
Abstract
Background
Early-onset colorectal cancer (CRC) is characterized by distinct molecular and clinical features, a more advanced stage at diagnosis, and unique challenges in clinical management.
Aim
This study aimed to characterize the clinicopathologic features of early-onset CRC and investigate the associations between clinicopathologic characteristics and genetic mutations in young Chinese patients.
Methods
In total, 239 young Chinese patients (age range: 22-45 years) diagnosed with CRC who underwent surgery from January 2016 to June 2022 were retrospectively enrolled. KRAS, NRAS, and BRAF mutations were detected using a mutation analysis panel kit. Mismatch repair (MMR) protein (MLH, PMS2, MSH2, MSH6) expression was evaluated by immunohistochemistry. Pearson's chi-squared test was used to assess the relationships of genetic mutations and MMR with patients’ clinicopathologic characteristics.
Results
The overall KRAS/NRAS/BRAF mutation rate was 50.6% (121/239), including individual rates of 44.4% (KRAS), 2.1% (NRAS), and 4.2% (BRAF). In addition, 15.1% of the patients (36/239) were MMR-deficient (dMMR). The BRAF V600E mutation was significantly associated with high grade (P = .012). Similarly, dMMR status showed significant associations with larger tumor size (P = .028), tumor location (P < .001), the absence of lymph node metastasis (P = .001), and the absence of distant metastasis (P = .038). KRAS mutations were more frequent in dMMR tumors than in MMR-proficient tumors (63.8% vs 40.8%).
Conclusion
Genetic mutations in the RAS/RAF pathway and dMMR status are associated with distinct clinicopathological features in patients with early-onset CRC. dMMR is a potentially favorable prognostic marker.
Introduction
Colorectal cancer (CRC) is the second most common malignancy and fourth leading cause of cancer mortality globally, and its incidence is rising notably in young populations. 1 A recent international investigation found that early-onset CRC incidence rates were rising in 27 of 50 countries. 2 Results from the Global Burden of Disease Study 2019 revealed that the global incidence of early-onset CRC more than doubled within 20 years. 3 These findings highlight the need to understand the molecular characteristics of young patients with CRC to guide precision medicine.
Carcinogenesis involves the accumulation of genetic alterations mediated through genomic instability. CRCs are molecularly classified into chromosomal instability and microsatellite instability (MSI) subtypes, with MSI (15%-20% of tumors) resulting from deficient mismatch repair (dMMR), which drives hypermutation. 4 Microsatellite instability-high (MSI-H) tumors demonstrate increased sensitivity to immune checkpoint inhibitors, informing current treatment strategies.5-6 Critically, early-onset CRC exhibits accelerated carcinogenesis through age-dependent epigenetic-metabolic crosstalk, a dimension absent in traditional classification frameworks.
Key biomarkers such as KRAS proto-oncogene, GTPase (KRAS), NRAS proto-oncogene, GTPase (NRAS), and B-Raf proto-oncogene, serine/threonine kinase (BRAF) mutations, and the MSI status, play pivotal roles in guiding treatment decisions.7–9 Mutation rates in these pathways vary significantly. KRAS mutation is observed in approximately 40% of patients with CRC, versus a rate of only 3% for NRAS mutation. 10 BRAF mutation has been identified in 10% of patients with CRC, and it is associated with the MSI status and poor prognosis. 11 The epidermal growth factor receptor (EGFR)-mediated signaling cascade plays a pivotal role in colorectal carcinogenesis, with the hyperactivation of this pathway observed in 60%-80% of patients, making EGFR a critical therapeutic target.12–14 Contemporary clinical practice has incorporated EGFR-targeted monoclonal antibodies into CRC treatment regimens, as these antibodies interrupt intracellular EGFR signal transduction pathways. 15 Although the genomic landscape of CRC has been well-documented globally, significant heterogeneity exists in mutation patterns across different geographic regions and ethnic groups.
Previous studies have revealed significant ethnic and geographic variations in mutation patterns, with important clinical implications. A large cohort study in China demonstrated mutation rates of 45.4%, 3.9%, and 3.1% for KRAS, NRAS, and BRAF, respectively, which differed significantly from the findings in Western populations. 16 Despite the well-documented genomic landscape of CRC, the molecular characteristics of sporadic early-onset CRC among Asian populations remain inadequately characterized, particularly regarding the interplay between RAS pathway alterations and MMR status.17–20
Early-onset CRC presents distinctive challenges in clinical management, as it is characterized by insidious symptoms, aggressive progression, early metastatic spread, heightened malignancy potential, and diagnostic challenges. Consequently, most patients are diagnosed at an advanced stage.21,22 In this study, we investigated the mutation status of KRAS, NRAS, and BRAF, along with the MMR status, in 239 Chinese patients with early-onset CRC who underwent surgery at our hospital between January 2016 and June 2022. Our objectives were to determine the frequencies of these genetic mutations and to evaluate their associations with clinicopathologic characteristics in this population. The findings provide valuable insights into the molecular characteristics of patients with early-onset CRC.
Materials and Methods
Patients
This retrospective study consecutively enrolled 239 young patients (≤45 years) with histopathologically confirmed colorectal adenocarcinoma who underwent curative-intent R0 resection at Guangdong General Hospital (Guangzhou, China) between January 2016 and June 2022. Individuals who received any neoadjuvant therapy (chemotherapy, radiotherapy, or molecular targeted agents such as anti-EGFR/VEGF inhibitors) prior to surgery, those with secondary malignancies, those who underwent non-curative resection (R1/R2), and those with incomplete clinical or molecular data were excluded. During the surgeries, tissue specimens were collected for histopathological evaluation. Clinicopathologic data were retrieved from the electronic medical records and pathology reports of the enrolled patients, including demographic information (age and sex), tumor characteristics (size, morphologic features, histologic grades), lymphovascular invasion, perineural invasion, and distant metastasis. Written informed consent was obtained from all participants, and this investigation was approved by the Ethics Committee of Guangdong General Hospital (S2025-296-01).
Histology and Immunohistochemistry
After surgical dissection, colorectal specimens were fixed in 10% buffered formalin, after which tumor sizes were measured. Subsequently, the specimens were embedded in paraffin and processed for hematoxylin and eosin (H&E) staining. All specimens were independently reviewed by three highly experienced pathologists according to the World Health Organization classification of tumors of the digestive system, 23 with discrepancies resolved by multi-headed microscope consensus.
For MMR status assessment, immunohistochemistry was performed on a Dako Autostainer Link 48 platform (Agilent, Santa Clara, CA, USA) using EnVision FLEX detection with the following antibodies: anti-mutL homolog 1 (MLH1) (M1 clone, 1:100), anti-postmeiotic segregation increased 2 (PMS2) (A16-4, 1:100), anti-mutL homolog 2 (MSH2) (G219-1129, 1:100), and anti-mutS homolog 6 (MSH6) (SP93, 1:100; all VENTANA). Any detectable immunohistochemical staining in tumor cells was considered positive. Two pathologists, blinded to the clinicopathologic information, independently evaluated the immunohistochemical staining results.
KRAS/NRAS/BRAF Mutation Detection
Mutation analysis was performed using formalin-fixed, paraffin-embedded (FFPE) tissues containing at least 10% tumor cells, as determined by pathological evaluation of H&E-stained sections. Genomic DNA was extracted from the selected FFPE samples using the QIAamp DNA FFPE Tissue Kit (Qiagen, Hilden, Germany) following the manufacturer's instructions. The mutational status of KRAS [exons 2 (codons 12-13), 3 (codon 61), and 4 (codons 117 and 146)], NRAS [exons 2 (codon 12) and 3 (codon 61)], and BRAF [exon 15 (codon 600)] was analyzed using the ADx KRAS/NRAS/BRAF Mutation Analysis Panel Kit (AmoyDx, Xiamen, China). Target amplification was conducted on a VeritiPro Thermal Cycler (Thermo Fisher Scientific, Waltham, MA, USA), and the polymerase chain reaction products were sequenced on a PRISM 3100 Genetic Analyzer (Thermo Fisher Scientific). Mutations were identified by comparing amplification levels with those of positive and negative controls in accordance with the manufacturer's established criteria.
Statistical Analysis
The associations between molecular events (KRAS/NRAS/BRAF mutation and MMR status) and clinicopathologic features were determined using Pearson's chi-squared test. Statistical analyses were performed using SPSS software (Version 26, IBM Corporation, Armonk, NY, USA). P < .05 was considered statistically significant.
Results
Clinicopathologic Features
To assess the demographic and clinical features of early-onset CRC, data from a cohort of 239 patients with early-onset CRC were analyzed. The detailed clinicopathologic characteristics of the patients are summarized in Table 1. The enrolled population consisted of 144 men (60.3%) and 95 women (39.7%) aged 22-45 years. The cohort included 62 rectal cancers and 177 colon cancers, and the most common location of colon cancers was the sigmoid colon (71 patients, 29.7%), followed by the ascending colon (48 patients, 20.1%).
Clinical Characteristics and Molecular Features of 239 Young Patients with Colorectal Cancer.
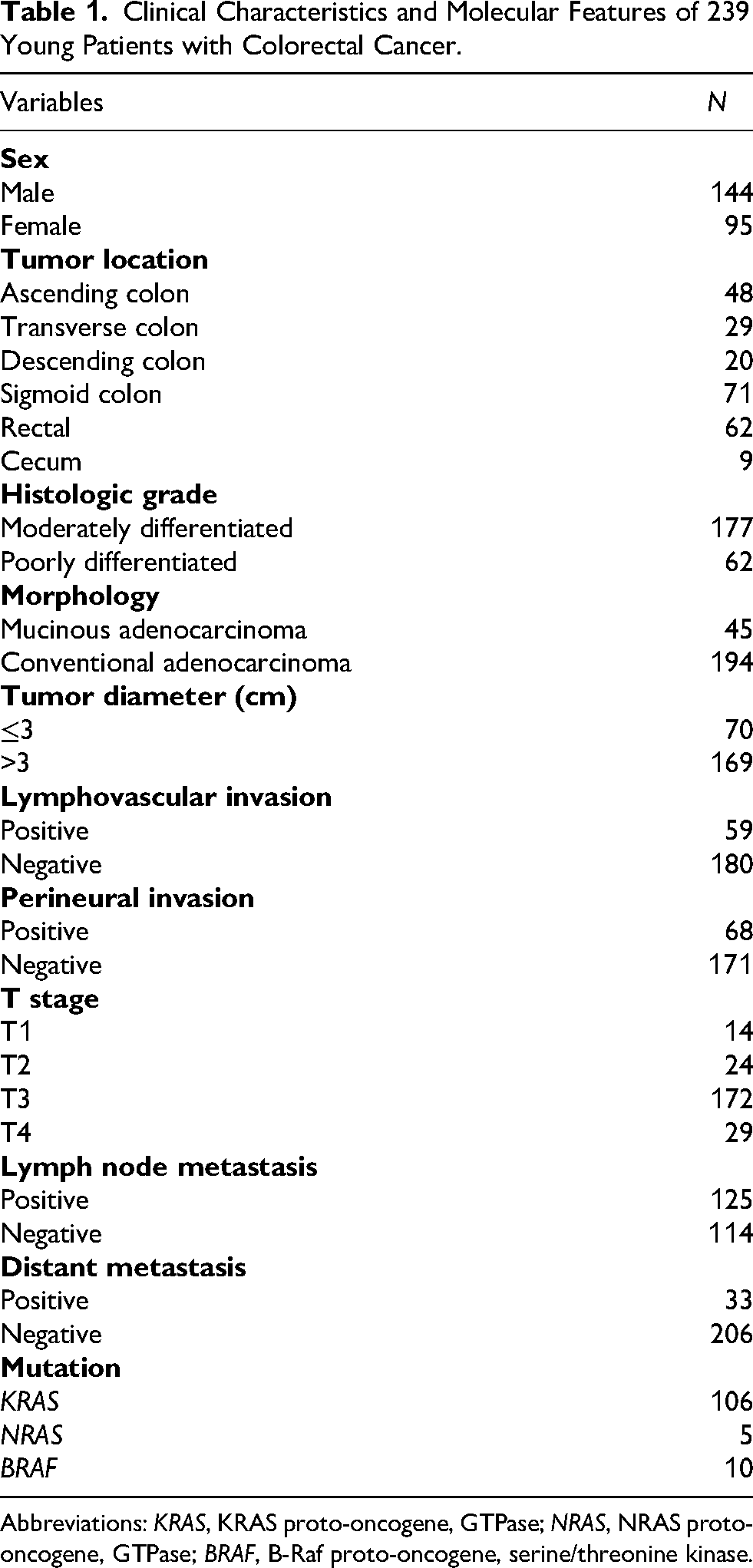
Abbreviations: KRAS, KRAS proto-oncogene, GTPase; NRAS, NRAS proto-oncogene, GTPase; BRAF, B-Raf proto-oncogene, serine/threonine kinase.
Histopathological examination revealed that 194 tumors (81.2%) were conventional adenocarcinoma, and 45 tumors (18.8%) were mucinous adenocarcinoma (Figure 1A). Of these, 177 tumors (74.1%) were of moderate histological grade, and 62 tumors (25.9%) exhibited high histological grade. Most tumors (169 patients, 70.7%) exceeded 3 cm in diameter. Based on the tumor, node, metastasis (TNM) staging system, there were 14 T1 (5.9%), 24 T2 (10%), 172 T3 (72.0%), and 29 T4 tumors (12.1%). Lymph node metastasis (N stage, Figure 1B) was observed in 125 patients (52.3%), and distant metastasis (M stage) was observed in 33 patients (13.8%).
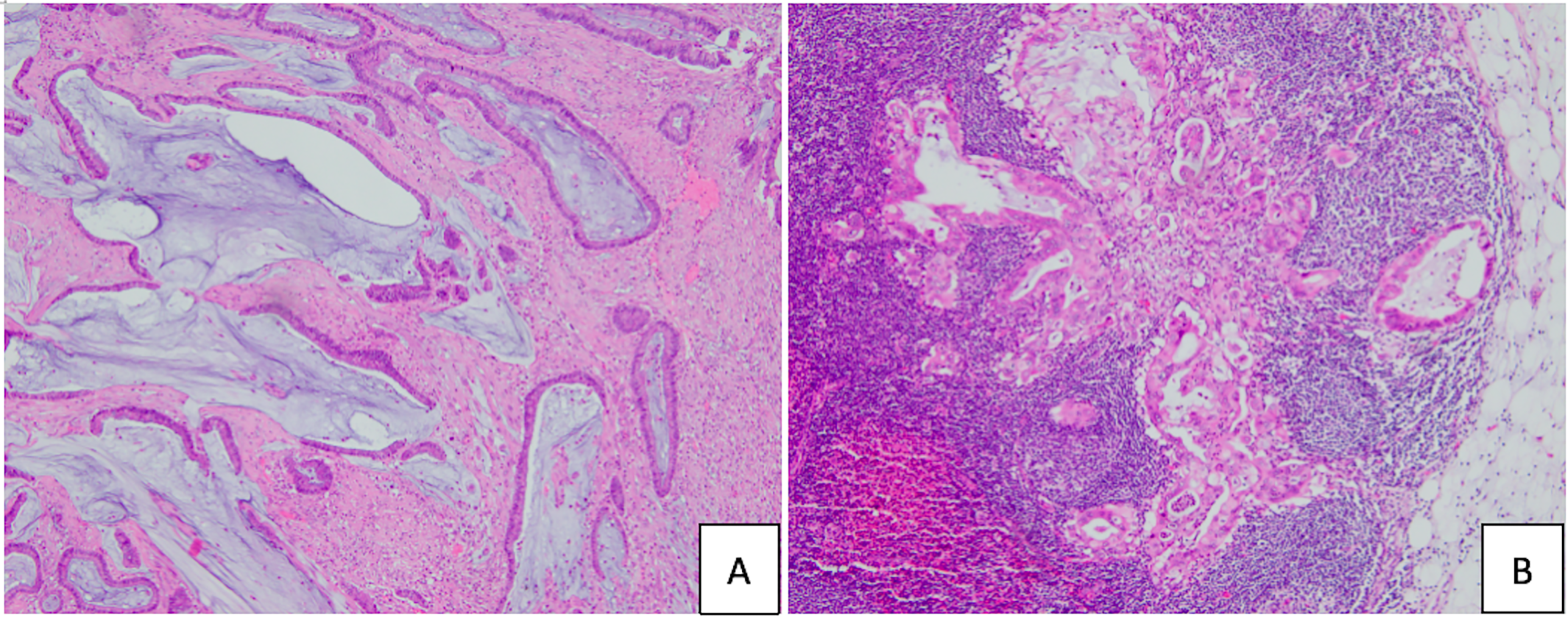
Microscopic features of not-otherwise-specified and mucinous adenocarcinomas. (A) Mucinous adenocarcinoma [hematoxylin and eosin (H&E), 100×]. (B) Lymph node metastasis (H&E, 100×).
Mutational status of KRAS, NRAS, and BRAF
To determine the molecular features of the RAS/RAF signaling pathway in early-onset CRC, mutational analysis targeting the KRAS, NRAS, and BRAF genes was conducted. The results demonstrated that 50.6% (121/239) of the cohort carried mutations in at least one of the genes in the RAS/RAF signaling pathway (Table 2). The individual mutation rates for KRAS, NRAS, and BRAF were 44.4% (106/239), 2.1% (5/239), and 4.2% (10/239), respectively. Notably, no patients with concurrent mutations in two or more genes were observed. 24
Comparison of Clinicopathological Features Based on the dMMR and Genetic Mutation Status.
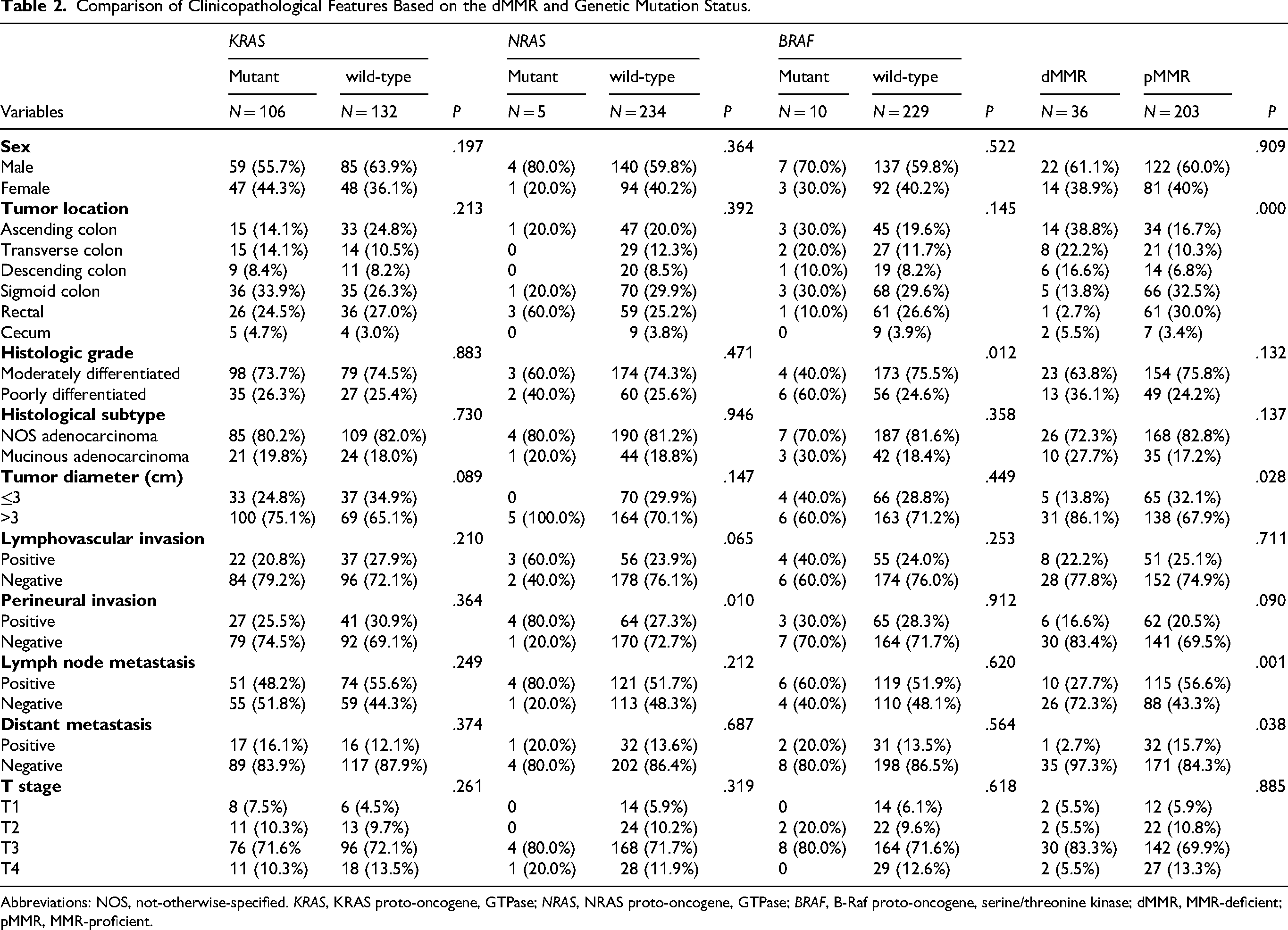
Abbreviations: NOS, not-otherwise-specified. KRAS, KRAS proto-oncogene, GTPase; NRAS, NRAS proto-oncogene, GTPase; BRAF, B-Raf proto-oncogene, serine/threonine kinase; dMMR, MMR-deficient; pMMR, MMR-proficient.
Associations Between KRAS/NRAS/BRAF Mutations and Clinicopathologic Features
To evaluate the clinical relevance of specific KRAS/NRAS/BRAF mutations, we investigated the associations between gene mutations and clinicopathologic features (Table 2). KRAS mutations had no statistically significant associations with sex, tumor size, histological grade, or TNM stage (P > .05). Despite the small number of NRAS-mutated tumors, a significant association was observed with perineural invasion (P = .01, Table 2). Perineural invasion was present in four of five NRAS-mutated patients, versus 64 of 234 NRAS wild-type patients. Additionally, the BRAF V600E mutation was significantly associated with high tumor grade (P = .012, Table 2). By contrast, no significant differences in KRAS and NRAS mutation rates were found among patients with varying tumor grades (P > .05). Furthermore, no significant differences in gene mutation rates were identified according to the primary tumor location (P > .05).
MMR Status and Correlations with Clinicopathologic Features
Based on the potential importance of dMMR in early-onset CRC, especially its connection with Lynch syndrome, 25 we evaluated MMR protein expression by immunohistochemistry. We assessed the expression of MLH1, MSH2, MSH6, and PMS2 in all collected tissue samples. The absence of expression of any tested MMR proteins was classified as dMMR (Figure 2), whereas patients carrying all four intact proteins were classified as MMR-proficient (pMMR). Among the 239 patients, the dMMR detection rate was 15.1% (36/239). Additionally, KRAS mutations were more frequent in the dMMR cohort (63.8%, 23/36) than in the pMMR cohort (40.8%, 83/203; P < .05).

The expression of the mismatch repair proteins mutL homolog 1 (MLH1), postmeiotic segregation increased 2 (PMS2), mutS homolog 6 (MSH6), and mutL homolog 2 (MSH2) in CRC (×200). (A) Adenocarcinoma with the loss of PMS2 expression. (B) Adenocarcinoma with the loss of MSH2 and MSH6 expression. (C) Adenocarcinoma with the loss of MLH1 and PMS2 expression. CRC, colorectal cancer.
Univariate analysis demonstrated that the dMMR status was significantly associated with a larger primary tumor diameter (P = .028), the tumor location (P < .001), the absence of lymph node metastasis (N0: 72.3% vs 43.4%; P = .001), and a lack of distant metastasis (M0: 97.3% vs 84.3%; P = .038). dMMR tumors exhibited a preference for proximal colon locations, with few patients harboring dMMR having tumors in distal locations compared with the findings in the pMMR population.
Discussion
Although CRC is traditionally considered a disease affecting middle-aged and older adults, recent epidemiologic data indicate a significant rise in both the incidence and mortality of CRC in patients younger than 45 years. 26 Patients with early-onset CRC display distinct molecular and clinical features and a more advanced stage at diagnosis. 27 These findings highlight the need for a deeper understanding of the pathogenesis of early-onset CRC.
In CRC, the most extensively studied oncogenes belong to the RAS family, among which the KRAS gene is the most frequently mutated. Our study identified a KRAS mutation rate of 44.4% (106/239), consistent with previous studies reporting a KRAS mutation rate between 30% and 50% in patients with CRC.28–30 Previous research indicated that KRAS mutations are more prevalent in women, patients with right-sided colon cancers, and patients with poorly differentiated tumors, and these mutations are also associated with patient age.31–33 However, our study did not find significant correlations between KRAS mutations and these clinicopathologic characteristics. The age-specific composition of our cohort may partly account for these discrepancies, as the biological behavior of KRAS-mutated tumors could differ between young and older patients. These findings suggest that KRAS-clinicopathologic associations are consistent across all CRC populations, emphasizing the potential value of age-specific molecular analysis in the future.
NRAS, another important member of the RAS gene family, has a relatively low mutation rate in CRC. Previous studies reported a mutation rate of 2.2%-7% in CRC,34,35 with a higher likelihood of occurrence in older patients. 36 In our study, the overall mutation rate of NRAS was 2.1% (5/239), aligning with these earlier findings. We observed that NRAS mutations were more common in patients with perineural invasion, a finding not previously reported in the literature to our knowledge. However, given the small number of NRAS-mutated patients (n = 5), this association should be interpreted with caution and requires validation in larger cohorts. No significant associations were found between NRAS mutations and other clinicopathological characteristics, consistent with previous studies.
Emerging evidence has revealed that the BRAF mutation rate in CRC ranges from 1.8% to 20%,37,38 in line with the BRAF mutation rate of 4.2% (10/239) in this study. Of note, accumulating evidence has linked the BRAF V600E mutation to various clinicopathologic features in patients with CRC (female sex, advanced age, high grade, mucinous histology, and proximal colon tumor location).39,40 In the current study, high histological grade was significantly associated with BRAF V600E mutation, which is consistent with previous studies that link BRAF V600E to poorly differentiated tumors in CRC.39,40 This association was observed across all age groups, indicating that the effect on tumor progression of this mutation may be independent of age. However, because of the small number of BRAF-mutated patients in this study, these findings should be confirmed in larger cohorts in the future.
MMR dysfunction represents an important pathway in CRC pathogenesis. Moreover, MMR status serves as a clinically important biomarker for predicting immunotherapy response, identifying hereditary cancer syndromes such as Lynch syndrome, and guiding prognosis prediction and treatment decisions in CRC.41,42 Our analysis revealed an association of the anatomical distribution with the MMR status. dMMR CRC displayed a significant preference for the proximal side of the colon (61.1%, 22/36). Conversely, few patients (2.8%, 1/36) harboring dMMR developed tumors in distal locations, contrasting the substantially higher proportion of patients who developed rectal tumors in the pMMR cohort (30%, 61/203). These findings suggest that dMMR can participate in the development of right-sided colon cancer, and the genetic mechanisms underlying left- and right-sided colon cancers might differ. Furthermore, the dMMR population also exhibited distinct metastatic features. We observed that 72.3% of dMMR tumors lacked lymph node metastasis, and these patients had a significantly lower rate of distant metastasis compared to the pMMR population. These observations might partially explain why a favorable prognosis is associated with the dMMR phenotype. Our findings both reinforce established associations and provide novel insights into the anatomical and metastatic behavior of dMMR tumors.
Interplay Between KRAS and MMR Status
In our study, we identified a KRAS mutation frequency of 63.8% among patients with dMMR, which significantly exceeded the rate in the pMMR cohort (40.8%). However, this pattern is inconsistent with previously reported data, which suggested a lower KRAS mutation rate in MSI-H tumors than in microsatellite-stable tumors. 43
Conventionally, MSI-H tumors are thought to arise through a distinct pathway driven by defective DNA MMR, which has been considered largely mutually exclusive with KRAS-driven carcinogenesis.
Several factors may account for this discrepancy. First, the age distribution of our cohort may play a role. Most previous studies examining KRAS and MSI associations were conducted in predominantly older populations, whereas our study focused exclusively on young patients (≤45 years). Early-onset CRC has been shown to exhibit distinct molecular features, and the relationship between KRAS mutation and MMR status may differ in this age group. Second, the composition of dMMR patients may differ between populations. While many prior studies did not distinguish between sporadic and hereditary dMMR/MSI-H tumors, our cohort may include a higher proportion of Lynch syndrome-associated patients, which have been reported to harbor higher KRAS mutation rates. Indeed, a recent study found a KRAS mutation rate of 65% in Lynch-associated dMMR/MSI-H tumors, aligning with our observation. 44
Limitations and Future Directions
Several limitations of this study should be acknowledged. First, due to the retrospective design and lack of follow-up data, survival analysis could not be performed. Consequently, the prognostic significance of the molecular markers examined remains unknown, and our findings are limited to associations with clinicopathological features rather than patient outcomes. Second, this study did not include an older control group for comparison; therefore, whether the observed features are specific to young patients or generalizable across age groups remains unclear. Third, the sample size was relatively small, particularly for subgroup analyses such as NRAS mutations (n = 5), which limited statistical power. Fourth, this was a single-center study, which may limit the generalizability of our findings. Fifth, MMR status was assessed solely by immunohistochemistry without confirmatory MSI testing, and discordance between these methods may have led to misclassification in a subset of patients. Sixth, we did not stratify the dMMR cohort by hereditary versus sporadic origin, which limits our ability to determine whether the observed high KRAS mutation rate in dMMR tumors is specific to hereditary or sporadic early-onset CRC. Future prospective multicenter studies with larger cohorts, age-matched control groups, molecular MSI testing, long-term follow-up, and a detailed classification of dMMR patients by hereditary status are needed to validate our findings and evaluate the prognostic significance of these molecular markers in patients with early-onset CRC.
Conclusion
In this investigation, we characterized the frequencies of KRAS, NRAS, and BRAF mutations and MMR protein expression patterns in 239 patients of early-onset CRC in China. We also interrogated the association between the RAS/RAF mutation landscape and MMR status. The connection between molecular alterations in RAS/RAF, MMR, and clinicopathologic features enhances our understanding of CRC biology in young patients and provides valuable guidance for personalized genetic testing and targeted therapies in the future.
Footnotes
Abbreviation
Acknowledgments
Not applicable.
Ethical Approval
This study was approved by the Ethics Committee of Guangdong General Hospital (S2025-296-01).
Informed Consent Statement
Written informed consent was obtained from all participants.
Author Contributions
LC contributed to conceptualization, investigation, methodology, writing original draft, and writing—review and editing. WY contributed to project administration, supervision, data curation, review editing, and funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Guandong Medical Research Fund (grant number A2022067).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.