
Abstract
Background
The 2022 World Health Organization (WHO) fifth Edition introduced major revisions to renal neoplasm classification, incorporating novel and molecularly defined entities. However, the extent to which these advances are adopted in routine pathology practice remains unclear. This international survey evaluated the global diagnostic work-up of kidney tumors, including access to ancillary tests (immunohistochemistry [IHC], fluorescence in situ hybridization [FISH], next-generation sequencing [NGS]) and familiarity with the current classification.
Methods
A 30-question online survey was distributed via SurveyMonkey to pathologists involved in renal tumor diagnostics between January and July 2024. The survey assessed demographics, practice setting, training background, WHO classification familiarity, and availability of IHC and molecular testing. Responses were analyzed using descriptive and inferential statistics.
Results
Of 427 respondents, 399 (94.8%) reported encountering kidney tumors and were included, representing 45 countries. The most represented were the United States (18.8%), Egypt (15.8%), Turkey (12.6%), the United Kingdom (8.8%), and India (7.3%). Nearly half (49.4%) had >10 years of practice, 41.1% lacked formal genitourinary pathology training, and 70.7% worked in academic settings. IHC was widely available (96.0%), whereas access to FISH (50.1%) and NGS (43.8%) was limited. High-resource academic centers had significantly greater access to molecular diagnostics than community settings (all p < .001). Kidney-specific molecular panels were available in only 18.1% of institutions. Emerging biomarkers (SDHB, FH, cathepsin K, TFE3, TRIM63) were substantially less available than conventional markers. Although 66.3% reported familiarity with the WHO classification, 33.6% cited barriers such as rapid updates, financial constraints, and workload.
Conclusions
Marked global disparities persist in renal tumor diagnostics. While IHC is widely accessible, advanced molecular tools and novel biomarkers remain unevenly distributed, underscoring the need for targeted educational and resource-sharing strategies.
Introduction
Renal cell carcinoma (RCC) represents approximately 2% of all adult malignancies, with clear cell RCC comprising the most prevalent subtype.1,2 The diagnostic classification of renal neoplasms has undergone rapid and substantial revision over the past 2 decades, driven by advances in molecular pathology. The WHO Fifth Edition Classification of Urinary and Male Genital Tumours has formally recognized numerous novel entities, including molecularly defined tumors, among others. 2 Several of these diagnoses require ancillary tests and/or molecular confirmation, including fluorescence in situ hybridization (FISH) assays and next-generation sequencing (NGS) panels.
While these advances in the renal tumor classification have been adopted in large academic centers with dedicated genitourinary (GU) pathology programs and reference laboratory resources, the extent to which they have been integrated into routine pathology practice globally remains poorly characterized. 3 Pathologists practicing in community hospitals, resource-limited settings, or countries with different healthcare infrastructure may face significant barriers in accessing novel biomarkers, molecular studies, and educational materials. 3 These disparities can directly affect the accuracy of diagnosis, the ability to identify hereditary tumor syndromes, and eligibility for targeted therapeutic agents. Specifically, we examined pathologists familiarity with the 2022 WHO renal tumor classification, the availability and utilization of ancillary diagnostic modalities, and the practical barriers encountered in the resolution of diagnostically challenging tumors.
Methods
Survey Design
A 30-question online survey titled “The Evaluation of Renal Tumor Diagnostics in Global Pathology Practice” was designed by the authors and administered via SurveyMonkey (SurveyMonkey Inc., San Mateo, CA, USA, Supplemental Data). The survey was structured to address 4 domains: (1) respondent demographics and practice setting, (2) experience with renal tumor specimens and uncommon entities, (3) familiarity with the 2022 WHO classification and perceived barriers to access up-to-date information and practice, and (4) availability and turnaround times of ancillary diagnostic tools (IHC, FISH, and NGS) and mechanisms for resolving challenging tumors. The full questionnaire is available as a supplementary file.
Participant Eligibility and Recruitment
Pathologists who encounter kidney tumor specimens in their clinical practice were eligible to participate. The survey was distributed via social media (X, formerly known as Twitter) as well as email to members of pathology professional networks and societies. Completion of the survey indicated willingness to participate, and respondents could also choose to participate anonymously. Three participants who did not consent were excluded, leaving a maximum of 424 consenting respondents. Among those, 399 (94.8%) confirmed active exposure to renal tumor pathology and were included in the primary analysis.
Data Collection and Ethical Considerations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Responses were collected in a private SurveyMonkey account where only 3 authors had access. Individual identifying information was not disclosed, and all data were analyzed and reported in aggregate only. As the survey was entirely voluntary and involved no collection of personally identifiable information, formal institutional review board (IRB) or research ethics committee (REC) approval was not required under applicable guidelines for observational, non-interventional survey research. Participation was optional and implied informed consent, with respondents free to withdraw at any time. No patient data, biological specimens, or sensitive personal information were collected. Data were stored securely and used solely for the purposes of this research. The study complied with applicable data protection regulations, including the General Data Protection Regulation (GDPR), where relevant.
Statistical Analysis
Statistical analyses were performed using SPSS software (version 26; IBM Corp., Armonk, NY). Descriptive statistics were calculated for each question. For questions permitting multiple responses, proportions were calculated relative to the number of respondents answering that question. Subgroup analyses were performed by practice setting, GU training background, years of experience, and geographic region (primarily US vs non-US where applicable). Two-proportion z-tests (2-sided) were used for pairwise comparisons of binary proportions. Chi-square tests of independence were applied to multi-group categorical comparisons. Kruskal–Wallis and Mann–Whitney U tests were used for comparisons of ordinal WHO familiarity scores. Because the same respondents answered IHC ordering questions for all 3 morphological categories (clear cell, eosinophilic, and papillary), McNemar tests with continuity correction were used to compare paired proportions within respondents. Statistical significance was set at 2-sided α = 0.05. All subgroup analyses were exploratory and post hoc.
Results
Response Rate and Participant Demographics
Of the 427 pathologists who accessed the survey, 424 (99.3%) consented to participate. Of these, 422 completed the demographic section, and 399 (94.8%) confirmed they encounter kidney tumor specimens in their practice; these 399 respondents constitute the primary study population. Responses were received from 45 countries (Puerto Rico was considered US territory) (Figure 1A). The 5 most represented countries were the United States (n = 75, 18.8%), Egypt (n = 63, 15.8%), Turkey (n = 50, 12.6%), the United Kingdom (n = 35, 8.8%), and India (n = 29, 7.3%). Among the 75 responses from the United States (Figure 1B), representing 24 states and Puerto Rico, the highest response rates were recorded from Texas (n = 13, 17.6%), New York (n = 10, 13.5%), and California (n = 6, 8.1%).
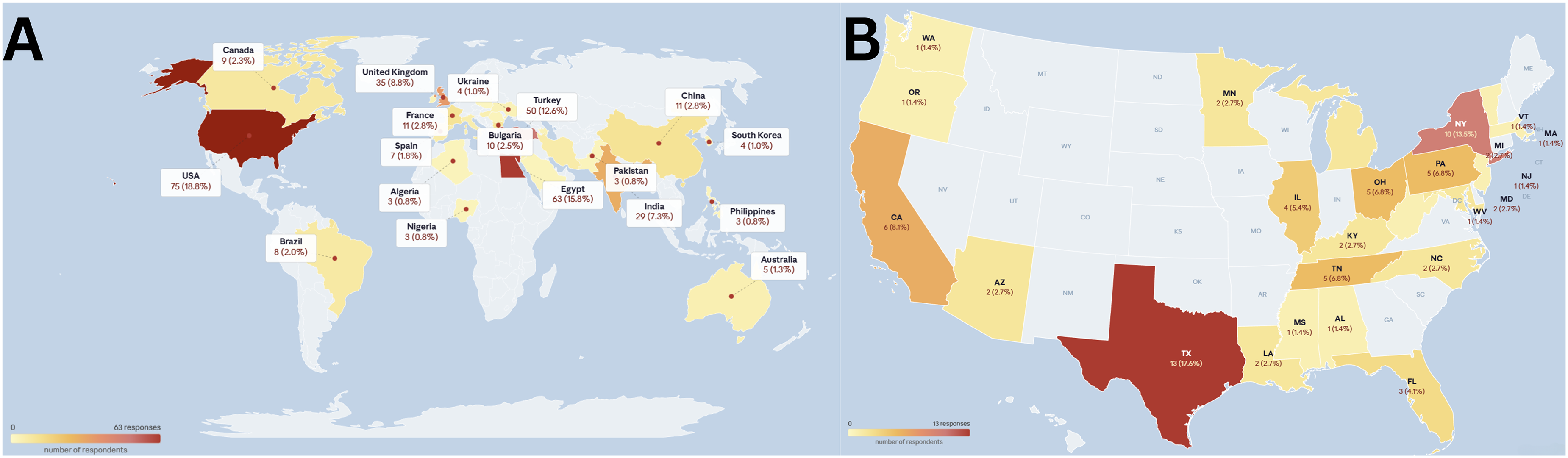
Global and US distribution of survey respondents. (A) World map illustrating the geographic distribution of the 399 survey respondents. Color intensity reflects the number of respondents per country. The 5 most represented countries were the United States (n = 75, 18.8%), Egypt (n = 63, 15.8%), Turkey (n = 50, 12.6%), the United Kingdom (n = 35, 8.8%), and India (n = 29, 7.3%). (B) Detailed map of the United States showing the state-level distribution of the 75 American respondents. Color intensity corresponds to the proportion of US respondents from each state. The highest response rates were recorded from Texas (n = 13, 17.6%), New York (n = 10, 13.5%), and California (n = 6, 8.1%).
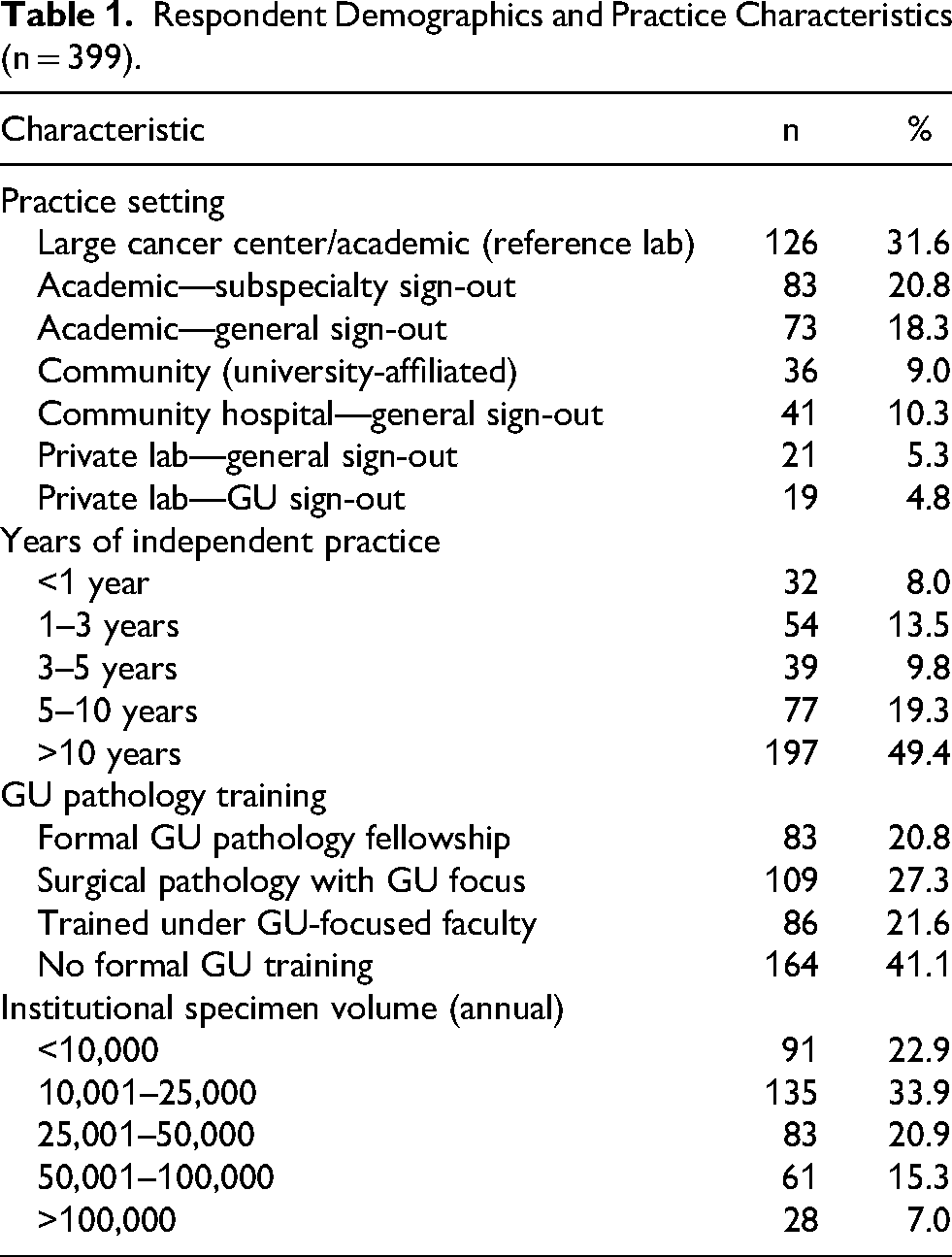
Regarding practice setting, the largest proportions worked at large cancer centers or academic institutions with reference laboratory services (31.6%, n = 126), academic departments with subspecialty sign-out (20.8%, n = 83, Figure 2A), or academic departments with general sign-out (18.3%, n = 73), collectively representing 70.7% of respondents. Community and private practice settings accounted for the remainder (Table 1). Almost half of the respondents (49.4%, n = 197) had more than 10 years of independent practice (Figure 2B). A notable 41.1% (n = 164) reported no formal GU pathology training, while 20.8% (n = 83) had completed a dedicated GU pathology fellowship. Regarding institutional specimen volume, the most common category was 10,001–25,000 specimens annually (33.9%, n = 135, Figure 2C).

Respondent demographics (n = 399). Horizontal bar charts summarizing the practice setting (A), years of independent practice (B), and genitourinary pathology training background (C) of the 399 survey respondents. The majority practiced in academic or high-resource settings (70.7%), nearly half had more than 10 years of experience (49.4%), and 41.1% reported no formal GU pathology training. The majority of respondents practiced in academic or high-resource settings, indicating that the reported resource limitations may underestimate challenges encountered in less specialized practice environments.
Respondent Demographics and Practice Characteristics (n = 399).
With respect to renal tumor exposure (Figure 3A, B), 49.8% of respondents (n = 198) encountered fewer than 5 renal biopsy or resection specimens per week, while only 3.5% (n = 14) saw more than 25 per week. Uncommon renal tumors (ie, entities other than clear cell RCC, classical papillary RCC, chromophobe RCC, oncocytoma, or angiomyolipoma) were encountered at least once a week by 9.6% (n = 38), while 33.9% (n = 135) encountered them only a few times per year, and 18.8% (n = 75) encountered them rarely.
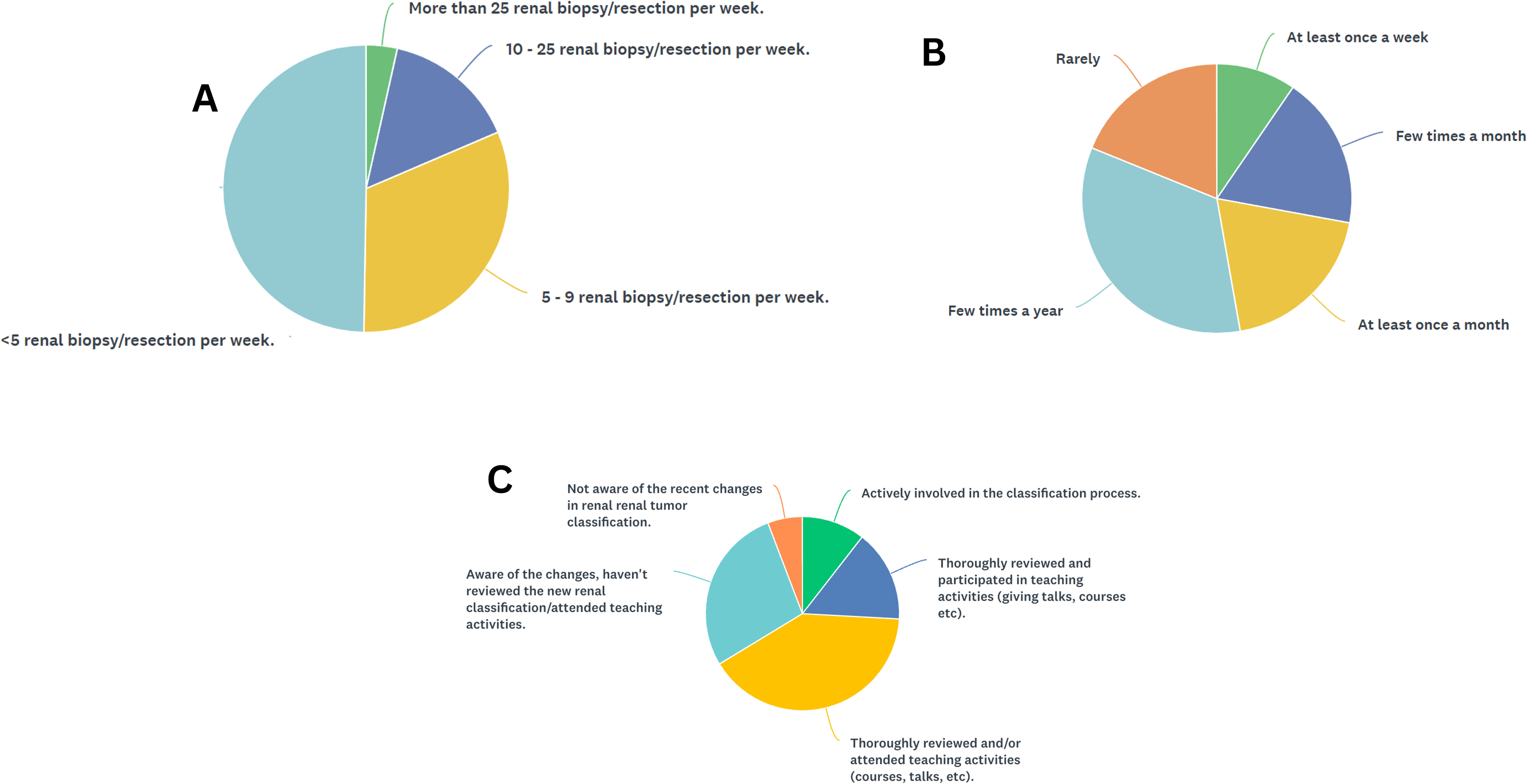
Renal tumor exposure and familiarity with the 2022 WHO Classification. Pie charts showing (A) the volume of renal biopsy/ resection specimens encountered per week, (B) the frequency of encountering uncommon renal tumor entities, and (C) the level of self-reported familiarity with the 2022 WHO Classification of renal tumors. The majority of respondents had low-to-moderate renal tumor volume, infrequently encountered uncommon entities, and 66.3% reported at least thorough familiarity with the current classification.
Familiarity With the 2022 WHO Classification
When asked about participants’ interaction with the 2022 WHO (Figure 3C), 10.6% (n = 42) had been actively involved in the classification process, and 15.3% (n = 61) had thoroughly reviewed it and participated in teaching activities. An additional 40.5% (n = 161) had thoroughly reviewed the classification and/or attended teaching activities, while 27.9% (n = 111) were aware of the changes but had not reviewed them in depth. Only 5.8% (n = 23) were unaware of recent classification changes. In aggregate, 66.3% of respondents reported at least thorough familiarity with the 2022 WHO classification. Familiarity with the 2022 WHO classification differed significantly by years of experience (p < .001): senior pathologists with more than 10 years of practice had significantly higher classification familiarity than early-career pathologists with fewer than 3 years of experience. Familiarity also varied significantly by practice setting, with high-resource academic pathologists reporting higher familiarity than community-based pathologists.
WHO classification familiarity had a direct impact on ordering of novel biomarkers (Figure 4). Pathologists familiar with the 2022 classification were significantly more likely to order SDHB (38.3% vs 11.2%, p < .001) and FH (28.0% vs 10.4%, p < .001) for eosinophilic tumors. In contrast, WHO familiarity did not significantly affect the tendency to skip IHC for morphologically characteristic clear cell tumors (43.2% vs 45.5%, p = .657) or papillary tumors (p = .153), nor did it significantly influence referral rates for expert consultation (p = .807). This pattern suggests that classification knowledge selectively improves diagnostic workup for challenging and potentially syndromic entities without disrupting routine practice.
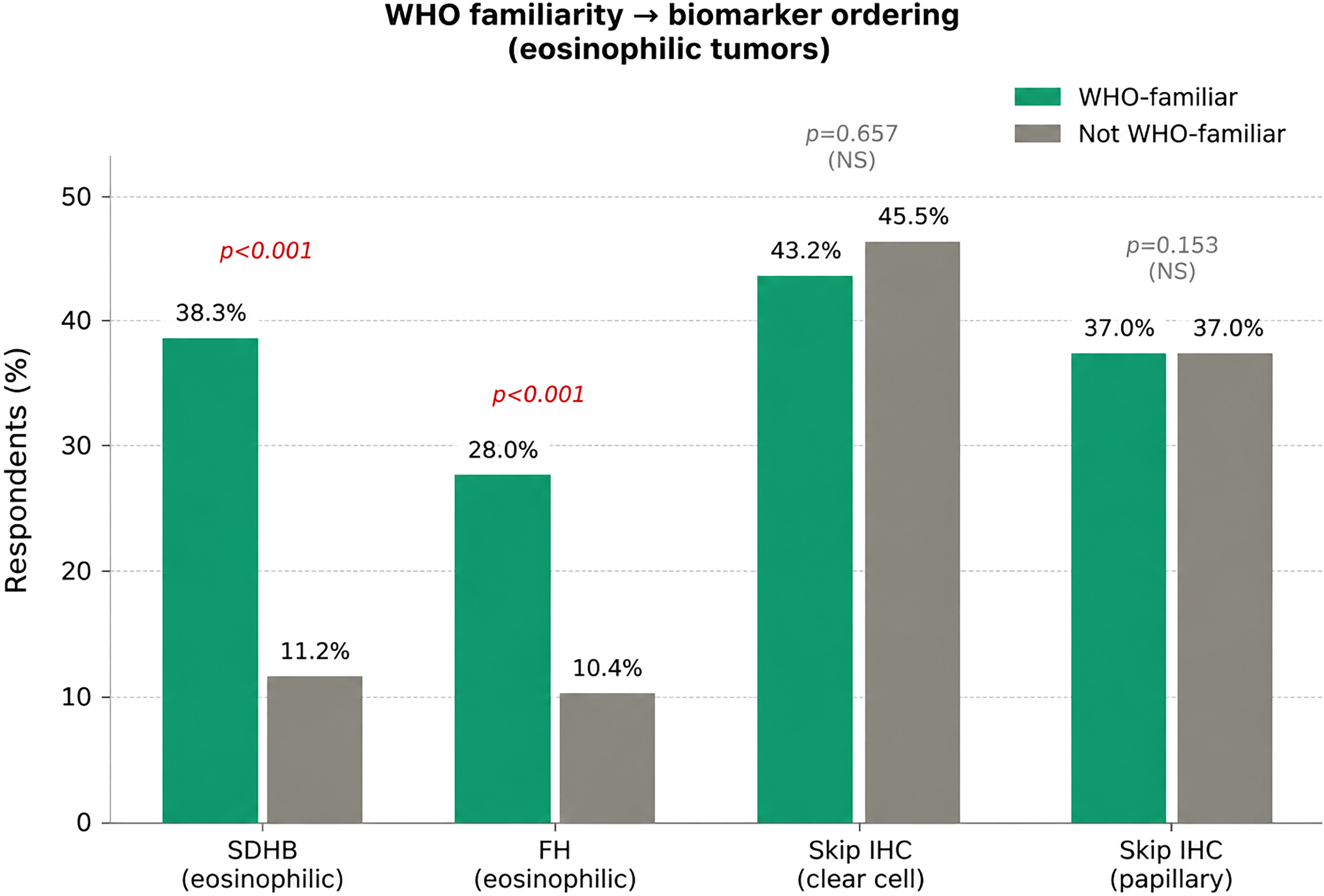
Impact of WHO familiarity on practice patterns. Bar charts illustrating the effect of 2022 WHO classification familiarity on biomarker ordering patterns. Greater familiarity with the updated classification was associated with increased use of novel biomarkers for diagnostically challenging renal tumors, suggesting that educational exposure directly influences diagnostic practice.
Among the 59.8% who perceived challenges in keeping up with classification changes, the most commonly cited barriers were the fast pace of changes (30.2%, n = 120), financial limitations preventing conference attendance (17.3%, n = 69), high clinical workload precluding participation in educational activities (15.1%, n = 60), and lack of experienced urologic pathologists at their institution (12.1%, n = 48). Access to reference materials was also a barrier for 9.1% (n = 36). Non-US pathologists were significantly more likely to report financial barriers to conference attendance (19.1% vs 3.1%; p = .002) and difficulty accessing WHO reference materials (11.0% vs 1.5%; p = .017). Notably, 40.2% (n = 160) perceived no challenges to keeping current with renal tumor classification.
IHC, FISH, and Molecular Resource Availability
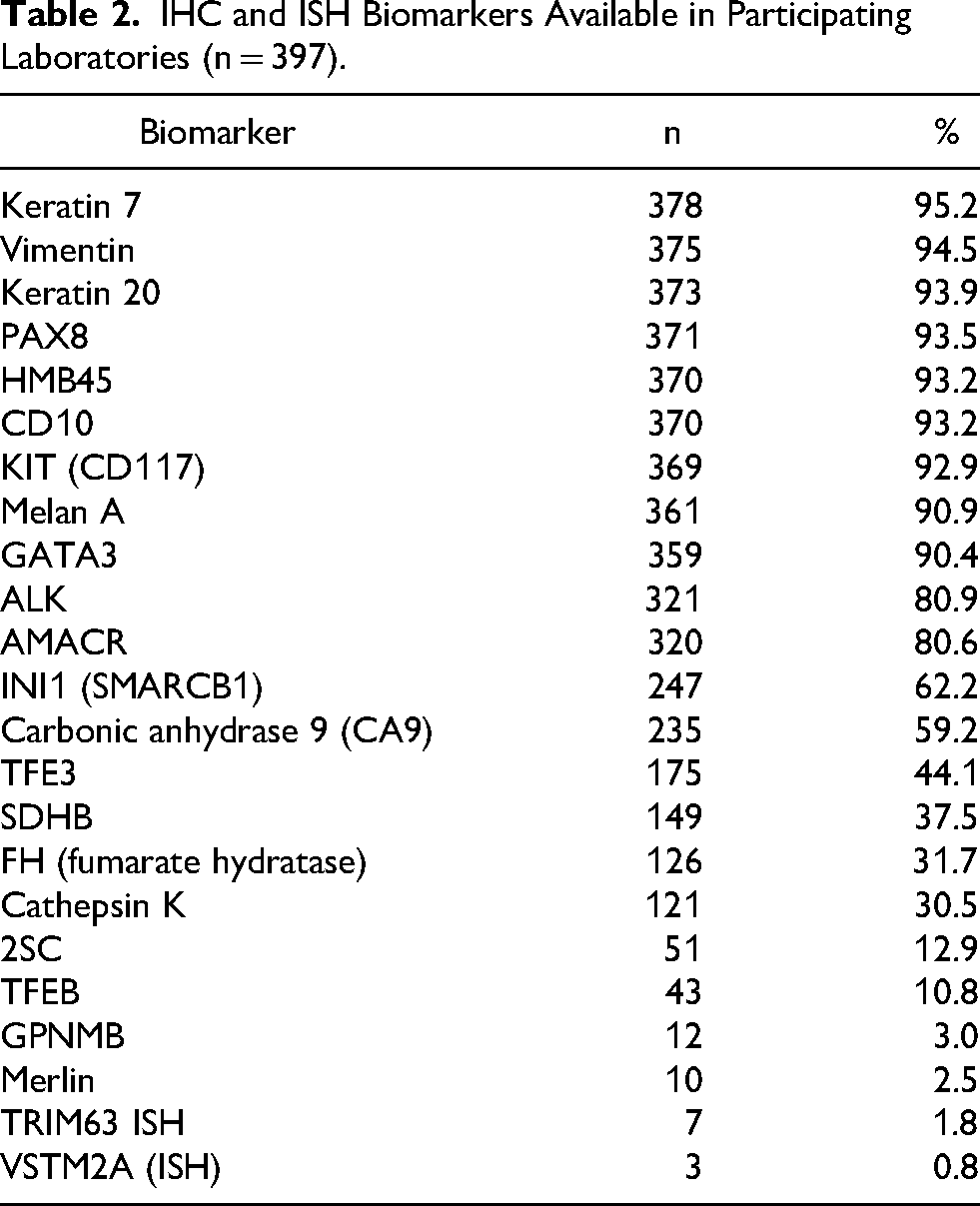
IHC was available for 96.0% (n = 381; Figure 5A) of participants. Among labs with IHC, conventional markers such as keratin 7 (95.2%), PAX8 (93.5%), CD10 (93.2%), and KIT (92.9%) were broadly available, while CA9 was available for 59.2% (Table 2). By contrast, markers increasingly critical for the 2022 WHO classification, including SDHB (37.5%), FH (31.7%), cathepsin K (30.5%), TFE3 IHC (44.1%), 2SC (12.9%), TFEB IHC (10.8%), GPNMB (3.0%), Merlin (2.5%), TRIM63-ISH (1.8%), and VSTM2A-ISH (0.8%), were available in a substantially smaller proportion of laboratories.
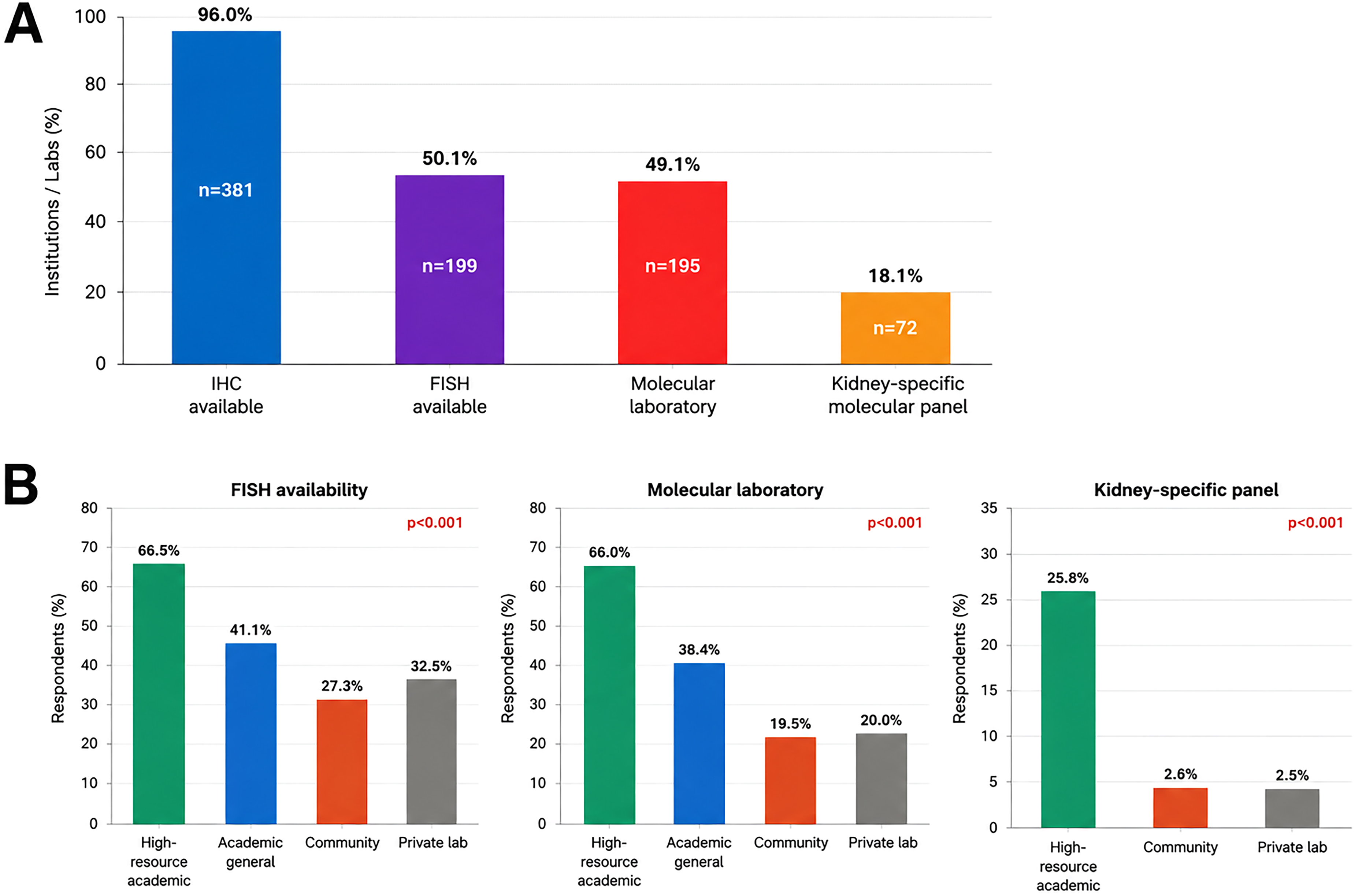
Availability of ancillary diagnostic resources. (A) Overall availability of immunohistochemistry (IHC), fluorescence in situ hybridization (FISH), molecular laboratory access, and kidney-specific molecular panels across participating institutions. While IHC was nearly universally available (96.0%), FISH, molecular laboratories, and kidney-specific panels were present in only half or fewer of institutions. (B) Availability of FISH, molecular laboratory access, and kidney-specific panels stratified by practice setting. All 3 resources were significantly more concentrated in high-resource academic centers compared to community and private laboratory settings (all p < .001).
IHC and ISH Biomarkers Available in Participating Laboratories (n = 397).
FISH testing was available in half of responding institutions (50.1%, n = 199). Of the kidney-relevant FISH tests, ALK FISH was the most commonly available (35.5%, n = 141), followed by TFE3 FISH (25.9%, n = 103) and TFEB FISH (14.9%, n = 59). A molecular laboratory was present at 49.1% (n = 195) of institutions; however, kidney-specific gene or fusion panels were available at only 18.1% (n = 72) of institutions, indicating that a general NGS panel without renal-specific content was more common. Kidney-specific molecular panels were significantly more available in the US than in non-US countries overall (35.4% vs 13.6%, p < .001).
Resource availability varied markedly by practice setting (Figure 5B). FISH was available to 66.5% of respondents at high-resource academic centers, 41.1% at academic general departments, 27.3% in community settings, and 32.5% in private laboratories (p < .001). Molecular laboratory access followed a similar gradient: 66.0%, 38.4%, 19.5%, and 20.0%, respectively (p < .001). Kidney-specific molecular panels were most concentrated in high-resource academic centers (25.8%) and nearly absent in community (2.6%) and private (2.5%) settings (p < .001). By contrast, in-laboratory IHC availability did not differ significantly between high-resource academic and community settings (98.1% vs 98.7%, p = .725), confirming that conventional IHC is the one diagnostic modality distributed equitably across all practice types. Notably, overall FISH availability and overall WHO classification familiarity did not differ significantly between US and non-US respondents as aggregated groups (p = .060 and p = .169, respectively).
IHC Utilization by Morphological Category
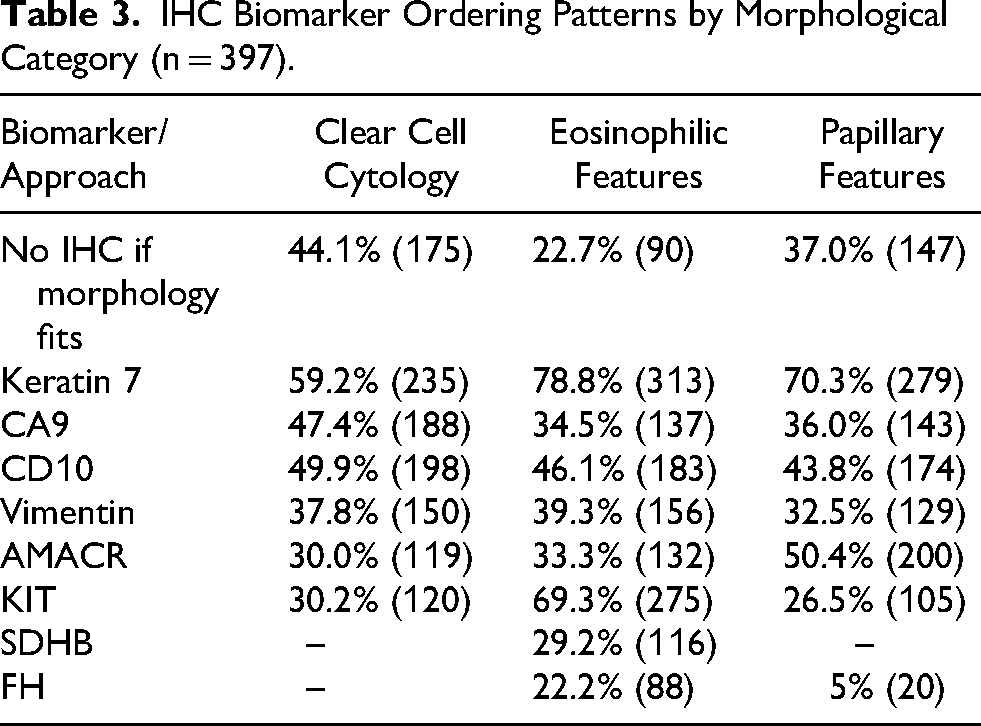
When describing their approach to IHC ordering, respondents showed variation based on tumor morphology (Table 3; Figure 6A, B). For tumors with clear cell cytology, 44.1% (n = 175) reported that they do not routinely order IHC when morphology is characteristic of a common clear cell neoplasm. Among those who do order IHC in this context, the most commonly ordered markers were keratin 7 (59.2%), CD10 (49.9%), and CA9 (47.4%). For eosinophilic renal tumors, only 22.7% (n = 90) reported withholding IHC when morphology was characteristic, and the most frequently ordered markers in this category were keratin 7 (78.8%), KIT (69.3%), and CD10 (46.1%). For papillary tumors, 37.0% (n = 147) did not order IHC when morphology was characteristic. Keratin 7 (70.3%) and AMACR (50.4%) were the most commonly utilized markers.
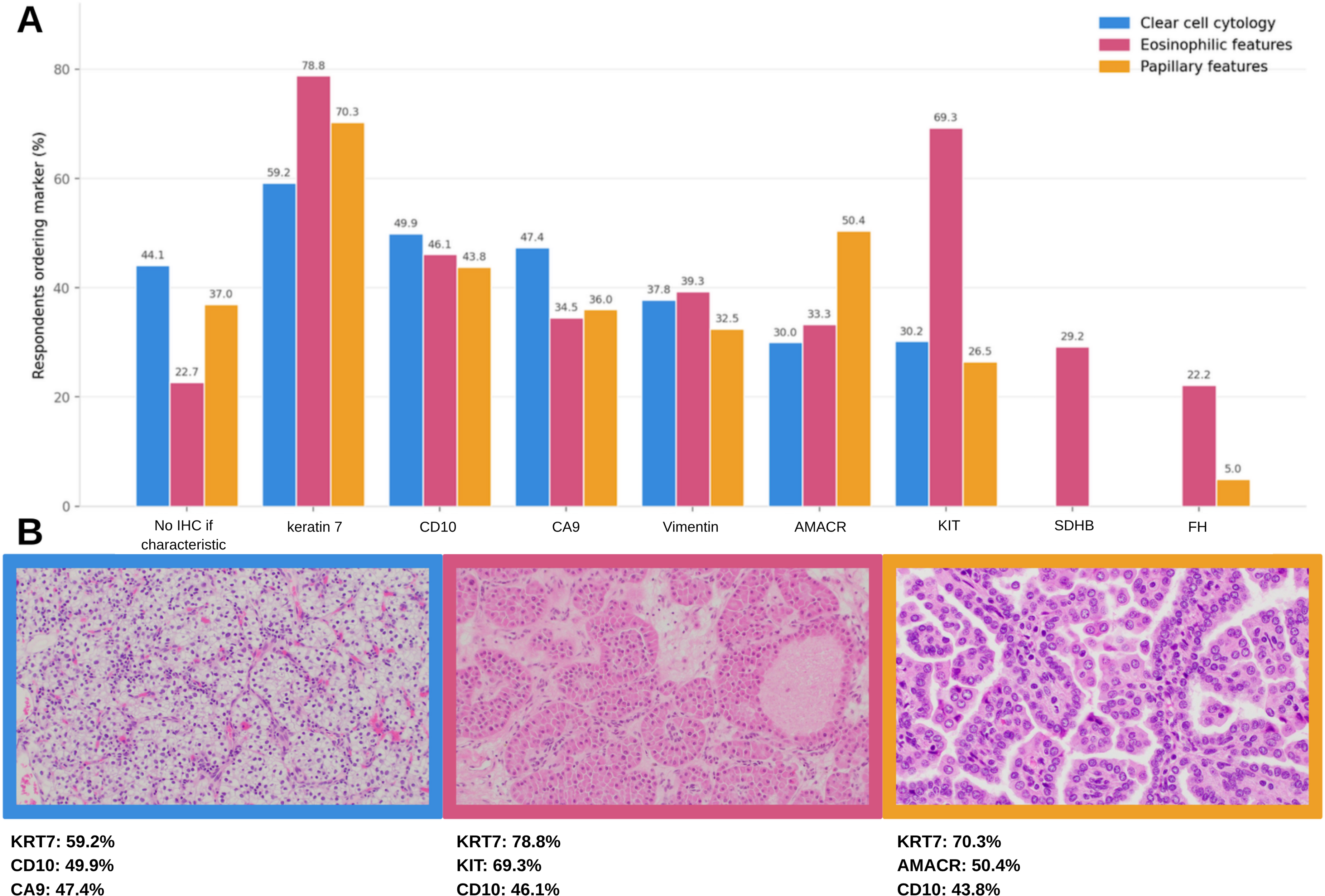
IHC biomarker ordering patterns by morphological category. (A) Grouped bar chart showing the proportion of respondents ordering each IHC marker stratified by tumor morphology (clear cell, eosinophilic, and papillary) and (B) most commonly ordered IHCs for different morphologies.
IHC Biomarker Ordering Patterns by Morphological Category (n = 397).
Resolution of Diagnostic Challenges
Regarding strategies for managing diagnostically challenging renal tumors, the most common approach was consulting a colleague with GU pathology experience (64.0%, n = 254), followed by referral to an external expert for consultation (40.3%, n = 160). Regularly scheduled GU pathology consensus meetings were available to 22.4% (n = 89) of respondents. Importantly, 6.6% (n = 26) reported having no support available for challenging scenarios. Pathologists without formal GU training were more than twice as likely to report no available support compared to GU-trained colleagues (10.4% vs 4.5%, p = .021) and were also significantly less likely to have access to regularly scheduled GU consensus meetings (16.5% vs 26.9%, p = .013) (Figure 7).
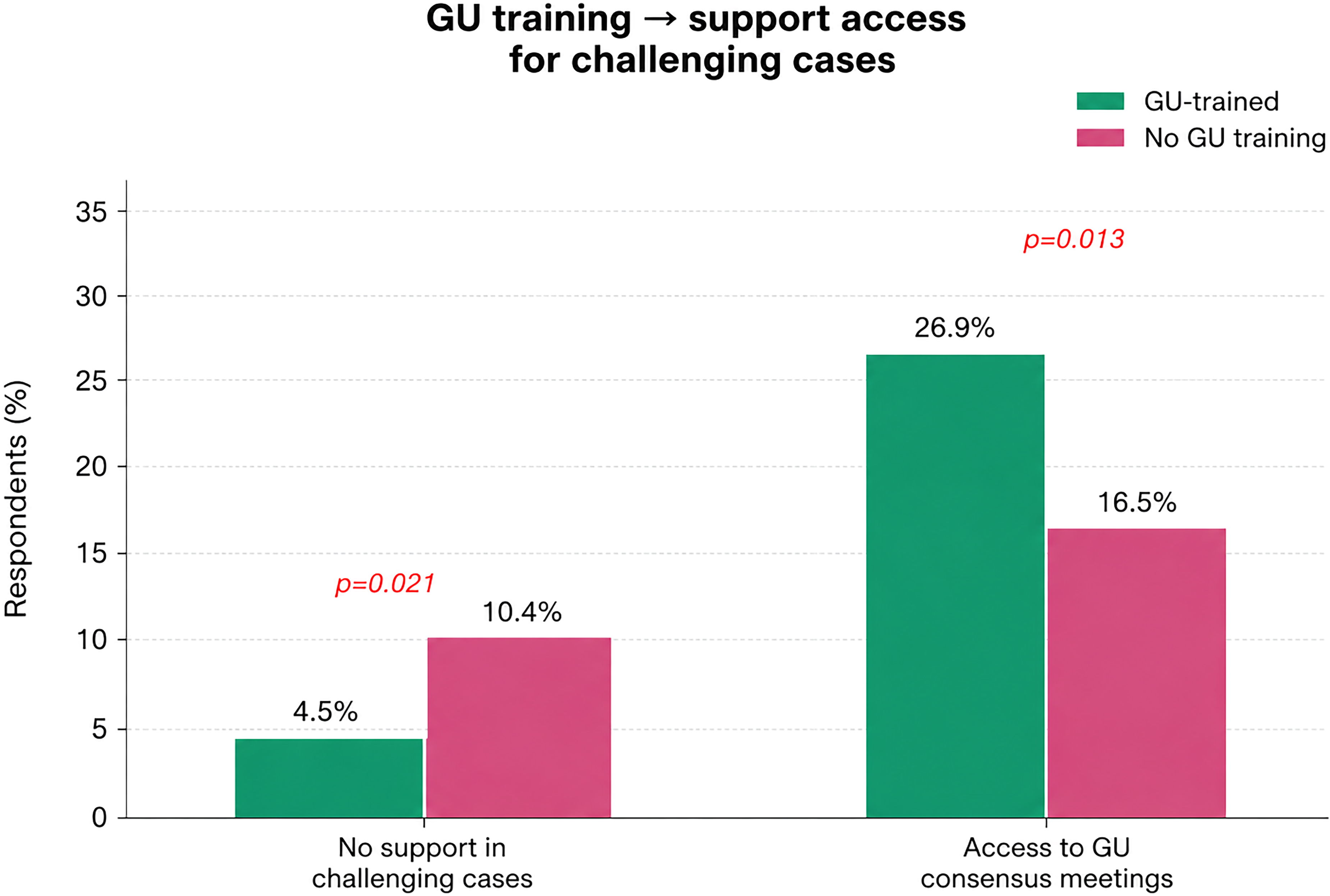
Association between genitourinary (GU) pathology training and access to support for challenging lesions. Respondents with GU training reported significantly lower rates of having no support in challenging tumors compared to those without GU training (4.5% vs 10.4%, p = .021).
The majority of respondents (63.5%, n = 252) reported sending fewer than 5% of kidney specimens out for additional work-up or expert consultation, while 10.6% (n = 42) reported that send-out testing or expert consultation was not available to them at all.
Figure 8 illustrates a subset of relatively uncommon renal tumors that may pose diagnostic challenges.

Representative examples of relatively uncommon and diagnostically challenging renal tumors and their corresponding immunohistochemical profiles. (A) TFE3-rearranged renal cell carcinoma and (B) diffuse nuclear TFE3 immunoreactivity. (C) Fumarate hydratase-deficient renal cell carcinoma with characteristic eosinophilic cytology and (D) Loss of FH expression in tumor cells. (E) Succinate dehydrogenase (SDH)-deficient renal cell carcinoma and (F) GATA3 expression in SDH-deficient RCC.
Diagnostic Turnaround Times
IHC was generally the most rapidly available ancillary test: 37.3% (n = 148) of respondents received results within 1 day, and 44.6% (n = 177) within 2–5 days. FISH results were available within 1–3 days for 10.3% (n = 41), within 4–6 days for 14.6% (n = 58), and required a week or more for 23.7% (n = 94); 49.9% reported FISH was unavailable in their lab. For NGS, 56.2% lacked in-house capability; of those with access, 20.4% received results within 1–2 weeks, and 21.2% waited more than 2 weeks.
For send-out assays, access was also limited: 30.6% reported send-out IHC was unavailable, 45.1% could not access send-out FISH, and 49.1% had no access to send-out molecular testing. Among those with access, wait times were considerable, particularly for send-out FISH (>1 week in 38.8%) and send-out NGS (>2 weeks in 32.2%).
Discussion
This international survey, comprising nearly 400 pathologists from 45 countries, provides the first large-scale global assessment of diagnostic practices for renal tumors. Our data reveal a complex landscape in which access to modern diagnostic tools is highly variable, and a significant number of practicing pathologists face barriers in both resources and education that may compromise their ability to fully implement the 2022 WHO renal tumor classification.
The 2022 WHO classification represents one of the most substantive revisions to the renal tumor taxonomy in recent years. 2 The formalization of molecularly defined entities means that the accurate diagnosis now frequently requires more than morphology alone. Identification of tumors that are related to germline mutations has direct clinical implications for the patient and family, including referral for genetic counseling.4,5 Similarly, the emergence of targeted therapies has made precise subclassification increasingly relevant for treatment selection. 6 Against this, our finding that critical biomarkers such as FH (31.7%), SDHB (37.5%), cathepsin K (30.5%), and GPNMB (3%) are available in only a minority of surveyed laboratories is concerning. Moreover, carbonic anhydrase 9 (CA9), which is a canonical biomarker in the diagnostic work-up of renal tumors with clear cell cytology was available in less than 60% of the labs overall. These markers occupy a central role in the 2022 WHO classification for the workup of tumors with eosinophilic and/or papillary morphology and potential syndromic tumors (2).
Access to FISH (50.1%) and NGS (49.1%) was available to approximately half of respondents, but kidney-specific molecular panels were present in only 18.1% of institutions. This means that even where a molecular lab exists, the testing available may be oncology-broad panels not optimized for the gene fusions or mutations most relevant to renal tumor entities (eg, TFE3, TFEB, ALK, ELOC, MET, TSC1/2 alterations). The practical consequence is that diagnosis of entities such as ALK-rearranged RCC, MiT family translocation-associated RCC, and emerging novel entities may require external referral, contributing to delays and variability in diagnostic reporting.
Familiarity with the 2022 WHO classification was encouraging overall, with 66.3% of respondents reporting thorough review or active involvement. However, the 33.7% with limited familiarity represents a substantive proportion of practicing pathologists who may be applying outdated diagnostic criteria. Importantly, barriers to keeping current were diverse: the fast pace of classification changes (30.2%), financial limitations (17.3%), and clinical workload (15.1%) are barriers that disproportionately affect pathologists in lower-resource settings and high-volume practices.
Our findings regarding IHC ordering practices suggest some variation in approach across morphological categories. The relatively higher IHC utilization for eosinophilic tumors (77.3% ordering at least 1 marker) compared to clear cell or papillary tumors likely reflects the more challenging differential diagnosis inherent to the eosinophilic category, which includes oncocytoma, eosinophilic chromophobe RCC, and a growing list of novel eosinophilic neoplasms. 7
The finding that 6.6% of respondents have no support available for challenging renal lesions is particularly notable. In this context, digital pathology may play an important role in facilitating referral and collaborative diagnostic support, particularly in settings where subspecialty expertise or ancillary diagnostic resources are limited. 8
Several limitations of this study should be acknowledged. The survey was distributed via professional networks and may over-represent pathologists with an existing interest in renal tumor pathology, potentially leading to an overestimate of familiarity with the WHO classification. The high representation of academic pathologists (70.7%) and the geographic skew toward the United States, Egypt, and Turkey may limit generalizability to community or private practice settings in other regions with subject to less resourceful pathology practice setting. Certain questions reflect self-reported behavior, which may not represent the actual pathology practice in the countries where those pathologists practice. Additionally, as with all cross-sectional surveys, the data reflect a single time point and may not capture rapid changes in resource availability that occur in dynamic healthcare systems. Future studies, including longitudinal follow-up and analysis by geographic subgroups (eg, income level of country, presence vs absence of subspecialty training), would further illuminate practice disparities. Another limitation is the lack of interrogation about how pathology is operated under the health authorities for each country, which may have different referral, insurance coverage, and practice settings. Finally, all subgroup analyses were exploratory and post hoc, having not been pre-specified in the survey design. These findings should be treated as hypothesis-generating rather than confirmatory, and independent replication is needed.
Conclusions
This international survey demonstrates substantial heterogeneity in the resources available for renal tumor diagnosis across global pathology practices. While conventional IHC markers are broadly accessible, the novel biomarkers central to the 2022 WHO classification are available in only a minority of laboratories worldwide. FISH and kidney-specific molecular panels remain restricted to approximately half or fewer of participating institutions. These findings have direct implications for the accuracy of renal tumor subclassification, identification of hereditary tumor syndromes, and access to molecularly guided therapy. Concerted international efforts are needed to improve access to essential diagnostic tools, expand educational initiatives, and foster consultation networks that support pathologists practicing in resource-limited settings. Pathology societies and classification boards should consider the global resource landscape when formulating diagnostic recommendations and developing educational programs.
Supplemental Material
sj-docx-1-ijs-10.1177_10668969261458406 - Supplemental material for The Evaluation of Renal Tumor Diagnostics in Global Pathology Practice
Supplemental material, sj-docx-1-ijs-10.1177_10668969261458406 for The Evaluation of Renal Tumor Diagnostics in Global Pathology Practice by Nazif Alperen Yıldırım, Laila Farid, Dilara Akbulut, Sana Malik, Maryna Slisarenko, Dilek Ertoy Baydar, Manana Jikurashvili, Elza Tjio, Yazgi Koy, Onur Ertunc, Levente Kuthi, Ahmed Montasser, Laurence Galea, Anandi Lobo, Dimitrios Korentzelos, Maria Sarah Lagarde-Lenon, Busra Yaprak Bayrak, Burcu Biltekin, Liang Cheng, Sean R Williamson, Ankur R Sangoi and Mahmut Akgul in International Journal of Surgical Pathology
Footnotes
Acknowledgments
ORCID iDs
Author Con tributions
M.A., D.A., D.E.B., A.R.S., and S.R.W. designed the survey. N.A.Y. prepared the first draft of the manuscript. L.C., M.A., N.A.Y., B.B., M.S., A.M
Ethics Approval
According to institutional and national guidelines, formal ethics committee approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data were collected anonymously. The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request, subject to applicable ethical and institutional considerations.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.