
Abstract
Introduction
Cannibalism is a common ecological interaction within the animal kingdom. It occurs not only due to extreme food scarcity or artificial conditions, but also naturally in various higher species. 1 Cannibalism also occurs at the cellular level in humans. In cytological and histological preparations, it appears as “a cell inside a larger cell with a crescent-shaped nucleus.” This appearance results from the engulfed cell being contained within a large vacuole, which pushes the cannibalized cell's nucleus to the cell's periphery.1,2 This phenomenon, first described in the last century, has been referred to by various names, including “bird's eye cells” and “signet ring cells,” on the basis of their morphological appearance under a microscope.3-5 The process by which one cell internalizes another is defined as “cell-in-cell formation.” Cell-in-cell (CIC) formation involves the internalization of living hematopoietic cells by nonphagocytic cells (emperipolesis), homotypic, and heterotypic phagocytosis-like uptake of living or dead cells, and the invasion of a tumor cell into the host cell (entosis). Thus, the ingestion of both living and dead tumor cells is referred to as cellular cannibalism (CC). There are some differences in CIC interactions, formation mechanisms, intercellular relationships, and intracellular fates. 6 Entosis and emperipolesis differ from cannibalism in that the cell invades the host cell rather than actively engulfing it. Emperipolesis differs from entosis in that it occurs between heterotopic cells, whereas entosis occurs between homotypic cells. Furthermore, emperipolesis allows the internalized cell to kill the host cell. Cannibalism can occur between the same cell types (homogeneous cannibalism) or between different cell types (heterogeneous cannibalism). 7
CC, as defined by Brouwer et al, 8 is a sequential process. The cannibalistic process begins with the attachment of the guest cell to the host cell, followed by its gradual internalization into the host cell's cytoplasm. As a result, the nucleus of the host cell is displaced to the periphery, acquiring a crescent-like shape, while the nucleus of the internalized (guest) cell remains morphologically intact within a large vacuole. Finally, the engulfed cell may die, divide within vacuoles, or escape the host cell and survive.
During carcinogenesis, most cancer cell metabolic pathways appear to transition from Pasteur-like metabolism to Warburg-like metabolism, resulting in an acidic microenvironment and, eventually, a positive feedback loop for carcinogenesis. In response to this acidic state, the tumor environment promotes the development of some pathogenic cells capable of surviving under such harsh conditions. 9 Through metabolic pathway transformation, malignant cells with a virulent phenotype survive by destroying other cells in the environment. This phenomenon is believed to be associated with the epithelial-mesenchymal transition (EMT) phenotype that cancer cells that engulf acquire.10,11 The tumor microenvironment facilitates this process. As a result, negative conditions such as hypoxia, nutritional deficits, and acidic environments promote CC. CC is hypothesized to help malignant tumors survive in extreme microenvironmental conditions such as hypoxia, nutritional deficiency, and acidity.2,9
Various CIC interactions are thought to be related to the aggressiveness, degree of anaplasia, invasiveness, and metastatic potential of the malignancy.12,13 CIC interactions have previously been described in tumors such as malignant melanoma, 14 endometrial stromal sarcoma, 15 breast carcinoma, 16 lung giant cell carcinoma, 17 pancreatic ductal adenocarcinoma (PDAC),18,19 and oral squamous cell carcinoma (OSCC).12,13,20-22 The CIC phenomenon is hypothesized to benefit tumors through cell competition while also contributing to tumor growth. 1 However, it has been suggested that CIC interactions could be used to inhibit tumor growth by eliminating malignant cells. 6 Various mechanisms have been postulated. Some of these include the hypothesis that, in the absence of nutrition, internalized cells serve as a nutrient source for the engulfing cell, while the engulfed cell is digested and killed, thereby eliminating cells with low malignant potential.1,7 Another idea is that tumor cells may directly and effectively neutralize the antitumor immune response by engulfing tumor-infiltrating lymphocytes (TLIs) and erythrocytes.11,23
Aneuploidy is an additional mechanism believed to facilitate tumor progression. Aneuploidy arises from horizontal or lateral DNA transfer from an engulfed cell subsequent to mitotic disruption. Enhanced chromosomal instability is believed to increase the malignant potential of tumors.24,25 The mechanism of CIC formation is believed to involve internalization through transmembrane 9 superfamily member 4 (TM9SF4), subsequently leading to degradation by lytic enzymes, including cathepsin B, caveolin, and the actin-binding protein ezrin, which are activated under acidic conditions.1,2,24 In molecular pathogenesis, MYC, KRAS G12 V, mutant TP53 expression, and CDKN2A loss are associated with CIC formation.26,27 Each of the molecular factors and mechanisms that are believed to be involved in CIC interactions may serve as novel potential targets for future antitumor therapies.
There are few studies in the literature examining the relationship between CIC interactions and prognosis in patients with colorectal carcinoma.7,28,29 Our study explores the utility of using CC in routine reporting as a potential additional parameter for determining the prognosis of patients with colorectal carcinoma. We also aim to identify potential clinical and histopathological parameters and possible molecular relationships that may be associated with CC.
Materials and Methods
Patient Selection and Data Collection
Our study was approved by the institution's ethics committee. All 232 patients diagnosed with colorectal adenocarcinoma who had resection materials examined in our department over a 7-year period and who had clinical follow-up data and hematoxylin-eosin (H&E) stained preparations were included in the study. Patient demographic data, including age and sex, and clinical data, including mortality, recurrence/metastasis status, and preoperative and postoperative treatment history, were obtained from the hospital information and registry system. Histopathological features, including tumor differentiation, lymphovascular and perineural invasion, budding status, presence of TLIs, tumor margins (infiltrative or pushing), and pTNM stage, were retrospectively collected and recorded from pathology reports.
Microsatellite instability (MSI) status was determined via polymerase chain reaction in patients classified as MSI-high or MSI-low on the basis of the results of routine mismatch repair (MMR) deficiency immunohistochemistry. Pyrosequencing was used to determine the KRAS mutation status of patients with metastatic disease. The results of patients who underwent MSI and KRAS analysis were retrospectively retrieved from pathology reports and recorded.
Histologic Definition and Quantification of Cell-in-Cell Structures in Tissue Specimens
All histopathological evaluations, including the identification and quantification of CC, were performed by a single experienced pathologist to ensure standardization and eliminate inter-observer variability. During the evaluation, the pathologist was unaware of the patients’ clinical outcomes and molecular characteristics. To verify the reliability of the scoring, intra-observer reproducibility was confirmed by re-examining 10% (n = 23) of the slides after a 4-week interval, which ensured a high level of consistency.
CC assessment was performed on a single representative H&E stained section for each patient. Slides were carefully selected from the archive, specifically targeting areas with high tumor density and no necrosis to provide optimal visualization and eliminate potential counting errors. Counting was primarily performed by scanning the entire tumor area at low magnification to identify regions with the highest cannibalistic activity. Following this initial assessment, quantification focused on these “hot spot” areas, predominantly located at the invasive edge of the tumor. To ensure diagnostic certainty, only structures meeting the classic morphological criteria for CC (a cell within a larger cell with a crescent-shaped nucleus) were included in the final count (Figure 1). Tumor necrosis or degenerative cell areas that were difficult to assess were excluded from the analysis. Furthermore, internalized or engulfed cells exhibiting typical mitotic figures or apoptotic features (such as pyknotic nuclei, nuclear fragmentation, and loss of nuclear detail) were not included in the assessment. As described in previous studies, sections were graded according to the number of cannibalistic cells found in 10 high-power fields of the tumor area using a 40x objective lens (0.65 mm2): Grade 1 (≤5 cells), Grade 2 (6-15 cells), and Grade 3 (≥16 cells).21,22

Cellular cannibalism is shown. (a) It is marked within a circle (H&E, x20 magnification), (b, c) CC is indicated by arrows (H&E, x40 magnification). CC, cellular cannibalism. H&E, hematoxylin-eosin.
Statistical Analysis
Statistical analyses were performed using the SPSS 29.0 statistical package (SPSS, Chicago). The chi-square test and Fisher's exact test were used to compare categorical data. The independent samples t-test was used to compare normally distributed continuous variables, while the Mann-Whitney U test was used for non-normally distributed variables. Overall survival was calculated by measuring the time between the biopsy date and the date of death. The Kaplan-Meier estimator was used to calculate overall survival rates, and the log-rank test was used to evaluate differences between survival curves. To examine the relationships between overall survival and prognostic parameters, all parameters were first evaluated using univariate analyses. Multivariate analysis models were created using parameters with prognostic significance in the univariate analysis and the CC variables, which were the main parameters we tested. Logistic and Cox regression analyses were performed to examine the relationships between survival, survival duration, and potential predictors. A P-value < .05 was considered significant; however, the significance threshold was adjusted to P ≤ .0045 after Bonferroni correction for multiple clinicopathological comparisons.
Results
Demographic and Histopathological Characteristics
Among the patients included in the study, 80 (33%) were female, and 152 (67%) were male. The mean age was 64.36 ± 12.9 years (range: 23-90). The tumor locations were as follows: colon in 134 patients (57%) and rectum in 92 patients (43%). Among the tumors analyzed, 101 (87%) were classified as well-to-moderately differentiated, whereas 27 (13%) were poorly differentiated. Lymphovascular invasion was observed in 87 (36%) of the patients, with perineural invasion noted in 42 (18%) patients. Tumor budding was present in 125 (54%) patients. MSI was evaluated in 184 patients. It was detected in 15 patients (5%). CC occurred in 196 (84%) patients, whereas 37 (16%) did not exhibit this phenomenon. The degree of cannibalism was graded as follows: grade 1 in 11 (6%) patients, grade 2 in 147 (75%) patients, and grade 3 in 38 (19%) patients. Among the patients, 128 (55%) had metastatic disease, whereas 104 (45%) had nonmetastatic disease. The distribution of patients according to pT stage was as follows: T1 in 22 patients (12%), T2 in 62 patients (33%), T3 in 64 patients (34%), and T4 in 39 patients (21%). Additionally, 131 (56%) of the patients received treatment, whereas 23 (10%) did not.
Follow-Up
The median overall survival for all patients was 72 ± 3 months. The cumulative survival rates at 1, 3, and 5 years after resection were 90%, 68%, and 54%, respectively. The median follow-up duration was 48.6 months. The median overall survival time was significantly longer in the nonmetastatic group (107.2 ± 3 months) than in the metastatic group (48.8 ± 3.5 months) (log rank; P < .001).
Relationship Between Survival and Histopathological Features and Cellular Cannibalism
To create more homogeneous prognostic groups, all survival analyses were performed separately for the nonmetastatic, metastatic, and overall study groups.
Overall Study Group
CC was noted in 6 of 22 patients at the T1 stage, 42 of 62 patients at the T2 stage, and all 103 patients at the T3 and T4 stages. The association between advanced T stage and CC was statistically significant (P < .001). The association between advanced N stage and CC was also significant (P < .001). A significant association was found between lymphovascular invasion, perineural invasion, and CC (P < .001). Following the Bonferroni correction, the association between CC and tumor budding did not reach statistical significance with the adjusted alpha level of P ≤ .0045 (P = .005). No association was found between lymphocytes infiltrating the tumor, tumor margin structure, and CC (Table 1). The association between MSI status and CC was also not statistically significant. Furthermore, the parameters detailed in Table 1 were also compared with the grades of CC, and no statistically significant associations were identified.
Relationships Between Demographic and Histopathological Parameters and CC.
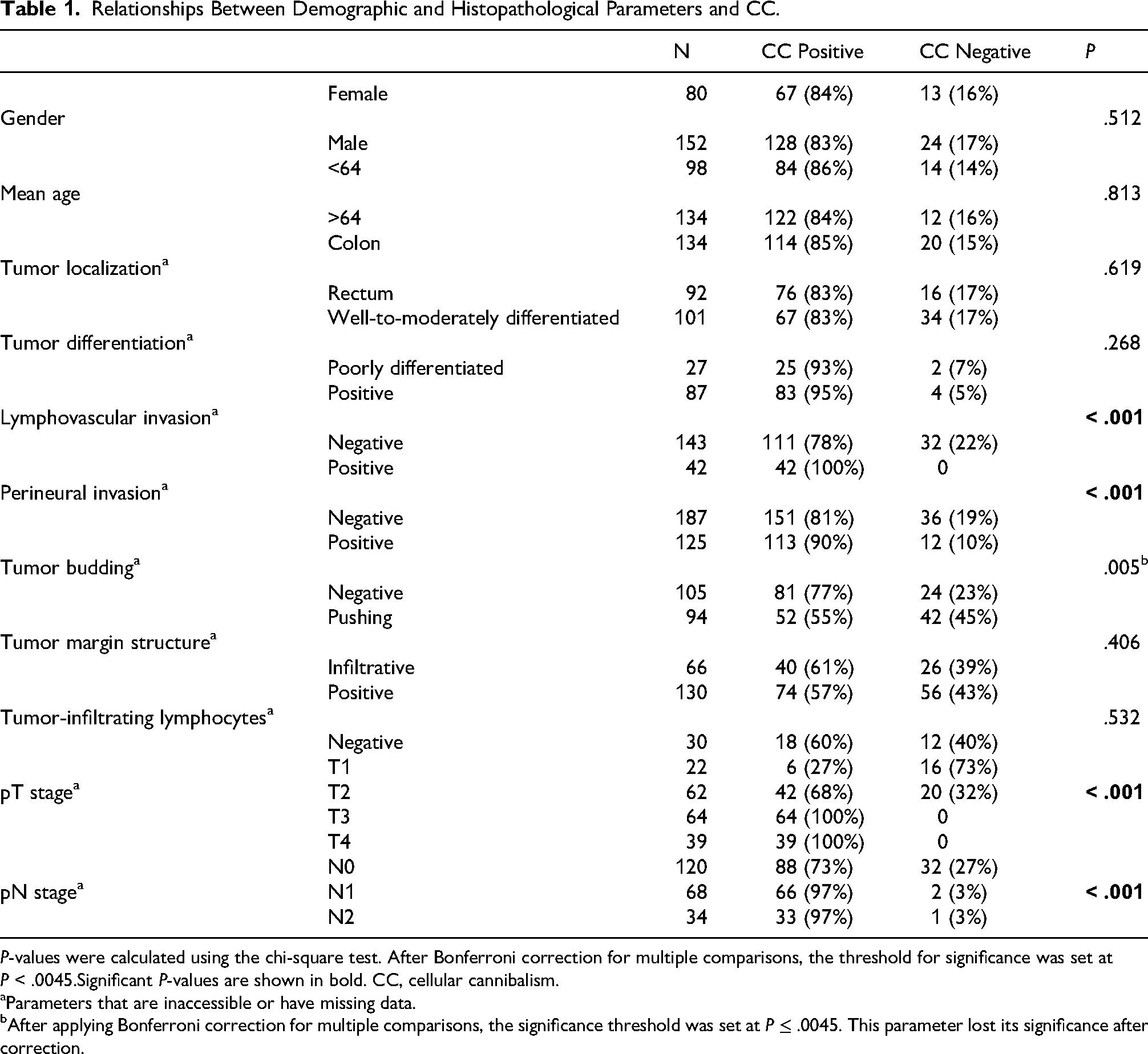
P-values were calculated using the chi-square test. After Bonferroni correction for multiple comparisons, the threshold for significance was set at P < .0045.Significant P-values are shown in bold. CC, cellular cannibalism.
Parameters that are inaccessible or have missing data.
After applying Bonferroni correction for multiple comparisons, the significance threshold was set at P ≤ .0045. This parameter lost its significance after correction.
There was a significant association between metastasis and several factors: positive surgical margins (P = .039), tumors located in the rectum (P = .007), lymphovascular invasion, perineural invasion, and the pT and pN stages (P < .001). Additionally, a significant association was found between CC, an increased number of CC, and grade 3 CC with metastasis (P < .001) (Table 2). In our multivariate logistic regression analysis, we identified advanced pN stage as an independent poor prognostic factor for tumor recurrence within a model that included tumor localization, lymphovascular invasion, perineural invasion, CC number, CC degree, and pT and pN stages (OR 4.9, 95% CI: 1.1 to 21.3, P = .033).
Comparison of CC Parameters in Metastatic and Nonmetastatic Study Groups.
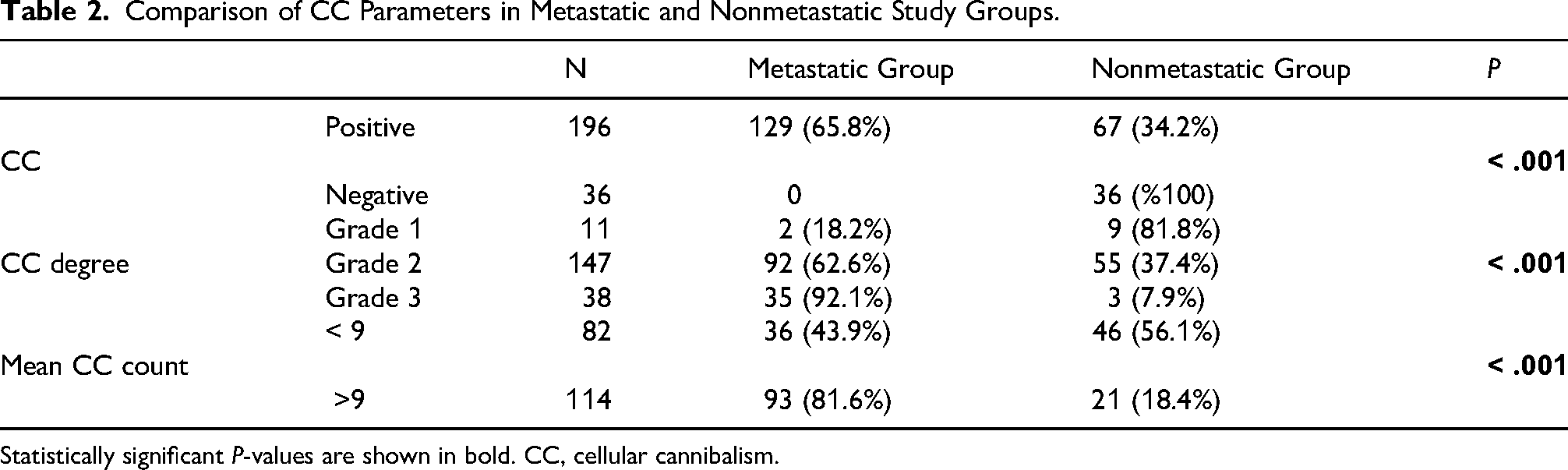
Statistically significant P-values are shown in bold. CC, cellular cannibalism.
A significant association was found between the mortality rate and several factors, including positive surgical margins (P = .012), rectal tumor localization, lymphovascular invasion, perineural invasion, pT stage, and pN stage (P < .001). In addition, a significant association was noted between the mortality rate and CC and between the mortality rate and increased CC count (P < .001). Overall survival was significantly lower in patients with positive surgical margins than in those without (27.4 vs 74 months, respectively) (log rank; P = .002), in patients with lymphovascular invasion than in those without (54 vs 82.1 months, respectively) (log rank; P < .001), in patients with perineural invasion than in those without (45.9 vs 78.1 months, respectively) (log rank; P < .001), and in patients with CC than in those without (64.6 vs 109 months, respectively) (log rank; P < .001). Additionally, overall survival was statistically significantly shorter in patients with Grade 3 CC than in those with Grade 2 CC (40.7 vs 68.8 months, respectively) (log rank; P = .01) (Figure 2). In our multivariate model, which included variables such as lymphovascular invasion, perineural invasion, pT stage, metastasis, and CC, Cox regression analysis revealed that the presence of metastasis was an independent poor prognostic factor (HR 6.2, 95% CI: 1.5 to 25, P < .001). Additionally, in our logistic regression analysis, which incorporated variables of localization, lymphovascular invasion, perineural invasion, CC, number of CC, pT stage, and metastasis status, both CC and the presence of metastasis were identified as independent poor prognostic factors (OR 10.8, 95% CI: 1 to 115.6, P = .049, OR 20.8, 95% CI: 4.2 to 102.3, P < .001, respectively) (Table 3).
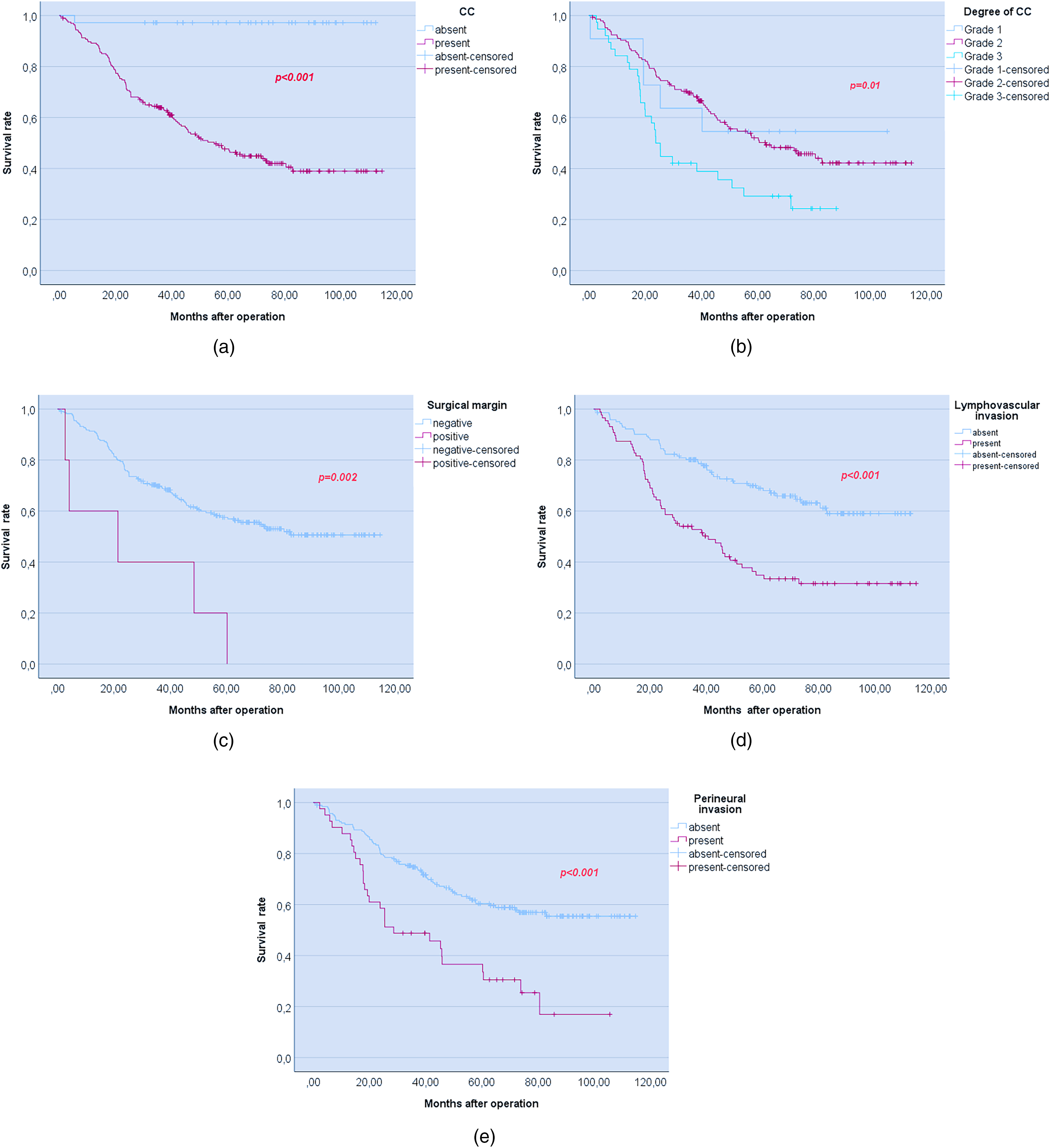
The Kaplan-Meier survival curves of the groups are presented. (a) Overall survival for CC, (b) overall survival for degree of CC, (c) overall survival for surgical margin status, (d) overall survival for lymphovascular invasion, (2) overall survival for perineural invasion. CC, cellular cannibalism.
Univariate and Multivariate Analysis of Predictors of Overall Survival for the Overall Study Group. The P-values for Univariate Analyses are Given. The P-values, Hazard and Odds Ratios, and Confidence Intervals for Multivariate Logistic and Cox Regression Analyses are Also Provided.
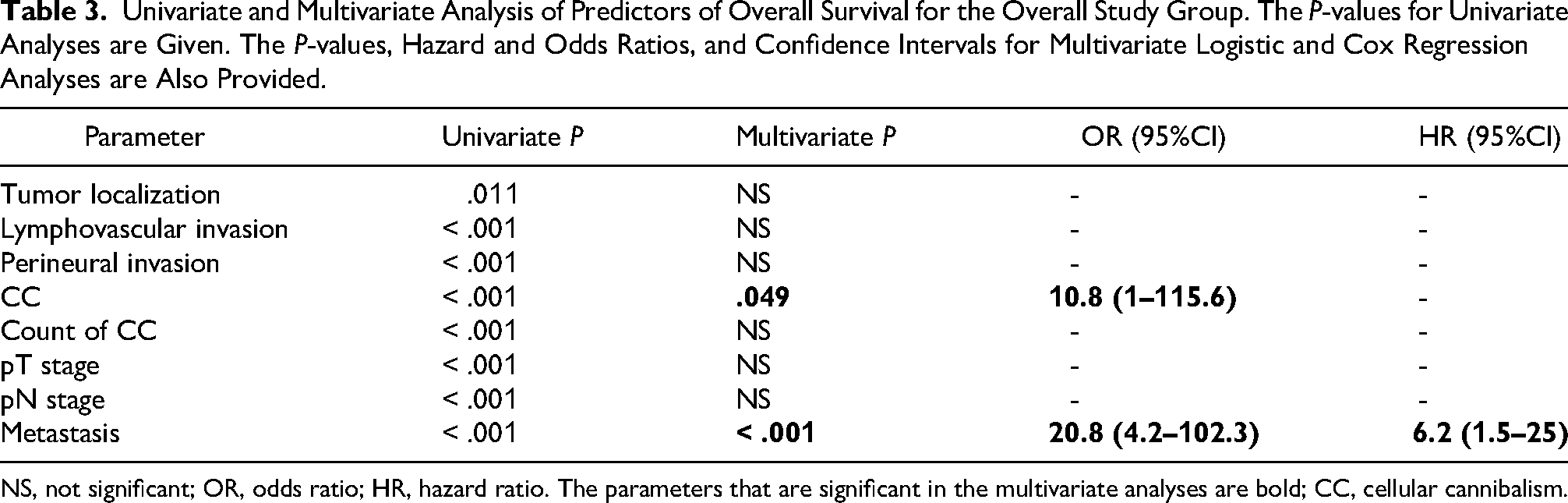
NS, not significant; OR, odds ratio; HR, hazard ratio. The parameters that are significant in the multivariate analyses are bold; CC, cellular cannibalism.
Univariate and Multivariate Analysis of Predictors of Overall Survival for the Non Metastatic Study Group. The P-values for Univariate Analysis are Given. The P-values, Hazard and Odds Ratios, and Confidence Intervals for Multivariate Logistic and Cox Regression Analyses are Also Provided.
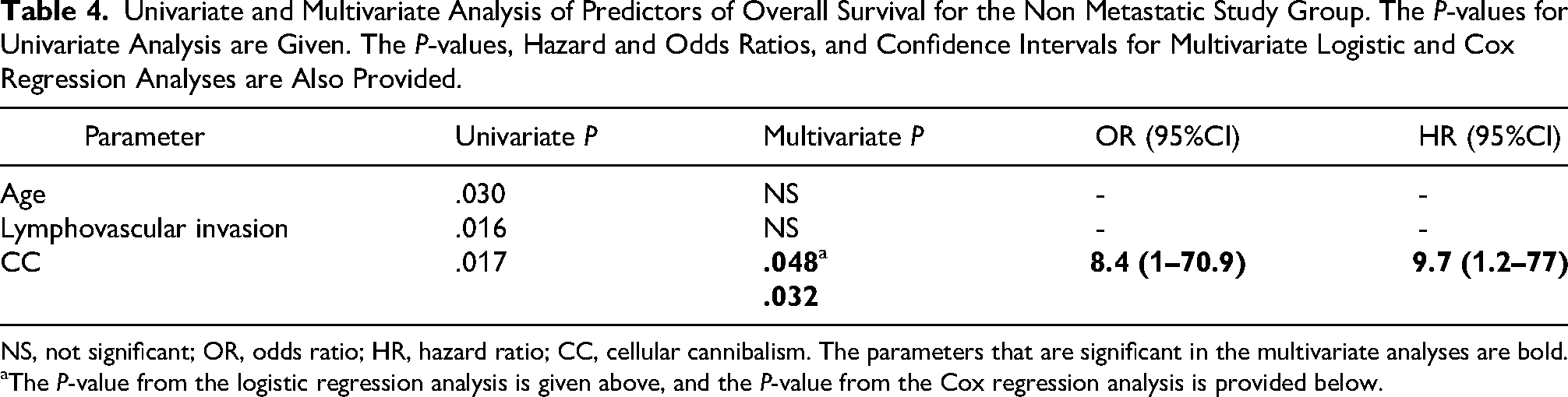
NS, not significant; OR, odds ratio; HR, hazard ratio; CC, cellular cannibalism. The parameters that are significant in the multivariate analyses are bold.
The P-value from the logistic regression analysis is given above, and the P-value from the Cox regression analysis is provided below.
There was a significant association between death and male sex (P = .034), rectal tumor location (P = .04), and the presence of lymphovascular invasion (P < .001). There was no significant association between death and the mean number or degree of CCs.
The median overall survival time in this group was 48.8 ± 3.5 months. Overall survival was markedly lower in men than in women (40.6 vs 48.7 months, respectively) (log rank; P = .043), in individuals with positive surgical margins than in those without (18 vs 48.1 months, respectively) (log rank; P < .001), in patients exhibiting lymphovascular invasion than in those without (35.4 vs 50.8 months, respectively), in T4 stage patients than in T3 stage patients (33.2 vs 46.6 months, respectively) (log rank: P = .048), and in N2 stage patients than in N0 stage patients (31.3 vs 51.2 months, respectively) (log rank; P = .044). No significant link was found between overall survival time and the average number or degree of CCs. In our multivariate model, which included variables such as sex, surgical margin status, pT and pN stages, lymphovascular invasion status, and degree of CC in Cox regression analysis, positive surgical margin and male sex were identified as independent poor prognostic factors (HR 14.9, 95% CI: 1.4 to 150.4, P = .022; HR 2.2, 95% CI: 1.1 to 4.2, P = .013, respectively). Our multivariate model, which included variables such as sex, tumor location, lymphovascular invasion status, and degree of CC in logistic regression analysis, revealed that the presence of lymphovascular invasion was an independent poor prognostic factor (OR 7.4, 95% CI: 2.5 to 22, P < .001) (Table 5).
Univariate and Multivariate Analysis of Predictors of Overall Survival for the Metastatic Study Group. The P-values for Univariate Analysis are Given. The P-values, Hazard and Odds Ratios, and Confidence Intervals for Multivariate Logistic and Cox Regression Analyses are Also Provided.
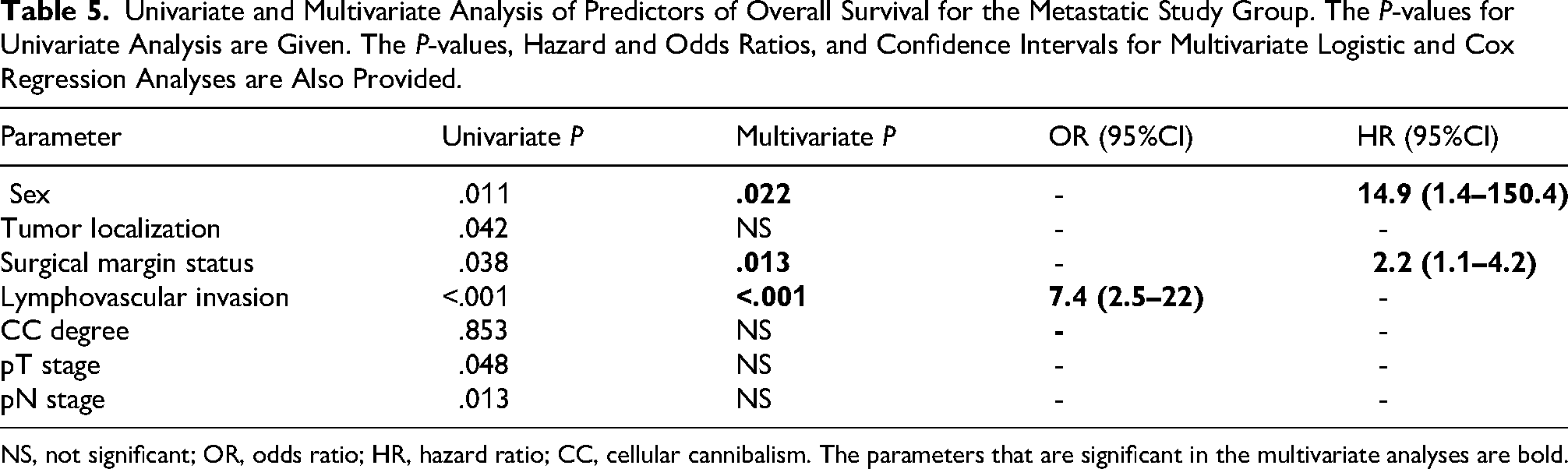
NS, not significant; OR, odds ratio; HR, hazard ratio; CC, cellular cannibalism. The parameters that are significant in the multivariate analyses are bold.
Discussion
In this study, a statistically significant association was found between the presence of CC and adverse morphological prognostic factors, such as advanced pT and pN stages, lymphovascular invasion, and perineural invasion. Overall survival was significantly shorter in patients with CC. Furthermore, in the multivariate analysis, the presence of CC was identified as an independent poor prognostic factor.
Previous studies have suggested a potential relationship between cannibalistic cell counts and aggressive and metastasizing behavior in systemic cancers. A study comparing metastatic and nonmetastatic OSCC revealed that the metastatic group had a considerably greater mean number of CC. 22 In our study, the presence of Grade 3 CC and the average number of CCs were also significantly associated with metastasis.
A study suggested grading breast carcinomas using increased CC counts. 30 Additionally, CIC interaction was found to be more prevalent in poorly differentiated tumors in a study of PDACs. 18 We found no significant associations between the average CC count and the degree of CC and tumor differentiation. However, the small number of poorly differentiated tumors in our group may have constrained our evaluation.
The findings of a study involving PDACs demonstrated that tumors with CICs presented an increased incidence of lymphovascular and perineural invasion, which aligns with our findings. 19 Another study examined the relationships between CIC structures and clinical and histopathological parameters in patients with colorectal carcinomas, with a specific focus on pTNM staging, age, sex, and lymphovascular invasion parameters; however, no significant associations were found. 28
Studies on the relationships between CIC interactions and survival in rectal tumors, head and neck squamous cell carcinomas, and PDACs have revealed that the presence and number of CICs are associated with shorter survival. Multivariate analyses in these studies revealed that the presence of CIC is an independent poor prognostic factor.19,31 In a study of colorectal carcinomas, CIC was identified as an independent poor prognostic factor for patients with stage 3 colorectal carcinoma. 28 We found that CC was linked to shorter survival in both the nonmetastatic study group and the overall study group. In addition, we determined that CC was an independent poor prognostic factor in multivariate analyses of these study groups.
Furthermore, our findings revealed a link between tumor budding and CC. This relationship has not been previously examined in the literature, and our study is the first to investigate and demonstrate it. Despite the weakening of statistical significance due to multiple comparison corrections (Bonferroni), the observed trend appeared biologically plausible. Tumor budding, by definition, consists of isolated tumor cells or small clusters of tumor cells that detach from the main tumor and migrate into the stroma. During the EMT, budding tumor cells acquire cytoskeletal changes, migratory potential, and the ability to remodel the extracellular matrix. This transition is believed to facilitate their migration through the extracellular matrix, invasion of lymphatic and vascular structures, and metastasis to regional lymph nodes and distant organs. Budding is considered a histological reflection of EMT. 32
A study on colorectal carcinomas showed that, similar to tumor budding, CIC interactions are significantly more prevalent at the invasive edge of the tumor than at its center, and this phenomenon has prognostic significance. 28 Tumor budding, by definition, consists of isolated tumor cells or small clusters of tumor cells that detach from the main tumor and migrate into the stroma. Although these phenomena have different histological appearances and definitions, the results of our study raise questions about whether CIC interactions play a role in the tumor budding process or whether these two different processes are similar in terms of their mechanisms at some points.
Previous studies have reported that tumor cells exhibit genetic alterations following homotypic or heterotypic engulfment, leading to tumor progression and antitumor resistance.24,33 A study conducted with colorectal carcinomas revealed that there was a significant relationship between the frequency of CIC interactions and the amplification of stem cell genes, which increased the potential for metastasis. 7 Recent studies support the role of CIC interactions between tumor cells and other cell types, including macrophages and mesenchymal stromal cells, in metastasis. Macrophage-tumor cell fusion has also been shown to promote metastasis in colon cancer and melanoma.10,34 It is claimed that tumor cells engulf heterotrophic cells, such as mesenchymal stromal cells, causing EMT, increasing stem cell transformation and migration, and thus allowing tumor invasion and metastatic spread. 35
These studies support the idea that there may be a possible relationship or similarity between tumor budding, a prognostic parameter in colorectal carcinomas, and the CIC interaction mechanism. The results of our study also support this idea. However, further research is needed to definitively establish this potential relationship and answer the questions that arise. Demonstrating this relationship could provide a more meaningful basis for using CIC interactions as a potential additional prognostic parameter.
Lugini et al 14 demonstrated that tumor cells can engulf immune cells developed against them. These findings suggest that metastatic tumor cells may use CC as a strategy to evade the immune system. Furthermore, a study on lung carcinomas reported that lymphocytes infiltrating the tumor were associated with CC and may be an indicator of the tumor evading the immune response. 11 The tumor periphery contains tumor cells that have infiltrated into an immune cell-rich stroma. 36 Due to the higher number of immune cells, the concentration of cytokines and death ligands is increased in this region. This event is believed to enhance cellular interactions between immune cells and tumor cells. 37 In our study, we investigated the relationship between CC and lymphocytes infiltrating the tumor. We also compared CC with MSI, a feature of colorectal carcinoma with MMR deficiency, which is known to be associated with an active tumor immune microenvironment and is an important prognostic parameter in daily practice. We did not observe a significant relationship between CC and the presence of TILs or the MSI status.
KRAS mutation status has become an important parameter for guiding treatment decisions in patients with metastatic colorectal carcinoma. Previous studies have revealed a significant association between KRAS mutation and CIC interactions.18,36 In our study, CC was observed in all patients in the metastatic patient group with available molecular analysis results, so the evaluation was based on the mean CC count, and no significant association was found between CC and the KRAS mutation status. However, since the molecular analysis was not performed on all patients and our evaluation was based solely on the mean CC count, it is limited and is considered insufficient for assessing the relationship between KRAS mutation and CC.
As a result, different CIC interactions (entosis, homotypic, or heterotypic CC) have been identified in various malignancies. Some studies correlate the existence of CIC structures with a favorable prognosis, 37 whereas others associate them with an unfavorable prognosis and rapid disease progression.19,31 The variability in study results is attributed to the distinct processes of CIC interactions and the unique characteristics of tissue and cell types across different tumor types. The heterogeneous results are confusing, but these cellular interactions appear noteworthy. A clearer definition of CIC interactions is needed, along with a more profound understanding of their pathogenesis and molecular properties. The data suggest that CC may be a potential predictive marker or, by better understanding its formation mechanisms, a focus for targeted therapies that could alter the course of the disease. 14 It is also thought that CC could be inhibited by inhibiting ezrin phosphorylation or synthesis or by inhibiting tumor acidification via proton pump inhibitors. 1
The limitations of our study include a small sample size and its retrospective design, which resulted in missing data that could not be accessed for analysis. Furthermore, there is a challenge in definitively distinguishing between other intracellular interactions, such as emperipolesis and entosis, based solely on morphological assessment. However, to avoid confusion and ensure diagnostic certainty, only structures meeting the classic morphological criteria for CC (a cell inside a larger cell with a crescent-shaped nucleus) were included in the final count. This morphological definition of CC encompasses both homotypic (tumor-tumor) and heterotypic (tumor-inflammatory or stromal cell) CC. It is not possible to distinguish between these two conditions solely morphologically. Although the initial hypothesis of our study focused on tumor-tumor cannibalism, we evaluated both because we could not make this distinction at the morphological level. This issue is another limitation of our study. However, both appear to contribute to tumor progression through the mechanisms discussed in detail above. In this case, it might be considered that making a true distinction between homotypic and heterotypic CC may not be important.
Conclusion
CC can be determined by morphological features under a light microscope without the use of advanced and expensive molecular techniques. In our study, we found that CC is associated with a poor prognosis in patients with colorectal carcinomas. CC alone appears to have limited predictive value compared to traditional prognostic factors such as tumor grade, stage, and lymph node invasion. However, we believe that combining it with other predictive parameters can enhance the prognosis prediction for patients. We consider our study results valuable, as they evaluated the relationships between CC and numerous other histopathological parameters in patients with colorectal carcinomas. We believe that further studies with larger sample sizes and longer follow-up periods, as well as testing for inter-observer agreement, are needed to confirm the reliability of CC as an important and valid prognostic marker in patients with colorectal carcinoma. However, CC has been recognized as an important morphological parameter in various tumor types. It is considered to have a strong correlation with anaplasia, tumor aggressiveness, and metastatic potential. Consequently, we assert that the identification and quantitative assessment of cannibal cells during routine histopathological evaluations are crucial for validating their role as a morphological predictor.
Footnotes
ORCID iDs
Ethical Approval
This study was conducted in accordance with the principles of the Declaration of Helsinki and good clinical practice guidelines and was approved by the Dokuz Eylül University Non-Interventional Research Institutional Ethics Review Board (decision number and date: 7708-GOA-2023/01-16, 04.01.2023). Due to the retrospective nature of our study, it was not possible to obtain informed consent from the participants. Our institute's ethics committee adopts the approach that informed consent is not required for non-invasive research conducted entirely with archived materials, without additional patient testing, and with anonymized patient information. We conducted the study in accordance with ethics committee requirements.
Consent for Publication
“Not applicable.” This manuscript does not contain any individual personal data in any form (including individual details or images).
Author Contributions
All authors participated in the study design, data interpretation, data analysis, and review of the manuscript. SC, AA, and SS designed the study and wrote the manuscript. SC, AA, OS, and SS contributed to drafting, review, and editing. AA and SS contributed to validation and review. IG, ITU, HE, FB, and SS contributed to clinical management and review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.