinical decision-making. Future studies should evaluate whether component-specific profiling identifies actionable alterations that could inform therapy at recurrence.
Conclusion
We present a patient with combined SCLC and a synchronous adenocarcinoma that illustrates the importance of integrated histologic and molecular assessment for accurate diagnosis and treatment in synchronous and combined presentations. Biopsy undersampling represents a significant pitfall in combined tumors. In higher stages, failure to identify a small cell component could fundamentally alter treatment. The overlapping truncal mutations (TP53, RB1, KRAS) with distinct subclonal events are consistent with either branched evolution from a common progenitor or independent primaries arising under field cancerization; these models cannot be distinguished based on bulk sequencing alone. Future multi-region or single-cell sequencing studies will be needed to resolve clonality questions and test whether a trunk-and-branch evolutionary model underlies such presentations. Profiling may also identify actionable alterations that could inform therapeutic strategies in the recurrent or metastatic setting.
Footnotes
Ethical Approval
Ethical approval was waived by the UC Davis Institutional Review Board, as this is a deidentified single case report based on retrospective review of existing clinical and pathologic material, which does not meet the threshold for full IRB review under institutional guidelines.
Consent for Publication
Written informed consent for publication of clinical details and images was obtained from the patient. Identifying information has been anonymized to protect privacy.
Author Contributions
Robin Chang: conceptualization, data curation, writing–original draft, and writing–review and editing. Alejandro S. Mendoza: resources, data curation, and writing–review and editing. Swikrity U. Baskota: investigation, methodology, resources, supervision, validation, and writing–review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data relevant to this case report are included within the article. Additional details are available from the corresponding author upon reasonable request.