
Abstract
This study was designed to compare the tensile strength of ruptured Achilles tendons repaired using either the triple bundle technique or the Krakow locking loop technique. Eight pairs of fresh frozen cadaveric Achilles tendons were harvested. A simulated “Achilles tendon rupture” was created 4 cm from the calcaneal insertion in all sixteen tendons by transversely cutting the tendon with a scalpel. One Achilles tendon “rupture” of a pair was repaired using the triple bundle technique, while the other tendon of the pair was repaired using the Krakow locking loop technique. Then, using a servohydraulic testing machine, each tendon was tested to failure in tension at a displacement rate of 2.54 cm/sec. The average rupture load for the triple bundle technique was 453 N (range 397 ñ 549 N), while the average rupture load for the Krakow locking loop technique was 161 N (range 121 ñ 216 N). This difference in averages represents a statistically significant superiority of 2.8 to 1 (p < 0.001) in favor of the triple bundle technique.
INTRODUCTION
Management of acute Achilles tendon injuries remains controversial. Although surgical repair is frequently recommended for active patients, there is no clear consensus on the method of repair or rehabilitation. Currently some surgeons institute early range of ankle motion after Achilles tendon repair, with the intent to hasten recovery and improve outcome 4,9 . This approach requires a durable and stout repair. Both the Krakow locking loop technique and the triple bundle repair have been reported to be successful, in conjunction with early range of ankle motion, for the treatment of acute Achilles tendon rupture. 1,4,5,9
In 1995 Watson et al. reported a biomechanical study in which they compared the Kessler, Bunnell and Krakow locking loop techniques of Achilles tendon repair. 12 They found that the Krakow locking loop technique was 1.58 and 1.73 times stronger than the Bunnell and Kessler techniques, respectively. Clinically, Mandelbaum et al. reported no reruptures in 29 patients after using the Krakow locking loop method with the initiation of early range of motion for treatment of acute Achilles tendon rupture. 4
Using the triple bundle repair, Marti et al. was able to begin ankle motion within a week after surgery, and, after obtaining near full motion, placed the patients into a walking cast. 5 This method was also used successfully in a study by Beskin et al. 1
Currently there are no data comparing the biomechanical strengths of the Krakow locking loop technique and triple bundle technique for the surgical repair of Achilles tendon ruptures. This study was designed to compare the tensile strengths of the Krakow locking loop and triple bundle methods.
MATERIALS AND METHODS
Sixteen fresh frozen cadaveric Achilles tendons (eight pairs), without previous evidence of injury, were collected from cadavers aged between 62 and 82 years old at death. The tendons were harvested from the musculotendinous junction to the calcaneal insertion, including a block of calcaneal bone. The distal bone block was large enough to allow two Steinmann pins to be passed through it transversely.
A simulated “Achilles tendon rupture” was created 4 cm from the calcaneal insertion in all sixteen tendons by transversely cutting the tendon with a scalpel. One tendon of each pair was placed into one of two groups, alternating the left and right limbs to prevent nonrandomization error. In group 1, one Achilles tendon “rupture” of each pair was then repaired according to the triple bundle technique (Figure 1). In group 2, the Achilles tendon from the contralateral limb was repaired according to the Krakow locking loop technique as described by Watson et al. (1995) (Figure 2). 12 All tendons were repaired with No. 1 Ethibond nonabsorbable suture material (Ethicon, Sommerville, NJ). The repair in both groups was extended 4 cm proximally and distally from the rupture site. This allowed an equal number of loops or passes proximally and distally for all sixteen repairs. All knots were tied with five square knots.
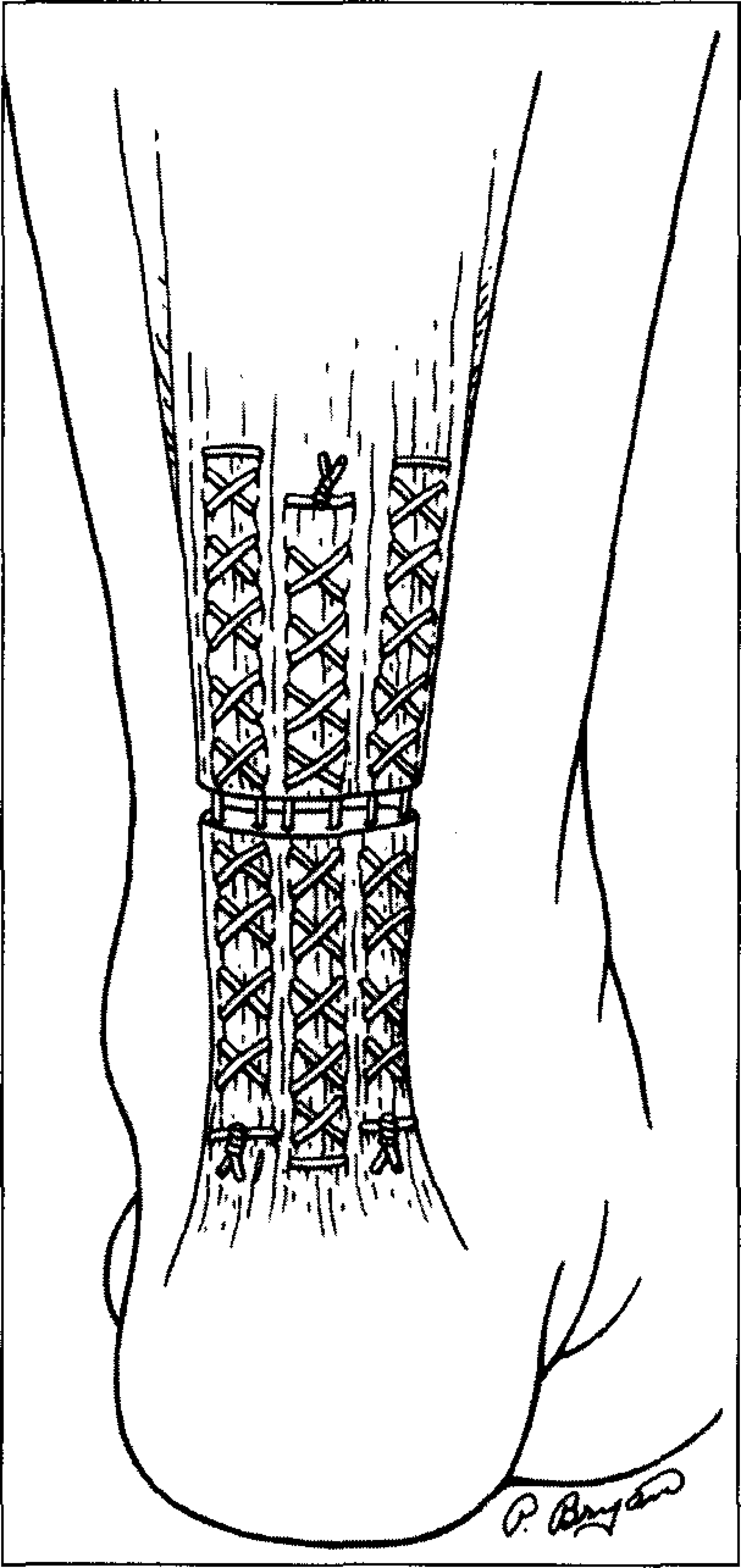
The triple bundle technique used for repair of the Achilles tendons in group one. Six suture strands cross the rupture site and the knots (three in all) are tied away from the rupture site.
Distally two Steinmann pins were drilled across the calcaneal bone block in a posterior to anterior direction at the base of the insertion of the Achilles tendon as shown in Figure 3. Each tendon was then placed into a Bionix servohydraulic testing machine (MTS Systems Corporation, Minneapolis, MN). The proximal end of the tendon was clamped in the testing machine using a specially designed soft-tissue clamp. At the distal end a chain was attached around the Steinmann pins, and the chain was clamped to the testing machine. The tendon was loaded to failure in tension at a rate of 2.54 cm/sec. This rate has already been used in a design protocol described by Watson et al. (1995); we used it in order to a correlate our results with those from their study. 12 Furthermore, we consider that this rate is within the range of rates at which loads are imposed on a Achilles tendon during ankle range of motion. The data collected from the MTS machine provided a force-displacement curve and a value of maximum force at rupture.
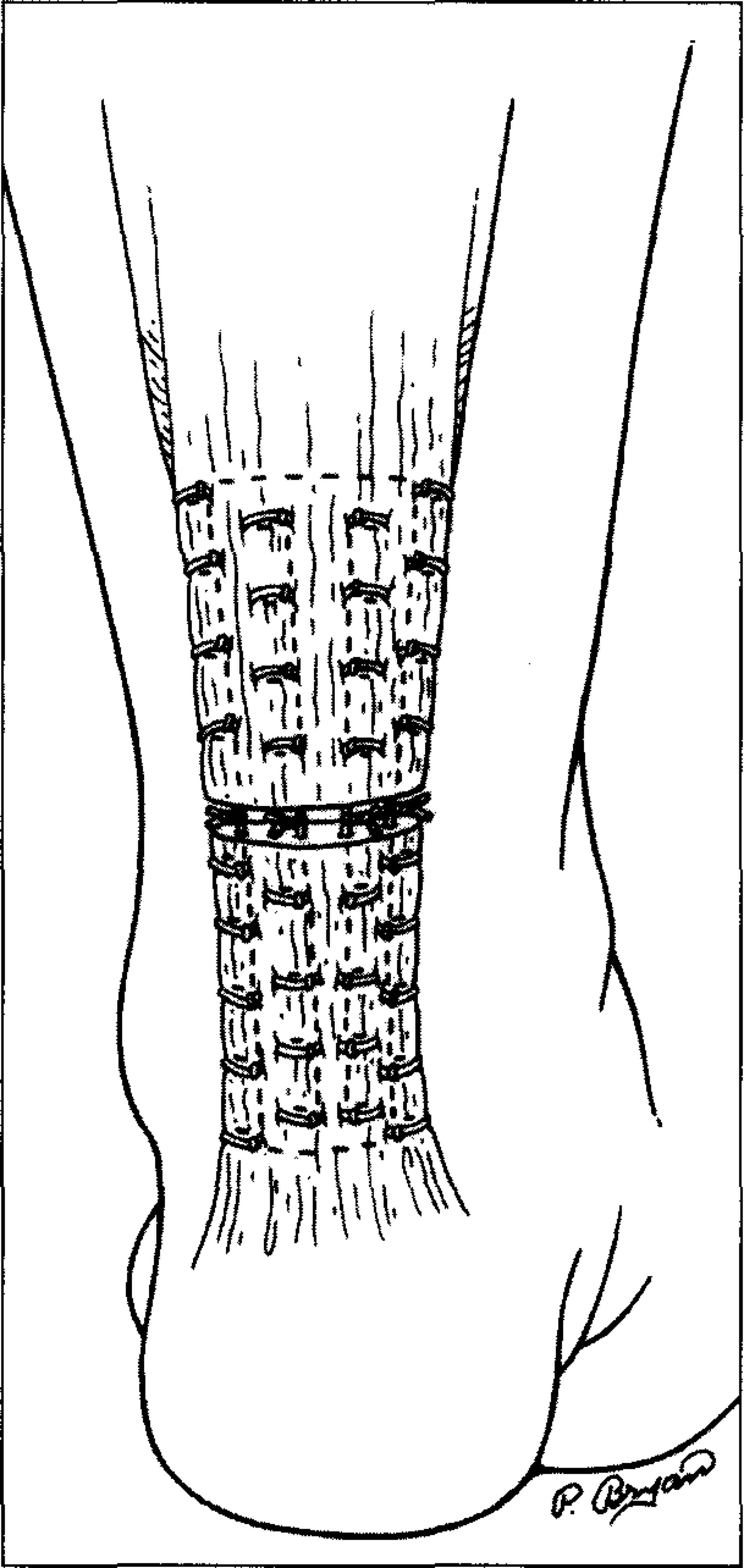
The Krakow locking loop technique used for repair of the Achilles tendons in group 2. Four suture strands cross the rupture site and the knots (four in all) are tied at the rupture site.
RESULTS
As shown in Figure 4, the mean value of force at rupture for group 1 (triple bundle technique) was 453 + 53.9 N (range 397–549 N). Failure of the repair in this group occurred in the substance of the tendon, away from the simulated rupture site, in all except three cases. In each of these three cases the central “bundle” suture broke at the knot. None of the suture repairs showed evidence of unraveling of the knot.
The mean value of force at rupture for group 2 (Krakow locking loop technique) was 161 + 31.1 N (range 121–216 N). Failure of the repair in this group occurred at the simulated rupture site in all cases. The suture failed at the knot in seven of eight cases. In one of the tendons in this group the two outer sutures unraveled at the knot; this tendon revealed the lowest value of force at rupture in this group (121 N).
Using t-test for independent groups analysis on the mean values for group 1 and 2, the difference in load to failure using tensile testing of the Krakow technique versus the triple bundle technique resulted in a p < 0.001. The highest load to failure of group 2 (216 N) was an “outlier” according to t-test analysis.
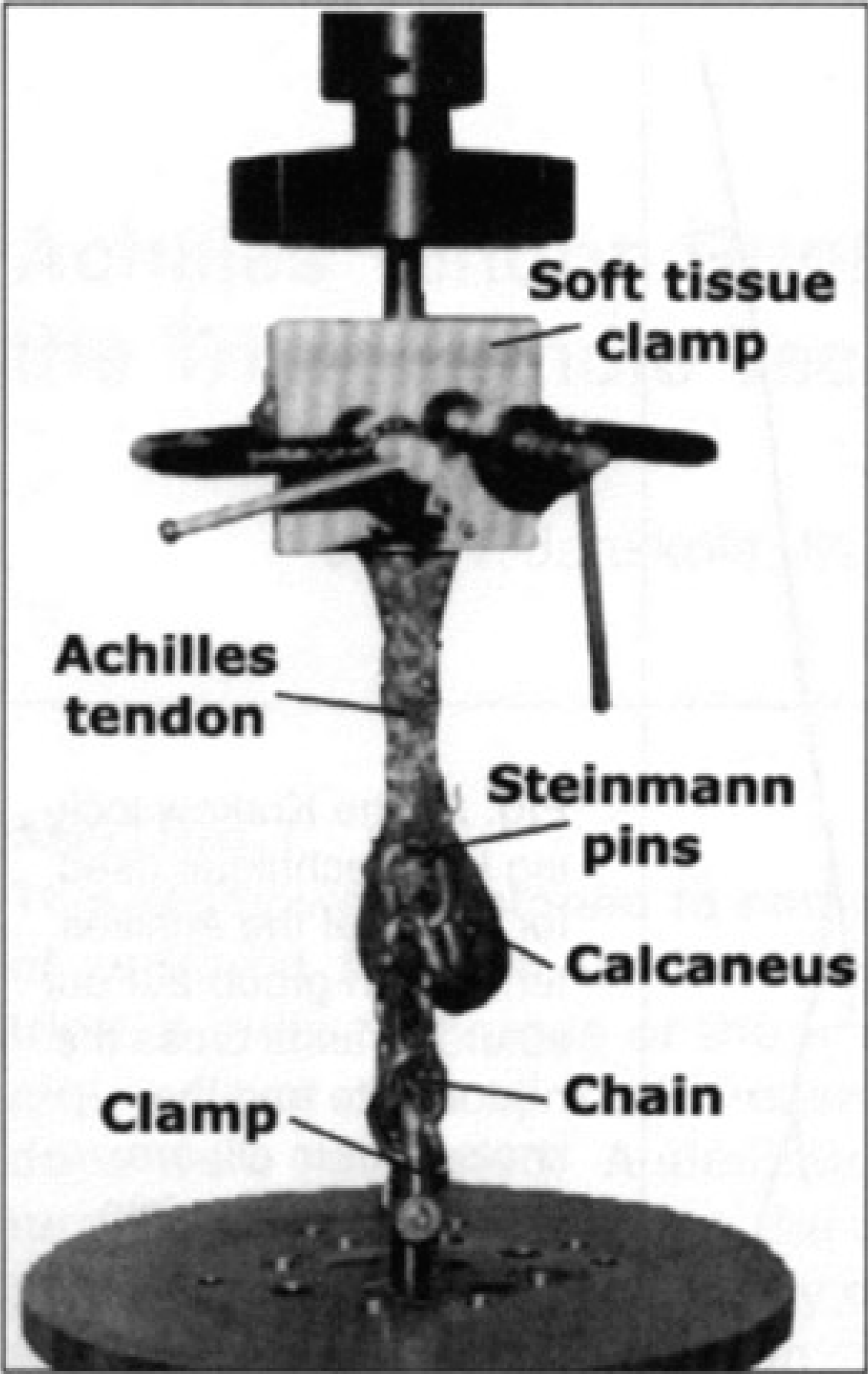
A cadaveric Achilles tendon placed in the servohydraulic testing machine after repair using triple bundle technique. The proximal end is clamped to the testing machine with a soft-tissue clamp. Distally, the calcaneus has two Steinmann pins drilled through in a posterior to anterior direction, which are then connected to a clamp with a steel chain.
DISCUSSION
The authors found that in Achilles tendon rupture repair the triple bundle technique is nearly threefold stronger in tension than the Krakow locking loop technique. This difference is, in the main, due to the increased number of strands crossing the rupture site (six with the triple bundle versus four with the Krakow technique). Biomechanical studies evaluating methods of hand flexor tendon repair have found similar differences in relation to the number of strands crossing the rupture site, i.e. four strand techniques are twice as strong, and six strand techniques three times as strong, as two strand techniques. 10 Another factor in this difference is that the knot is tied away from the rupture site in the triple bundle technique, whereas in the Krakow technique the knot is tied at the rupture site. Having the knot at the rupture site could set up a stress riser on the suture at the rupture site, and subsequent tension on the suture could result in early failure at the knot; this is supported by the fact that in seven of eight cases the suture failed at the knot in group 2 (Krakow technique). In addition, studies evaluating hand flexor tendon repairs have found that repairs usually rupture at the suture knots. 10 Theoretically, the suture could be tied away from the rupture site which might alleviate the problem and improve the tensile strength of the repair.
Currently numerous direct repair suture techniques exist for repairing acute Achilles tendon ruptures. These include the Krakow locking loop technique, 4 Kessler, 7,8,11 Bunnell, 2,8 continuous six strand suture technique, 6 and triple bundle technique. 1,5,8 Two biomechanical studies exist in the literature comparing the strength of these direct repair suture techniques. The more recent study, as previously discussed, was by Watson et al. in 1995, which showed the Krakow technique to be stronger than the Bunnell and Kessler. 12 In their manuscript, Watson et al. denotes that their results may influence the choice of repair method when surgically treating Achilles tendon ruptures. Similarly, we believe that our results may be influential when choosing a repair method, but we cannot provide proof that the increased strength of repair is necessary for an acceptable clinical outcome. In addition, the questions will remain: Does the application of the greater number of suture passes when using triple bundle technique produce more tissue injury and vascular constriction than the lesser number of passes when using the Krakow technique? If so, is the additional injury worth the benefit of increased tensile strength? However, provided there is no disadvantage to the stronger triple bundle technique, then clearly patients with Achilles tendon ruptures would benefit from the strongest repair method.
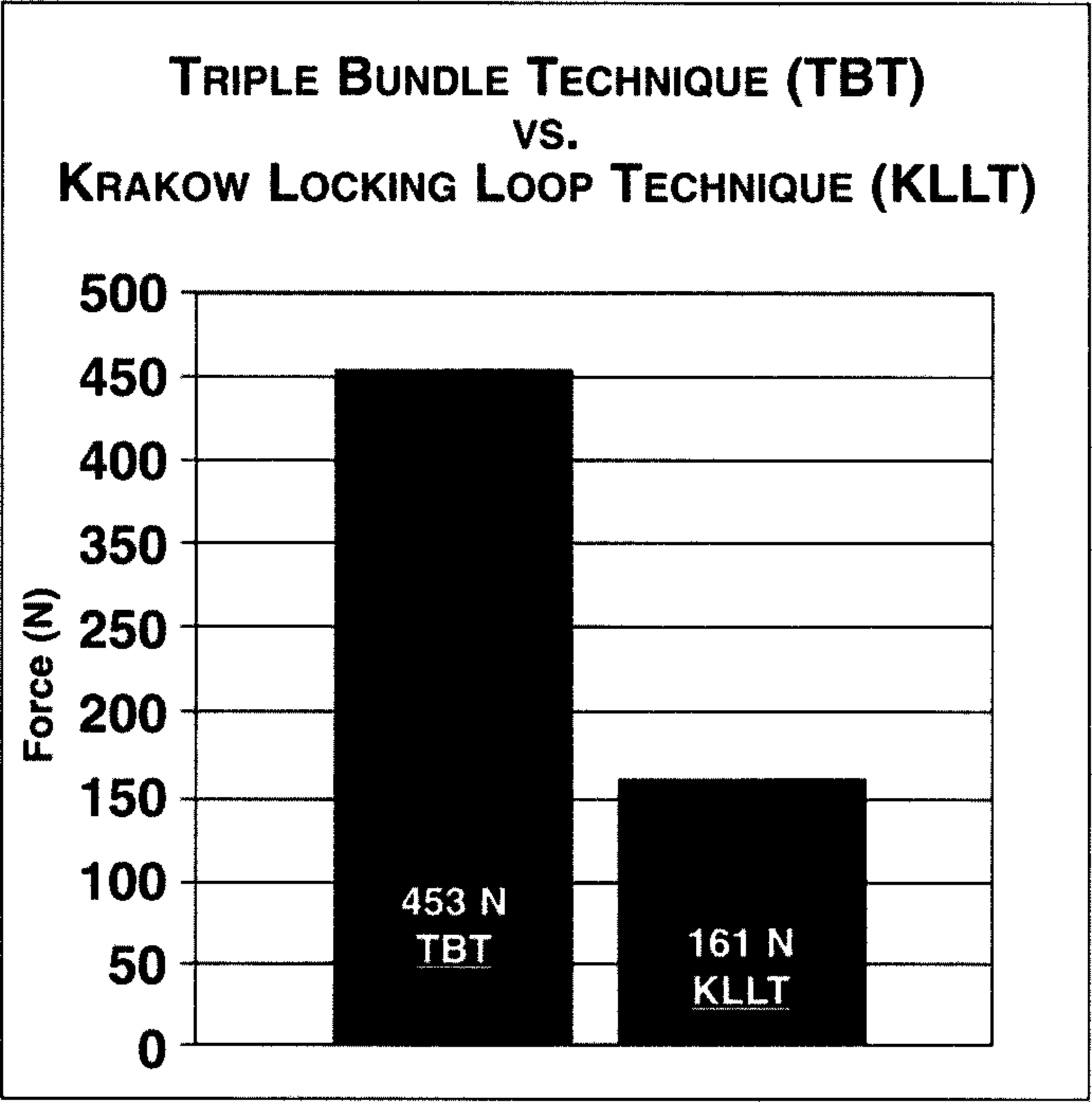
Graph representing the mean load to failure of group 1 (triple bundle technique: 453 N, SD = 53.9 N) and group 2 (Krakow locking loop technique: 161 N, SD = 31.1 N).
In 1991 Mortensen and Saether reported a biomechanical comparison of their continuous six strand suture (CSSS) technique to the Mason (a grasping-type repair similar to the Kessler) and Bunnell. 6 They found that both the Mason and Bunnell techniques ruptured at a tension of 20 to 110 N, whereas the CSSS technique ruptured at 130 to 290 N. However, as noted by Watson et al., 12 Mortenson and Saether did not report specifics regarding the median or mean load to failure or how many ruptures occurred at high or low values. 6 Furthermore, in contrast to the present study and the study by Watson et al., Mortenson and Saether did not use a testing machine. They applied hanging weights which they increased by 5 N every 30 seconds until failure. Their method, although equivalent in terms of actual load application, is inferior in terms of its inability to apply precise rates of loading.
A criticism against our study protocol is that our simulated rupture, by means of a transverse cut with a scalpel, does not reproduce the characteristic frayed “mop end” appearance of a clinical rupture. However, it would be difficult to reproduce a frayed rupture without causing increased randomization error. The triple bundle technique was specifically designed for repairing ruptures with frayed ends, whereas a transverse cut is the ideal rupture to repair with the Krakow locking loop technique. This suggests that the difference in strength between the two methods would be even more in favor of the triple bundle technique when a clinical rupture (frayed ends) is surgically repaired.
CONCLUSION
These results show that Achilles tendons that are surgically repaired using the triple bundle technique are significantly stronger in tension than those that are surgically repaired using the Krakow locking loop technique.