
Abstract
The anterior drawer test is commonly used in the diagnosis of ankle joint mechanical instability. However, the effect of axial load on the anterior drawer test has not been examined in vivo. The purpose of the study was to assess the effect of axial load on passive anterior instability, and on the diagnostic measurement of the anterior drawer instability of the ankle joint complex. A total of 21 subjects with various degrees of ankle sprains were tested on a device that could continuously record applied anterior force and the resultant displacement of the rear-foot. Anterior drawer flexibility of the ankle joint complex in a neutral dorsi/plantar flexion position was quantified on both feet for all subjects without and with an axial load (385 N). Flexibility of the ankle joint complex in anterior drawer was defined as the slope of a linear load-displacement curve (which fitted test data with high correlation coefficients (r>0.991)). With axial load, anterior drawer flexibility was significantly reduced by 28.8% compared to that without axial load. The difference in anterior drawer flexibility between injured and intact ankles significantly decreased with axial load. An axial load increased the stability of ankle joint complex. However, axial load reduced the sensitivity of anterior drawer test to mechanical instability of the ankle joint complex.
INTRODUCTION
The ankle anterior drawer test is the most commonly used technique to diagnose acute damage or permanent deficit to the anterior talofibular ligament (ATFL).2,9 This technique has demonstrated its validity in the clinical examination of ankle joint instability.9,10,13,19,20 However, those clinical studies have been criticized because the anterior drawer test was conducted under non-weight bearing conditions.6,8 The optimal conditions to perform the diagnostic test are unknown.
There have been few reported in vitro studies that have evaluated the effect of axial load on the stability of ankle joint complex8,16,23,24 to simulate weight bearing. McCullough and Burge 16 studied the range of rotation of the talus in the cadaver ankles under conditions that simulated normal weight bearing. It was found that rotation was load-dependent in both the intact ankle and following dissection of the lateral collateral ligaments. The similar findings were reported by Fraser and Ahmed 8 in which they measured passive rotational motions of ankle joint while applying an increasing axial load of up to 666 N. The rotational motion decreased with increasing axial load. Stormont et al. 24 conducted a study on twenty-one cadaver specimens with sequential dissection of ligaments. They tested the specimen in adduction/abduction and inversion/eversion under no axial load and with 670 N axial load. They found that with axial load, the articulate surface provided for 30% and 100% of constraint resistance in adduction/abduction and inversion/eversion, respectively, but it was insignificant in restraining those motions without axial load. In vitro studies have consistently demonstrated the importance of axial load in stabilizing the ankle joint complex. However, there have been no reported in vivo studies on human subjects to demonstrate the difference in anterior drawer stability of the ankle joint complex due to axial load.
For patients with unilateral ankle injuries, the difference in joint flexibility between the intact and injured ankles is a reliable measure for joint mechanical instability.1,12 However, it is unknown under what condition (with or without axial load) a clinical measurement would most likely find a difference in flexibility between the two ankles. One would like to know under which condition, with or without axial load, the anterior drawer test would reveal a larger difference in ankle flexibility between the injured and the intact ankles of the patients with unilateral ankle sprain. To determine this one can compare the difference in joint flexibility between the injured and the intact ankles of the same subject under two conditions. If the difference in joint flexibility decreases with the application of axial load for a reasonable number of subjects with various levels of ankle sprains, the axial load then can be considered to reduce the sensitivity of anterior drawer test to the ankle instability.
The objectives of this study were to quantify the effect of axial load on anterior drawer flexibility of ankle joint complex in uninjured subjects and subjects with various levels of ankle sprains. By comparing the difference of ankle flexibility between the injured and the intact ankles in subjects with unilateral ankle sprains, we could determine whether the axial load would reduce the sensitivity of the anterior drawer test.
METHODS
A total of 21 individuals (11 males, 10 females) volunteered for the study. The subjects had mean age of 28 years (19–43), average height of 175 cm (162–190) and body weight of 70.6 kg (49–88). Before testing, each subject was informed about the procedure and filled out a questionnaire. The questionnaires revealed various ankle injury levels. A history of Grade III sprains was reported by 7 subjects, and Grade I and/or II sprains in the rest of subjects except two subjects who reported no injury history of their ankles. Among those with history of ankle sprains, a total of 14 subjects had unilateral ankle injuries. The current symptoms were reported to be severe by 6 subjects, and mild or none by the rest of subjects. The informed consent procedure was approved by the university ethics committee.
In vivo measurement of flexibility of the ankle joint complex was conducted on an apparatus which was originally developed for in vivo measurement of the range of foot motion 17 (Figure 1). This construction consisted of three frames. An outer frame included a seat for the subject and the mounting support for a leg fixator and a foot plate. The leg fixator could slide up and down along a vertical axis fixed on the outer frame. The foot plate was used to fix the subject's foot. The foot plate was designed to move in three rotations (dorsi/plantar flexion (DP), eversion/inversion (EI), and adduction/abduction (AA)) and two translations (anterior/posterior translation (AP), and medial/lateral translation (ML)) relative to the outer frame, corresponding to the five degree of freedom motions of the ankle joint complex. In this study, however, all three rotational motions were constrained by a locking mechanism on each rotational joint in order to eliminate the effect of coupled rotations on the measured anterior translation. Axial load was applied by putting the weights on the top of leg fixator. A force transducer (precision tensile load cell, Model LCCA-100, accuracy 0.037% in full scale, range 454 N, OMEGA Engineering, Inc., Stanford, CT, USA) was mounted on a cable which was used to pull the foot plate along an anterior direction. A linear motion transducer (Displacement transducer, PT101-0030-111-1110, accuracy 0.1% in full scale, range 76 cm, Intertechnology, Inc., Ontario, Canada) was mounted on the posterior side of the outer frame while its sliding string was fixed onto the foot plate. During anterior drawer testing, the signals from both force transducer and linear motion transducer were converted to digital signals at a sampling frequency of 30 Hz and stored in the hard disc of a personal computer.
The injured side, grade of sprain, anterior drawer flexibility on both ankles with and without axial load, and the percentage difference (PD) in joint flexibility between the injured and the intact ankles for 14 subjects with unilateral ankle sprains. The definition of PD is provided in the text.
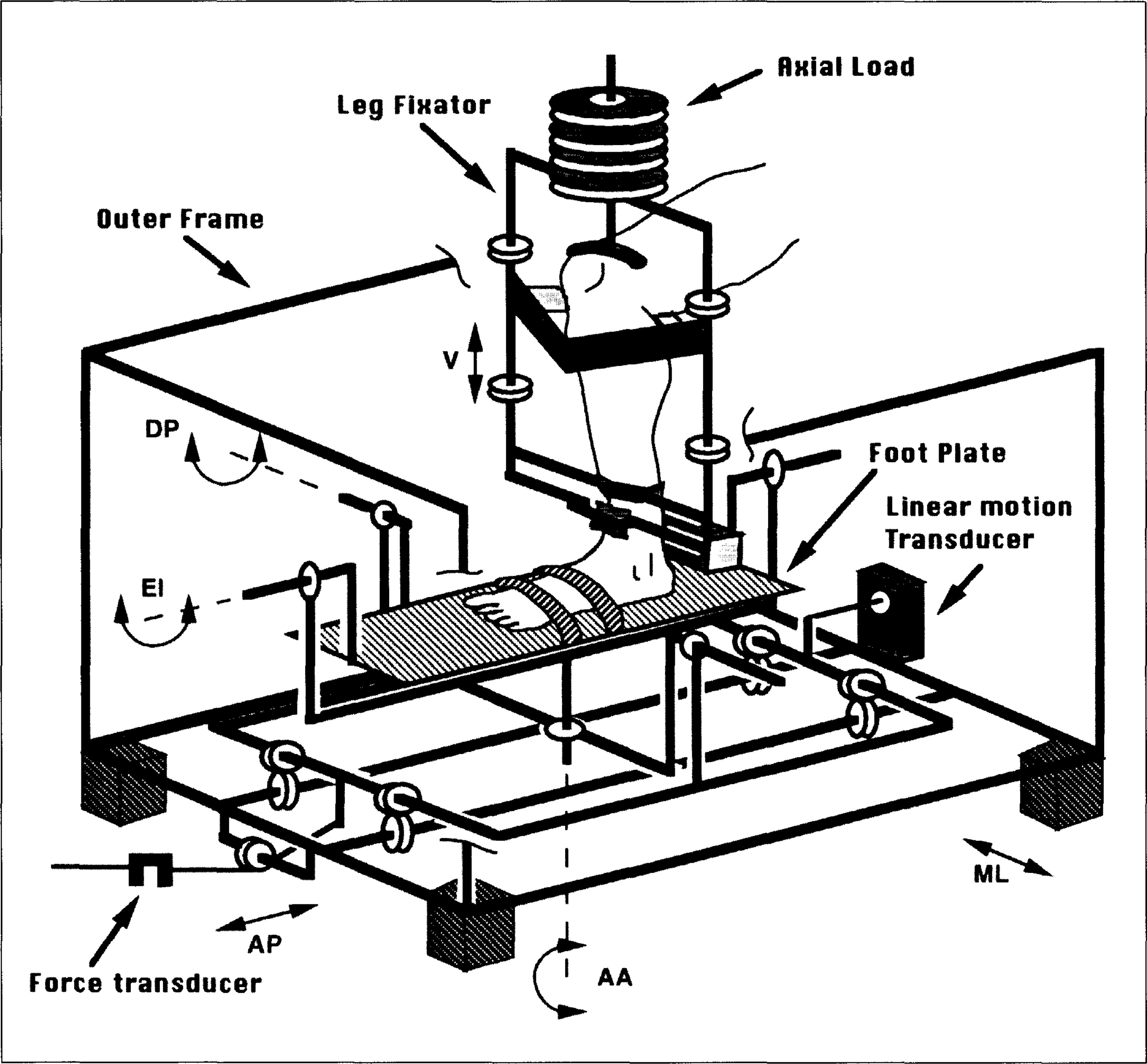
Illustration of the ankle joint flexibility measurement apparatus. The leg is affixed by clamps and straps onto the leg fixator. The foot is affixed to the foot plate with straps. Anterior drawer force is transformed to the heel by a metal piece with padding fixed on foot plate.
During the anterior drawer test, the subject sat on a seat with his/her knee at 90° of flexion, with the lower leg in a vertical position. The subject was instructed to maintain a relaxed state of his/her leg muscles throughout whole testing. The plantar surface of the foot on the foot plate was in the horizontal plane. The heel firmly contacted a small platform on the posterior side of the foot plate which was used to push the heel in anterior direction. The leg was fixed by a V-clamp and Velcro strap around the knee. Two V-clamps on either side of the lower leg and an additional steel bar on the front just above the malleoli were used to fix the lower leg. The bare foot was fastened by means of Velcro straps over the midtarsal and the metatarsal bones to the foot plate. The ankle joint was positioned in its neutral dorsi/plantar flexion position by locking the foot plate in a perpendicular position relative to the leg. Stiehl et al. 23 found that ankle flexion (10° dorsiflexion to 15° plantarflexion) did not play a significant role in determining anterior drawer stability, and therefore, we chose to measure joint flexibility in the neutral position only. Anterior force was applied manually through a cable connected to the foot plate, while the latter pushed the heel forward. The maximum value of applied anterior drawer force was approximately 140 N, and was controlled by the operator unless that the subject would feel any discomfort or pain. The loading rate was controlled manually by the operator to be about 24 N/s. A real-time display of the force data helped the operator in controlling the magnitude and the rate of applied force. At first, the loading and unloading was repeated five times on the right ankle without axial load. Subsequently, an axial load of 385 N was then applied on the top of leg fixator frame and the same test was repeated. Since the axial load was applied on the knee joint at 90° of flexion, only about a half of averaged body weight (385 N) was applied in order to avoid the possible discomfort on subject. The same procedure was then repeated on the left ankle.
The first loading-unloading circle on each test was excluded from data analysis, since it functioned as a pre-conditioning on the joint (Figure 2). The loading portion of the load-displacement data from rest of four repeated measurements showed high consistency and linearity. A straight line was used to fit the loading portion of the load-displacement data. The slope of the line was defined as the flexibility of the ankle joint complex. A paired t-test was conducted on the mean values of flexibility of all ankles tested to compare the difference between the 385 N axial load condition and the no axial load condition.
For 14 subjects with unilateral ankle sprains, the percentage difference (PD), defined as percentage ratio of the difference in flexibility between the injured and the intact ankles divided by the value of flexibility of the intact ankle, was calculated to examine the change of joint flexibility due to ankle injury. To further determine whether or not two ankles of the same subject become more alike in their flexibility under axial load, differences in flexibility between the involved and the intact ankles of the 14 subjects were compared in the following manner. The more-flexible minus less-flexible ankle flexibility of each subject was first calculated for the no axial load condition. The same side-to-side difference in flexibility was then calculated for the axial load condition. A paired t-test was used to determine significant level of the difference in flexibility between two axial load conditions.
RESULTS
The significance level of data fit on loading portion of load-displacement curve was determined by a Fisher test. The linear correlation between applied anterior force and resulted displacement of ankle joint complex was highly significant for each test (Figure 2). The correlation coefficients (r) ranged from 0.970 to 0.999. For tests conducted without axial load, the mean correlation coefficients were 0.992 (SD, 0.0043) for all ankles tested. With axial load, the corresponding mean correlation coefficients were 0.995 (SD, 0.0053).
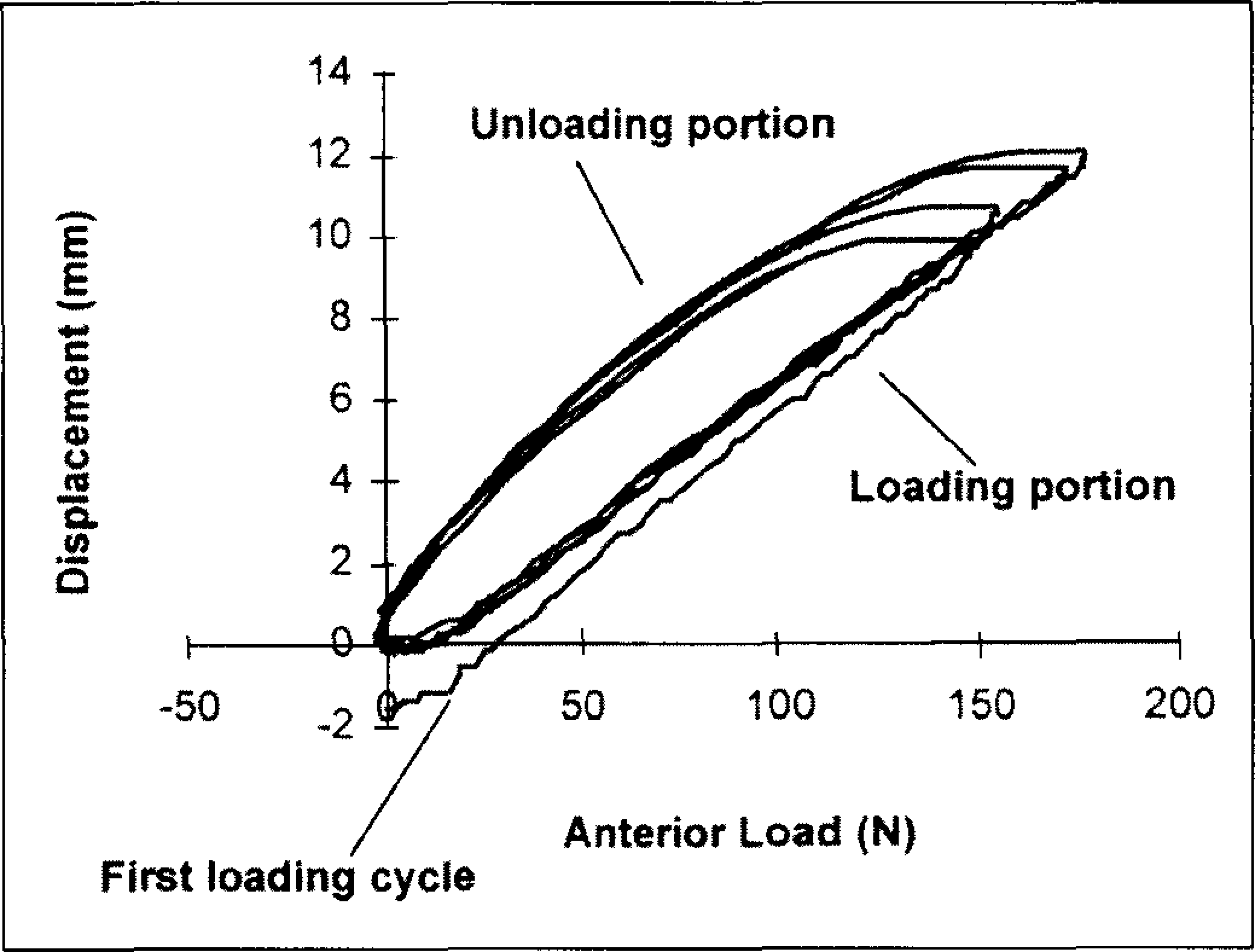
Raw data of measured load-displacement curve of ankle joint complex, showing loading and unloading portions. The first loading cycle was excluded from data analysis since it functioned as a preconditioner.
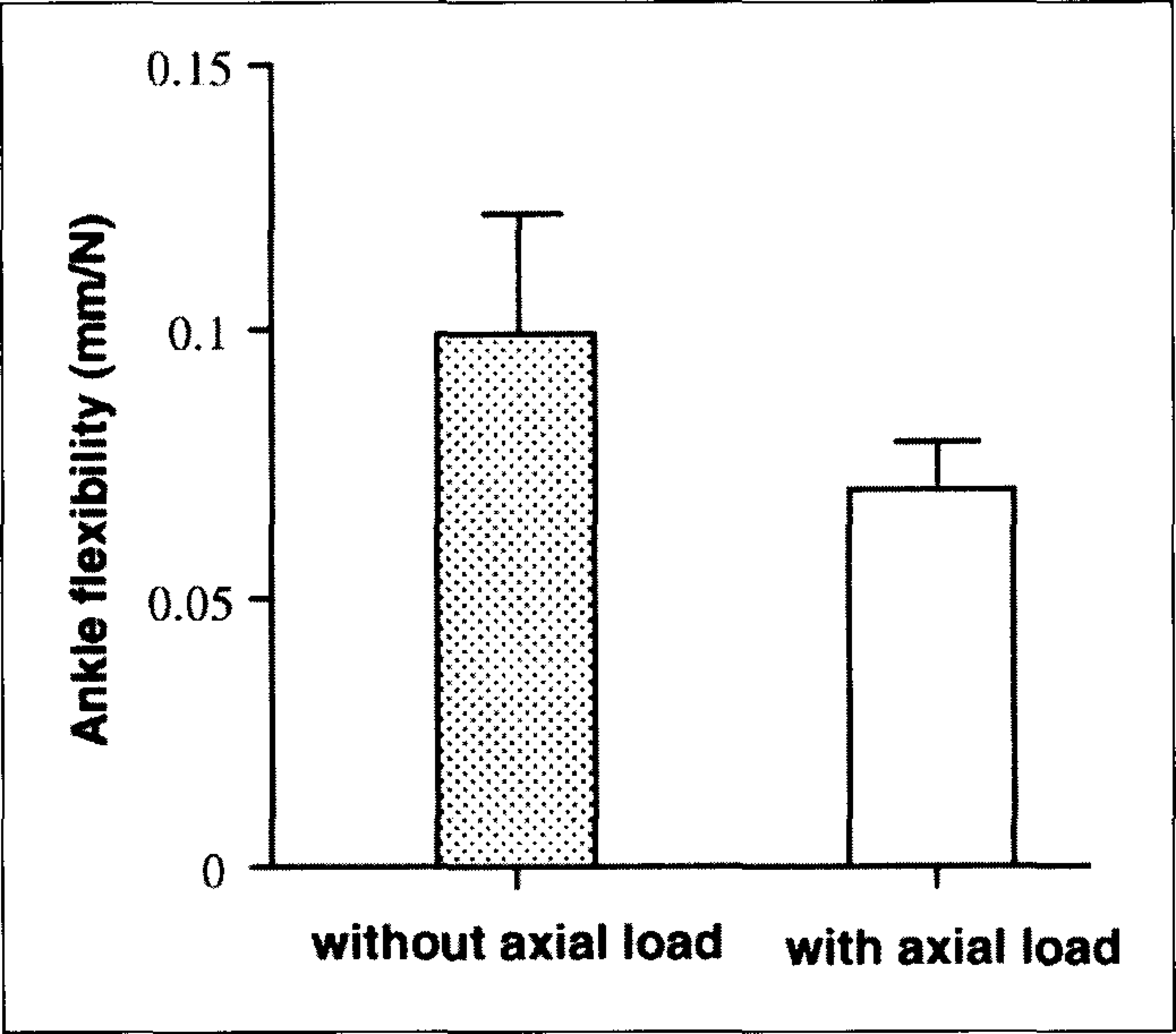
Flexibility value (mean and SD) for all ankles tested. The change in ankle flexibility with applied axial load was highly significant (P<0.0001).
The effect of axial load on anterior drawer flexibility of the ankle joint complex was significant (P<0.0001) (Figure 3). Comparing ankle flexibility without axial load to that with axial load, the mean flexibility (mm/N) decreased from 0.097 (SD, 0.023) to 0.069 (SD, 0.011) for all ankles tested. The average difference in anterior drawer flexibility was 28.8% after the application of axial load.
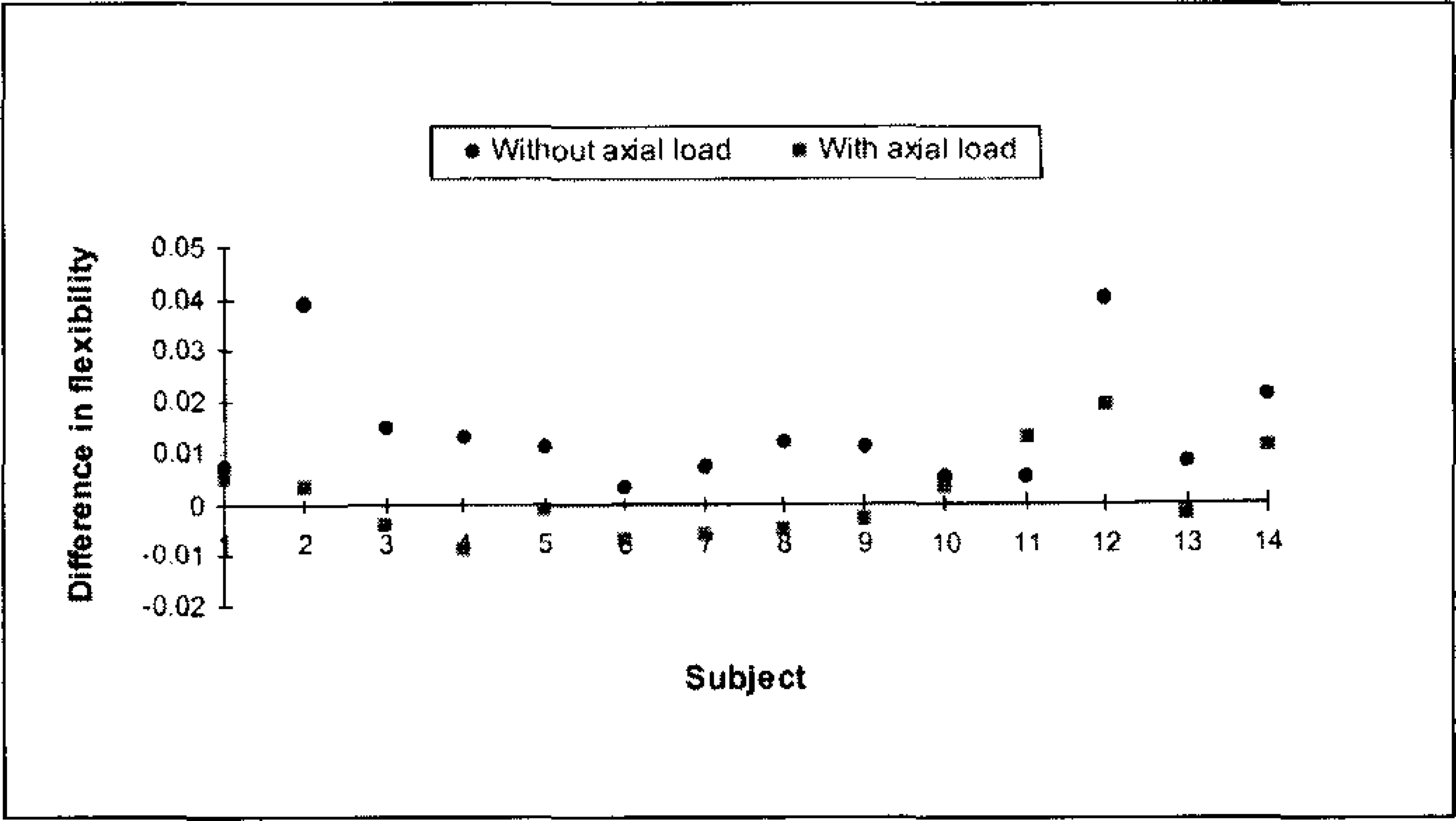
The more-flexible minus less-flexible ankle flexibility of each subject without axial load is compared to the same side-to-side difference in flexibility with axial load. The difference between two conditions is statistically significant (P<0.01).
The percentage difference (PD) in anterior drawer flexibility between the injured and the intact ankle joint complexes showed a wide range of variations among the 14 subjects with unilateral ankle sprains (Table 1). The PD ranged from −34.5 to +35.4 without axial load and from −19.4 to +17.9 with axial load. Such scattered distribution of the PD led to a mean value of 0.1 for the no axial load condition and −4.1 for the axial condition.
The difference in flexibility between more-flexible and less-flexible ankles in the same subject decreased significantly (P<0.01) with application of the axial load (Figure 4). If one were to inspect the absolute differences between the two sides, there was a significant reduction (P<0.02) in the flexibility with axial load as well.
DISCUSSION
It is commonly assumed that axial load increases the stability of the ankle joint complex in vivo, but the assumption has not been systematically examined. Cadaver studies have consistently shown that the increase in the axial load led to the decrease of the motion of the ankle joint. Stiehl and coworkers 23 applied a force of 150 N along the longitudinal axis of the foot of a cadaver specimen. The relative motion between tibia and foot was measured under two axial loading conditions of 150 N and 700 N. The increased axial load markedly reduced the motion of joint. Similar findings have been reported in the cadaver studies in the inversion/eversion and internal/external motions of the ankle joint complex. 8 The results presented in this in vivo study showed decreased flexibility of the ankle joint complex in anterior drawer motion with applied axial load. It supports the hypothesis that ankle instability may occur during loading and unloading but not once the ankle is fully loaded. 24
In this study, only two of the 14 subjects showed a PD value more than +17, which might be considered to be clinically significant. It indicated that about 14% of the involved ankles tested in this study might have passive mechanical instability. This ratio fell within the range of the ratio of passive mechanical instability after ankle sprain reported in the literature (2.5% to 45%) by various clinical studies.3,14,22 This in vivo study, however, showed a wide distribution of differences in flexibility between the ankles with history of sprains and their contralateral normal sides (Table 1). This finding did not agree with past in vitro studies that showed systematically the increased flexibility or range of motion of the ankle joint after sectioning the lateral collateral ligaments.4,15,21,26 The apparent contradiction between the current in vivo studies and the past in vitro studies may be due to ligamentous healing response that occurs only in the in vivo situation. Further, the results of the current study showed decreased joint flexibility in some ankles with history of ankle sprains. This result could not be directly compared to past clinical studies since those studies only reported the ratio of positive sign of passive mechanical instability without quantitative measurement of the flexibility. A significantly decreased flexibility (PD < −15) might be the results of massive scar tissue generated during healing of the ligaments.7,27 From the clinical standpoint, an ankle with abnormally reduced flexibility may require treatment in order to regain normal range of joint motion.
The differences in flexibility between the ankles with previous sprains and their contralateral intact sides were shown to decrease with application of the axial load during anterior drawer test. In both with and without axial load conditions, the differences in flexibility between the injured ankle and the contralateral normal side were positive in some subjects while negative in the other subjects.
It appears that the anterior drawer test is best conducted without axial load for the purpose of determining the change of joint flexibility. The mechanism responsible for increased instability by axial load has been suggested to be the results of increased joint congruity. 24 With axial load, the articulated structures of the ankle joint increased its role in constraining anterior motion of the joint while the restraint from ligaments reduced due to ligament relaxation. Therefore, it does not seem surprising that both ankles in the same subject become similar in their flexibility under axial load even though one of them had a previous sprain.
Muscle contraction may reduce ankle flexibility. In physical examination or stress radiographic diagnosis, the end of the range of ankle joint motion was reached in anterior drawer test to insure the accuracy of the measurements. Therefore, a muscle guarding reaction was likely going to occur with unknown degree of contraction depending on the tested individual.11,19 In this study, the applied load was at a level that did not cause discomfort. Also, the subjects were requested to relax their leg muscles. The leg was supported in the test apparatus in a manner that leg muscle forces were not required to maintain the position. However, ankle muscle activation was not measured and can be a potential source of error.
One of the limitations of this study was that applied force was only in the anterior direction, not in both anterior and posterior directions. Therefore, the resultant load-displacement curve did not include a region of “neutral zone”, 18 in which a relatively large displacement occurs with a small magnitude of applied load. We could not determine the effect of axial load on the neutral zone parameters.
Another limitation of the present study is that the results of joint flexibility include movement of the calcaneus with respect to the tibia, the deformation of the soft tissue of the foot and the soft padding on the surface of the fixation device. Those deformations increased measured flexibility compared to the true flexibility within the talocrural and subtalar joints. This is obvious when comparing the results of this study with results of previous studies. 25 However, all the tests were conducted under the same fixation conditions. Thus, the systematic errors in joint flexibility would not influence the comparison of joint flexibility with and without axial load.
Axial load has been demonstrated in this in vivo study to increase significantly the mechanical stability of the angle joint complex. The results of this study also implied that axial load reduced the sensitivity of anterior drawer test to mechanical instability of the ankle joint complex. Therefore, it is recommended that the ankle anterior drawer test be conducted without axial load for the purpose of diagnosis of mechanical instability.