
Abstract
Mucinous cystadenocarcinoma of the breast is rare and has been recently classified as a distinct entity in the fifth edition of the WHO Classification of Tumors. Here, we present a 47-year-old woman with a history of NST carcinoma in her right breast who subsequently developed a lump in the right chest wall close to the breast implant. Immunohistochemical analysis showed negativity for keratin 20 and CDX2, and positivity for mammaglobin, GCDFP15 and TRPS1 with a triple-negative phenotype. The diagnosis of primary mucinous cystadenocarcinoma of the breast was finally established. Next-generation sequencing identified likely pathogenetic mutations specifically in AKT1, EGFR, FANCA, BCL10, CTCF and RUNX1 and RP1-34H18.1::NAV3 gene fusion, making this as the first reported example in the literature harboring an RP1-34H18.1::NAV3 gene fusion identified within a comprehensive RNA-based molecular analysis, representing the 49th reported patient worldwide.
Introduction
Primary mucinous cystadenocarcinoma (MCA) of the breast is extremely rare. It was first described by Koenig and Tavassoli in 1998 1 and recognized as a distinct entity in the fifth edition of the WHO classification of tumors of the breast in 2019. 2 To date, only 49 patients with this diagnosis have been reported in the literature, including the one we here describe. Histologically MCA of the breast resembles its pancreatobiliary or ovarian counterparts, as it is composed of tall columnar cells with basal, bland nuclei and abundant intra- and extracytoplasmic mucin. According to the current literature, MCA of the breast predominantly affects female patients, with a reported age range of 41 to 63 years, with a favorable prognosis and no distant metastasis despite a triple-negative immunophenotype, lacking expression of estrogen receptor ER (ESR1), progesterone receptor PR (PGR), and HER2 (ERBB2).
Patient Presentation
Herein we present the case report of a 47-year-old woman with a history of luminal-B/HER2 negative invasive carcinoma of no special type (NST) in her right breast, diagnosed 5 years prior to the current presentation, treated with primary chemotherapy (PCT) and nipple-sparing mastectomy with breast implant. Approximately 5 years after the initial diagnosis, a firm 2-cm lump was detected in the right chest wall, adjacent to the breast implant. On ultrasound examination, the mass appeared well circumscribed. Follow-up exams, including a whole-body CT scan as well as abdominal and gynecological ultrasound examinations, excluded any possible extramammary origin, in particular the ovaries, the lungs and the pancreatobiliary tract. Germline genetic testing was negative, and no cancer predisposition was identified.
On gross examination of the surgical specimen, 2 distinct lesions measuring approximately 1.5 and 0.6 cm were identified in close proximity to each other. Both were well circumscribed and showed a white, gelatinous cut surface. The lesions were separated by intervening normal adipose tissue, consistent with multifocal disease. Histologically, the tumor revealed cystic spaces with papillary projections lined by tall columnar cells with basally located bland nuclei and apical mucin. Mucin was also present within the cystic spaces. Cytological atypia was mild to moderate; mitotic figures were rare (Figure 1A–C). Residual glandular breast tissue was identified at the periphery of the lesion, supporting the mammary origin of the tumor (Figure 1D).

Morphological features, hormone receptor, and HER2 status. Multiloculated cystic lesion with abundant mucinous content and complex glandular architecture ((A), hematoxylin & eosin; magnification: 20×). Dilated cystic spaces lined by mucin-producing epithelium with papillary and glandular infoldings ((B), hematoxylin & eosin; magnification: 100×). Tall columnar cells with basally located bland nuclei ((C), hematoxylin & eosin; magnification: 400×). Adjacent normal breast epithelium ((D), hematoxylin & eosin). Immunohistochemistry showing negative expression for estrogen receptor (ER) (E), progesterone receptor (PgR) (F), and HER2 (G), consistent with a triple-negative phenotype (magnification: 200×). Scale bars: 20 µm.
A wide range of immunohistochemistry panels were performed, revealing negativity for keratin 20, CDX2, CA19.9, PAX8 and WT1, and positivity for mammaglobin, GCDFP15 and TRPS1, a novel highly sensitive and specific marker for breast carcinoma, particularly a triple-negative breast cancer (TNBC), in accordance with recent literature (Figure 2). 3 Hormone receptors and HER2 status were also assessed, displaying a triple-negative immunophenotype with a proliferation index of 23% (Figure 1E–G).

Immunohistochemical profile. Diffuse cytoplasmic positivity for mammaglobin (A) and GCDFP-15 (B), together with nuclear expression of TRPS1 (C), supports mammary origin; however, GATA3 (D) and SOX10 (E) are negative. Cytokeratin staining shows diffuse cytoplasmic positivity for KRT7 (F) and patchy expression of KRT5/6 (G). Myoepithelial cells are absent, as demonstrated by negative staining for myosin (H) and p63 (I). Negative staining for PAX8 (J), WT1 (K), and CA19.9 (L) further excludes a non-mammary primary origin. Magnification of all panels: 200×; scale bars: 20 µm.
All these findings confirmed the diagnosis of primary MCA of the breast. During the multidisciplinary team meeting, a strict follow-up was recommended. After 23 months, the patient had no evidence of disease recurrence.
Molecular Analysis
Next-generation sequencing (NGS) with a multigene panel targeting 1385 genes and 21043 exonic regions, including 507 genes associated with cancer gene fusions, and with a total target size of 3.78Mb (TruSight RNA Pan-Cancer Panel, Illumina) was performed (see Supplemental Materials and Methods for details). The analysis predominantly identified missense variants (83%), followed by stop-gain mutations (14%), frameshift elongation (1%), and splice-site variants (2%) (Figure 3A). Among these, sequencing results revealed pathogenic missense mutations in AKT1 (p.E17 K), while the EGFR (p.P753S) variant showed limited evidence of pathogenicity and is currently classified as a variant of uncertain clinical significance. Conversely, the FANCA (p.S858R) mutation showed a conflicting interpretation regarding its pathogenicity. Additionally, BCL10 (p.S167Ffs*3) and CTCF (p.T204Nfs*26) were classified as pathogenetic frameshift mutations, while RUNX1 (p.R201*) was identified as pathogenic stop-gain mutation. All mutations exhibited variant allele frequencies (VAF) ≥ 5%. Notably, a previously unreported gene fusion event, RP1-34H18.1::NAV3 was also detected. This fusion involves a long non-coding RNA (RP1-34H18.1) as the 5’ partner and the protein-coding gene NAV3 as the 3’ partner, both located on chromosome 12.
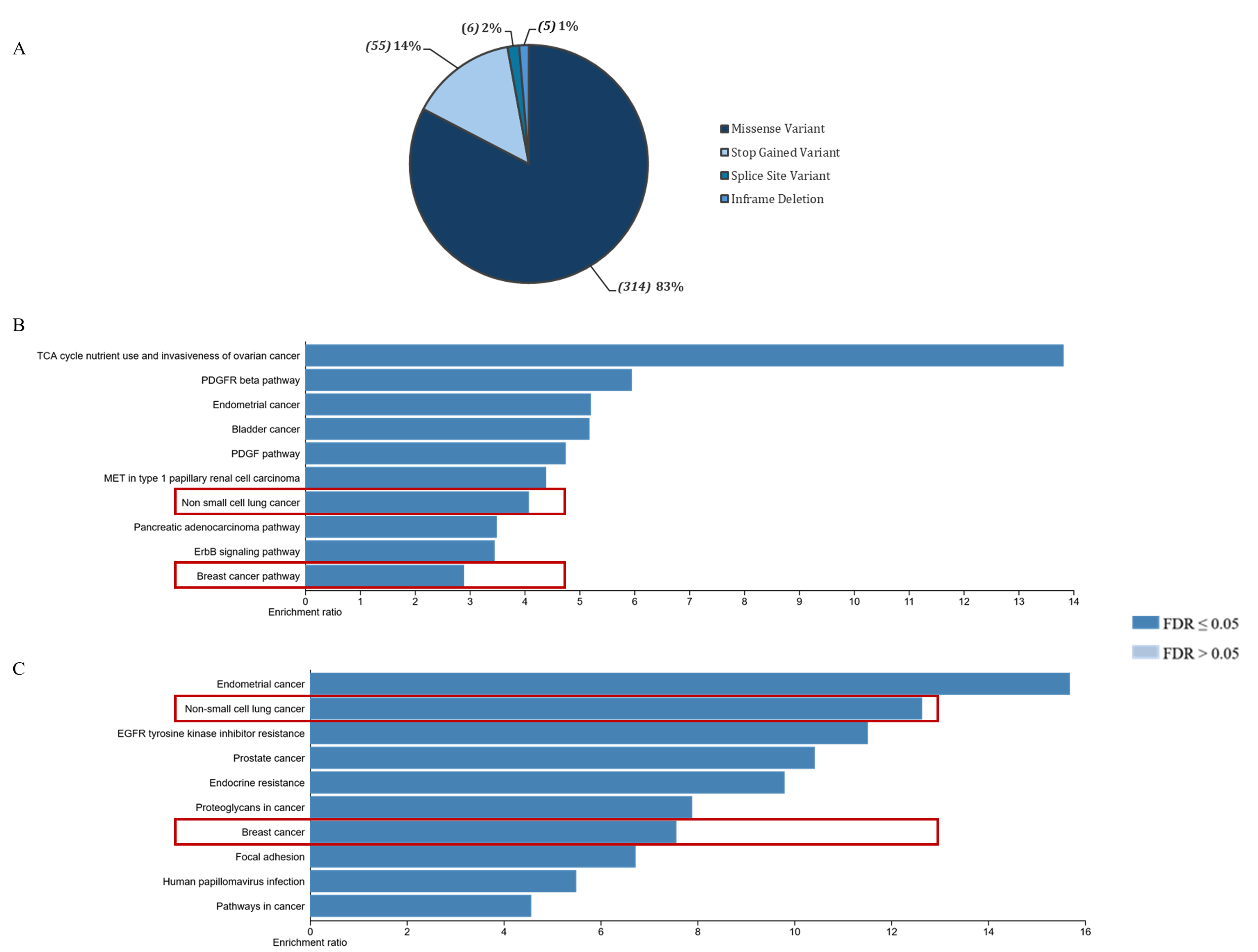
Variants detected in COSMIC Database. Distribution of 380 mutations by type, showing the percentage of missense, frameshift and stop gained variants and number of mutations for each type in brackets (A). Pathway enrichment analysis: frequency of total gene mutations in cancer-related pathways as identified through WikiPathways (B) and KEGG pathway (C). The abscissa represents the GeneRatio of the enriched pathways, the ordinate represents the name of the enriched pathways, and the color represents the significance of the FDR value. The top 10 significant pathways with FDR ≤ 0.05 were identified. The highlighted red boxes indicate the enriched pathways that overlap across distinct databases.
To further understand the biological functions of the identified genes, WikiPathways and KEGG enrichment analyses were performed. The WikiPathways analysis revealed that the top 10 most represented pathways were associated with TCA cycle nutrient use and invasiveness of ovarian cancer, non-small cell lung cancer (NSCLC), and breast cancer (Figure 3B). Likewise, the KEGG analysis highlighted pathways predominantly related to NSCLC and breast cancer (Figure 3C).
Discussion
Primary MCA of the breast is an exceptionally rare entity that requires careful distinction from other primary mucin-producing and cystic breast carcinomas, as well as from metastatic mucinous tumors, due to important diagnostic, therapeutic, and biological implications. The main differential diagnosis includes classic (pure) mucinous carcinoma. The latter is characterized by small clusters or nests of tumor cells floating in abundant extracellular mucin and typically demonstrates strong and diffuse ER and PR expression, consistent with luminal-type differentiation. In contrast, MCA of the breast exhibits multiloculated cystic spaces lined by tall columnar mucin-rich epithelial cells with stratification, tufting, and occasional papillary formations. A defining feature of MCA of the breast is the presence of abundant intracytoplasmic mucin within the lining cells, in addition to mucin within the cystic lumina. Furthermore, the cystic structures lack a peripheral myoepithelial layer, supporting invasive growth. Immunohistochemically, most reported MCAs of the breast are negative for ER and PR and frequently display a triple-negative phenotype, highlighting their biological divergence from classic mucinous carcinoma and their distinct therapeutic implications, particularly with regard to endocrine therapy. MCA must also be differentiated from cystic hypersecretory lesions of the breast, including cystic hypersecretory hyperplasia and cystic hypersecretory carcinoma. These entities are characterized by dilated ducts containing dense eosinophilic, colloid-like secretions and represent a spectrum ranging from benign proliferations to in situ and invasive carcinoma. Unlike MCA, cystic hypersecretory lesions are primarily duct-centered processes with characteristic secretory material rather than true mucinous epithelial differentiation with abundant intracytoplasmic mucin and a cystadenocarcinoma-like architecture. Recognition of this distinction is important, as cystic hypersecretory carcinoma is generally regarded as a variant within the spectrum of ductal carcinoma in situ with possible invasion, whereas MCA represents a distinct invasive mucin-producing carcinoma of the breast. The distinction from papillary carcinomas, including encapsulated and solid papillary carcinoma of the breast, is likewise essential. Although focal papillary architecture may be present in MCA of the breast, it does not represent a true papillary neoplasm. Papillary carcinomas typically demonstrate fibrovascular cores and are usually strongly ER/PR positive, reflecting luminal differentiation. In addition, they lack the prominent intracytoplasmic mucin that characterizes MCA of the breast. Finally, exclusion of metastatic mucinous tumors—particularly of pancreatobiliary, appendiceal, or ovarian origin—is mandatory, especially in the absence of an associated in situ component (eg, DCIS). Clinicoradiologic correlation and appropriate immunohistochemical panels are essential in this context. Primary MCA of the breast typically shows a keratin 7-positive, keratin 20-negative, and CDX2-negative immunophenotype, whereas metastatic gastrointestinal (appendiceal neoplasms included) or pancreatobiliary tumors more commonly express keratin 20 and/or CDX2; ovarian mucinous tumors strongly express CA19.9, may express PAX8, and are negative for WT1. 2 Correct identification of a metastatic lesion is critical, as it profoundly alters staging, prognosis, and systemic management. Overall, accurate recognition of MCA of the breast and its distinction from morphologically overlapping entities is essential to avoid diagnostic pitfalls and to ensure appropriate prognostic assessment and therapeutic decision-making. Molecular characterization of MCA of the breast remains limited in the literature. To better contextualize our findings, we compiled all published examples of primary MCA of the breast to date, including the current report (Table 1). The data from our comprehensive genomic analyses provide valuable insights into the molecular landscape of this neoplasm, contributing to a better understanding of its pathogenesis and potential therapeutic vulnerabilities. NGS analysis revealed a predominance of missense mutations, with additional stop-gain, frameshift elongations, and splice variants. Among these, several mutations were identified as pathogenic or likely pathogenic, highlighting potential drivers of tumorigenesis. One of the most notable mutations was AKT1 (p.E17 K), a well-established oncogenic alteration. AKT1 is mutated in 2% to 3% of breast and urinary bladder tumors, 4 as well as in other solid tumors, including endometrial, 5 prostate, 6 and lung 7 cancers. This mutation is known to cause constitutive activation of the PI3 K/AKT signaling pathway, which supports tumor cell survival and growth. 8 However, its detection in breast MCA may suggest a pivotal role in activating pro-survival pathways, consistent with its involvement in other subtypes of breast cancer. EGFR mutations are frequently associated with tumor progression and therapeutic resistance across various cancer types, such as NSCLC but including breast cancer, with rare disagreements. 9 However, the specific EGFR p.P753S variant identified in this tumor has limited supporting evidence regarding its oncogenic role, and its functional significance remains uncertain. The analysis also identified RUNX1 (p.R201*) mutation, a stop-gain alteration in a well-known tumor suppressor gene, 10 likely disrupting transcriptional regulatory functions, which may contribute to the loss of cell cycle control and proper differentiation. In addition, frameshift mutations were detected in BCL10 (p.S167Ffs*3) and CTCF (p.T204Nfs*26). These mutations are expected to produce nonfunctional proteins, implicating genomic instability, 11 unbalanced chromatin architecture 12 and deregulation of critical cellular pathways. Such alterations likely exacerbate the molecular disruptions that characterize breast MCA. Finally, although FANCA (p.S858R) mutation has conflicting pathogenicity interpretations, 13 its involvement in DNA repair pathways raises questions about its contribution to genomic stability in this tumor type and warrants further investigation. The pathway enrichment analyses further contextualized these genetic findings by linking them to broader biological processes relevant to MCA. One significant observation was the overrepresentation of pathways related to the TCA cycle and nutrient utilization. This might underscore the metabolic reprogramming commonly observed in cancers, including mucinous subtypes. This metabolic shift may support the high energy demands of tumor cells and facilitate biosynthetic processes necessary for proliferation. Additionally, both WikiPathways and KEGG analyses highlighted pathways associated with non-small cell lung and breast cancers. This overlap suggests that breast MCA shares molecular features with other epithelial malignancies, particularly in key processes such as cell adhesion, migration, and invasion. With respect to comparison across organs, the dominant genomic drivers reported in extramammary mucinous cystic neoplasms/cystadenocarcinomas appear to differ in emphasis. In pancreatic mucinous cystic neoplasms (the lesion class from which “pancreatic mucinous cystadenocarcinoma” typically arises), recurrent alterations most commonly involve KRAS and RNF43, with additional changes accumulating in higher-grade lesions and invasive disease (eg, TP53, CDKN2A, SMAD4), pointing toward predominant activation of MAPK signaling and disruption of tumor suppressor/cell-cycle control, while PI3K-pathway alterations can occur but are not generally highlighted as the principal recurrent event. 14 Similarly, ovarian mucinous carcinoma shows a distinct landscape characterized by frequent KRAS mutations and a substantial prevalence of TP53 alterations and ERBB2 (HER2) amplification, again suggesting that MAPK signaling and TP53/cell-cycle dysregulation are central themes; PI3K-pathway alterations may be present in some tumors but are not typically the defining feature. 15 In addition to the somatic point mutations described above, our NGS analysis identified a novel gene fusion, RP1-34H18.1::NAV3, not previously reported in MCA of the breast to our knowledge, while other recurrent mutations such as AKT1 and alterations in PI3 K pathway genes have been described in prior case series. The fusion was originally detected in glioblastoma (GBM), where NAV3 overexpression has been linked to increased invasiveness and a mesenchymal phenotype, with the fusion being detected in approximately 7% of fusion-positive GBM tumors. 16 RP1-34H18.1::NAV3 has been recently described also in endometrial cancer. 17
Literature Review for Primary Mucinous Cystadenocarcinomas of the Breast.
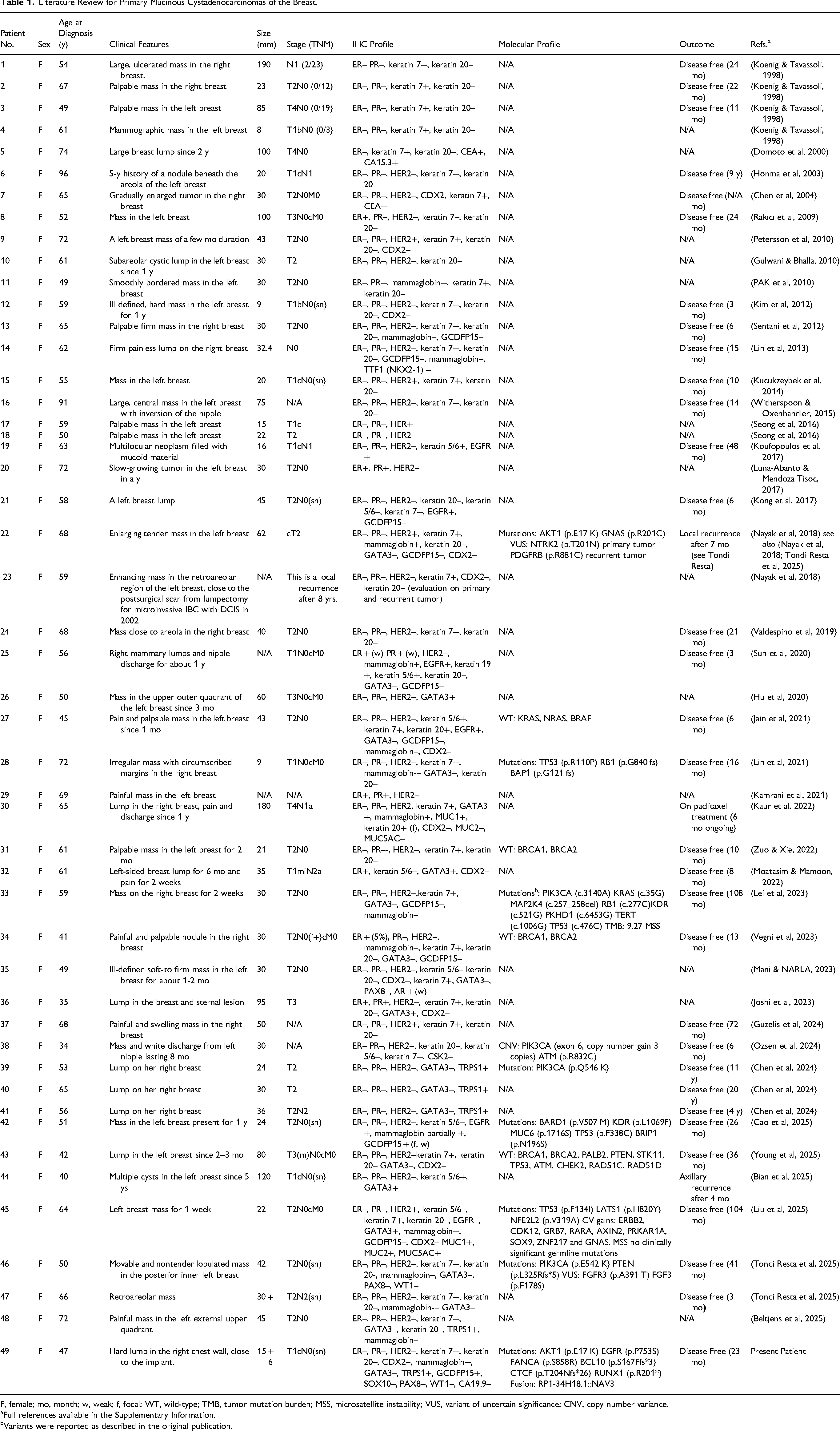
F, female; mo, month; w, weak; f, focal; WT, wild-type; TMB, tumor mutation burden; MSS, microsatellite instability; VUS, variant of uncertain significance; CNV, copy number variance.
Full references available in the Supplementary Information.
Variants were reported as described in the original publication.
NAV3 encodes a protein involved in microtubule regulation and cell migration, and its role in cancer appears highly context-dependent: it is downregulated in advanced stages of melanoma, it is altered in colorectal cancer, where copy number alterations correlate with lymph node metastasis and shorter overall survival, and recurrent somatic mutations have been recently described in endometrial carcinoma. In breast cancer, by contrast, NAV3 has been proposed to act as a tumor suppressor, regulating microtubule dynamics and promoting directional migration, thereby limiting metastatic spread. 18
Despite the comprehensive RNA-based analysis, several limitations must be acknowledged. The panel design does not allow definitive determination of the reading-frame status of the RP1-34H18.1::NAV3 fusion, and no orthogonal validation or functional assays were performed. The biological effect of the RP1-34H18.1::NAV3 fusion therefore remains uncertain. Two non-mutually exclusive scenarios may be hypothesized: an in-frame fusion might generate a chimeric protein with altered effects on cytoskeletal regulation and cell migration, whereas an out-of-frame fusion could result in truncated NAV3 protein or trigger transcript degradation via nonsense-mediated decay, effectively leading to loss of function. Given the proposed tumor-suppressive role of NAV3 in breast cancer, this latter mechanism may represent a biologically plausible scenario. Functional studies are nevertheless required to clarify its biological impact, particularly within the context of a triple-negative background. Although no metastatic disease has been observed in our patient at 23 months of follow-up, the presence of this fusion in a morphologically indolent yet genomically complex tumor raises important questions about its biological behavior and long-term clinical course. This underscores the need for rigorous clinical surveillance and may justify further research into its prognostic or therapeutic significance.
Although MCA of the breast typically shows a triple-negative immunophenotype, available data suggest a relatively favorable prognosis. This may reflect the heterogeneity of triple-negative breast cancers, as some low-grade or special-type variants exhibit indolent behavior. The presence of an AKT1 driver mutation—more commonly seen in luminal-type tumors—further suggests that the underlying biology of MCA may differ from that of conventional high-grade basal-like TNBC. However, the molecular profile identified in this study—characterized by multiple pathogenic mutations and a novel gene fusion—might reflect an increased clinical risk; therefore, a strict follow-up of the patient is necessary.
These observations offer valuable insights into the molecular basis of primary MCA of the breast, helping to lay the groundwork for future research. Overall, this report illustrates the value of incorporating RNA-based sequencing into the molecular analysis of rare tumors, as it may uncover previously unrecognized molecular alterations with potential clinical relevance.
Supplemental Material
sj-docx-1-ijs-10.1177_10668969261457877 - Supplemental material for Mucinous Cystadenocarcinoma of the Breast: A Clinicopathologic and Molecular Case Report With Literature Review
Supplemental material, sj-docx-1-ijs-10.1177_10668969261457877 for Mucinous Cystadenocarcinoma of the Breast: A Clinicopathologic and Molecular Case Report With Literature Review by Roberta Iozzo, Eugenia Belcastro, Giuseppe Nicolò Fanelli, Giovanni Fanelli, Aldo Pastore, Paolo Aretini, Elena Rossetti, Antonio Giuseppe Naccarato and Cristian Scatena in International Journal of Surgical Pathology
Footnotes
ORCID iDs
Ethical Consideration
This study was approved by the Institutional Review Board of the North Western Tuscany Area (CEAVNO) (approval number: 17770). The research was conducted ethically, with all study procedures being performed in accordance with the requirements of the World Medical Association's Declaration of Helsinki. Written informed consent was obtained from the patient for study participation and data publication.
Authors’ Contributions
R.I., E.B., G.N.F, and C.S. conceived the study; R.I. and E.B. wrote the manuscript; A.P. and P.A. analyzed molecular data; C.S and G.F. analyzed the histological data; E.R. analyzed the clinical data; C.S. and A.G.N. supervised the study and edited the manuscript. All the authors have read and approved the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Research Project PNRR “Tuscany Health Ecosystem” Ecosistema dell’innovazione sulle scienze e le tecnologie della vita in Toscana (THE)—Spoke 6: Precision Medicine & Personalized Healthcare. Personalized approaches and innovative treatments in oncology—advanced biomarkers for patient stratification. Codice Progetto: ECS00000017. Codice Unico di Progetto: I53C22000780001 (A.G.N. and C.S.).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.S. has received honoraria for consulting, advisory role, speaker bureau, and/or research grants from Bristol Myers Squibb, Astra Zeneca, Daiichi-Sankyo, Gilead, and Menarini.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.