
Abstract
Purpose
Longitudinal split tears of the peroneus brevis tendon have been increasingly reported as a source of lateral ankle pain and disability. MR imaging is useful in identifying the appearance of longitudinal split tears of the peroneus brevis tendon to differentiate this entity from other causes of chronic lateral ankle pain. We observed variations in anatomy associated with these tears.
MATERIALS AND METHODS
Twenty-two patients (eleven males, eleven females) were identified as having longitudinal split tears of the peroneus brevis tendon. These cases were reviewed retrospectively to evaluate for the following: shape of the peroneus brevis tendon, high signal in the peroneus brevis tendon, tendon subluxation, appearance of the superior peroneal retinaculum, presence of osseous changes in the ankle, lateral ankle ligaments, presence of a bony fibular spur, flattening of the peroneal groove of the fibula and presence of a peroneus quartus.
A control group consisted of twenty ankles imaged for reasons other than lateral ankle pain. The same structures were assessed in this group. A Fisher's exact P-value was used to determine the significance of each finding in the two groups.
RESULTS
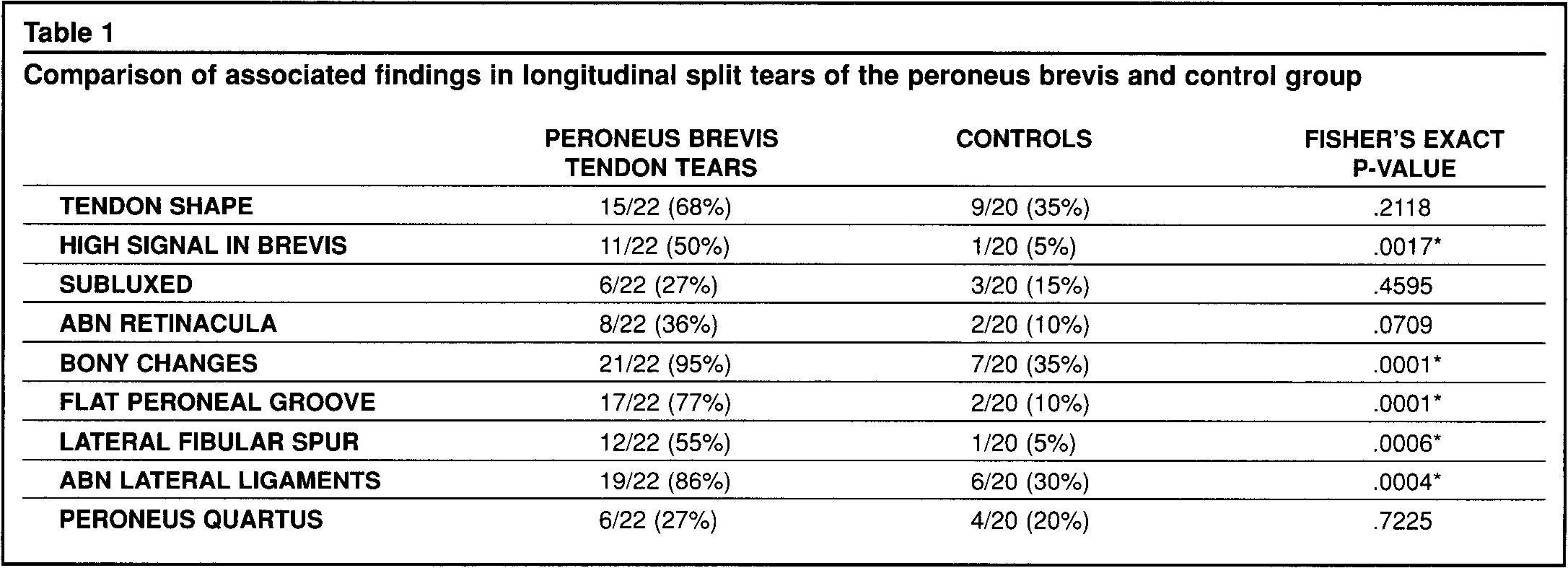
Statistically significant associated findings were chevron shaped tendon (p = .0001), high signal in the peroneus brevis (p = .0017), bony changes (p = .0001), flat peroneal groove (p = .0001), abnormal lateral ligaments (p = .0004), and lateral fibular spur (p = .0006).
Conclusions
MR imaging is useful in differentiating longitudinal split tears of the peroneus brevis tendon from other lateral ankle disorders. It can show the extent of the abnormality in the tendon and the associated findings of soft tissue and/or bone variations which must be addressed at the time of surgery.
INTRODUCTION
Chronic pain and disability following ankle injuries are common, and the exact etiology can be difficult to diagnose. The differential diagnosis of chronic lateral ankle pain includes lateral ligament disruption, sinus tarsi syndrome, osteochondritis dissecans, fractures, osteoarthritis, loose bodies, and anterolateral impingement syndrome. Peroneal tendon injuries, once considered uncommon, have been reported to be a frequent source of chronic lateral ankle pain. 1,4,9 MR imaging can play a valuable role in evaluating chronic lateral ankle pain by demonstrating the etiology and thereby helping the surgeon in planning the appropriate treatment. This study was undertaken to evaluate the appearance of longitudinal split tears of the peroneus brevis on MR imaging, and to observe the variations in anatomy associated with these tears.
MATERIALS AND METHODS
Retrospectively we studied all ankle MR exams performed at two institutions between August 1992 and April 1997 which were interpreted as having a longitudinal split tear of the peroneus brevis. The study included 22 patients, eleven males and eleven females. The ages ranged from 13–76 years (average 39.7 years). Imaging was performed using a 1.5T magnet (GE Signa, Milwaukee, WI). An extremity coil was used in all cases. A variety of sequences were used which included spin echo T1 (TR/TE 600/20), proton density (TR/TE 2000/20), T2 (TR/TE 2000/70) as well as fast spin echo with fat suppression (TR/TE 3500/105 effective) and gradient echo (TR/TE 600/15 flip angle 30∞) imaging. Imaging planes included axial, sagittal and coronal. All three planes were not obtained in every patient. Each study was evaluated to determine the following: shape of the peroneus brevis tendon, high signal in the peroneus brevis tendon, tendon subluxation, appearance of the superior retinaculum, presence of bony changes in the ankle, lateral ankle ligaments, presence of a fibrocartilagenous or bony fibular spur, flattening of the peroneal groove of the fibula, and presence of a peroneus quartus muscle.
A control group consisted of twenty ankles imaged for reasons other than lateral ankle pain. The same structures were assessed in this group. A Fisher's exact P-value was used to determine the significance of each finding in the two groups. A P-value of less than 0.05 was considered statistically significant.
No patients in our series or in the control group had rheumatoid arthritis, seronegative spondyloarthropathies, gout, steroid injections, other connective tissue disorders or infections that would increase the risk of a tendon degeneration predisposing the patients to longitudinal splits.
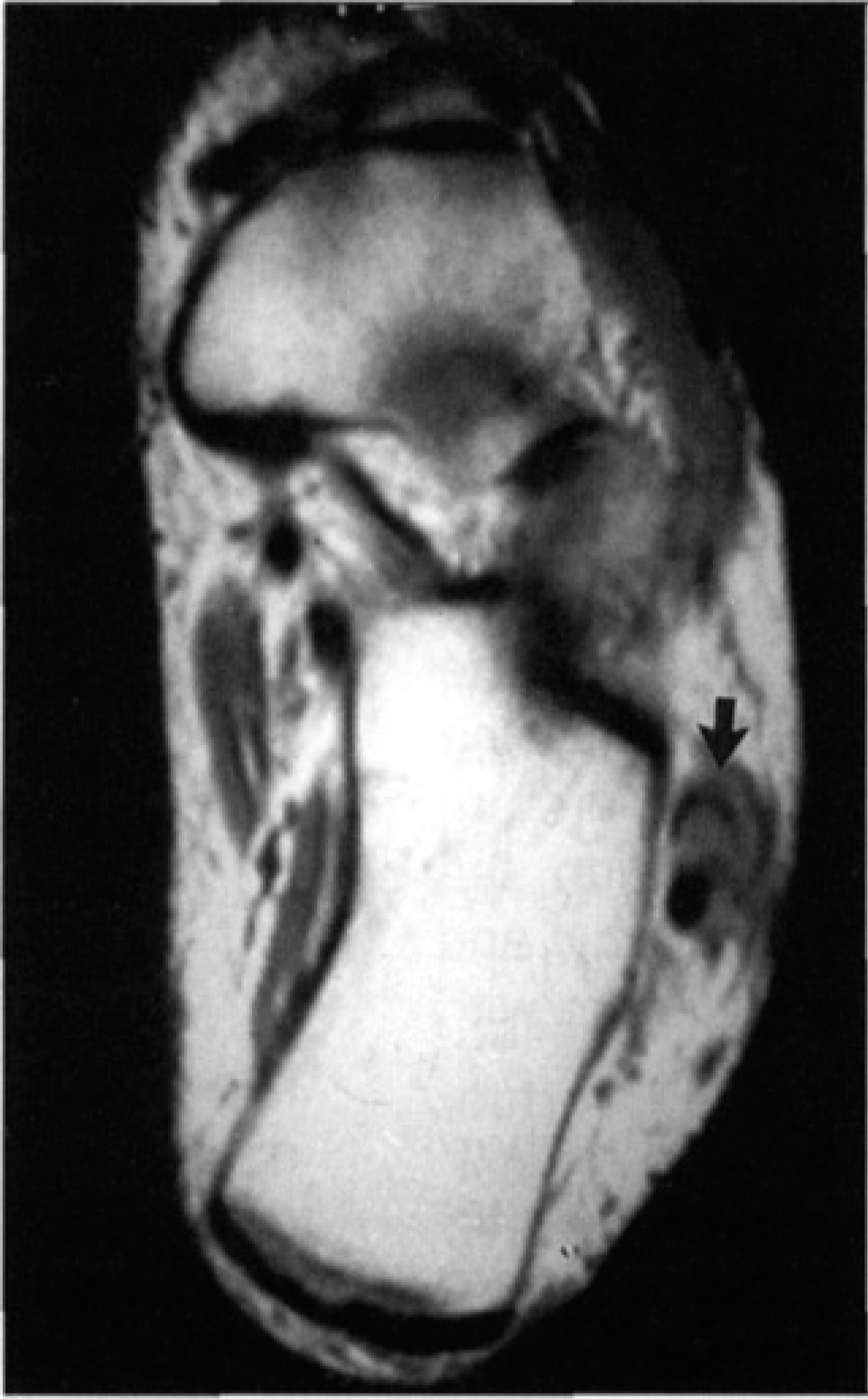
Axial proton density image (TR/TE 2000/20) demonstrates a chevron shape of the peroneus brevis (arrow).

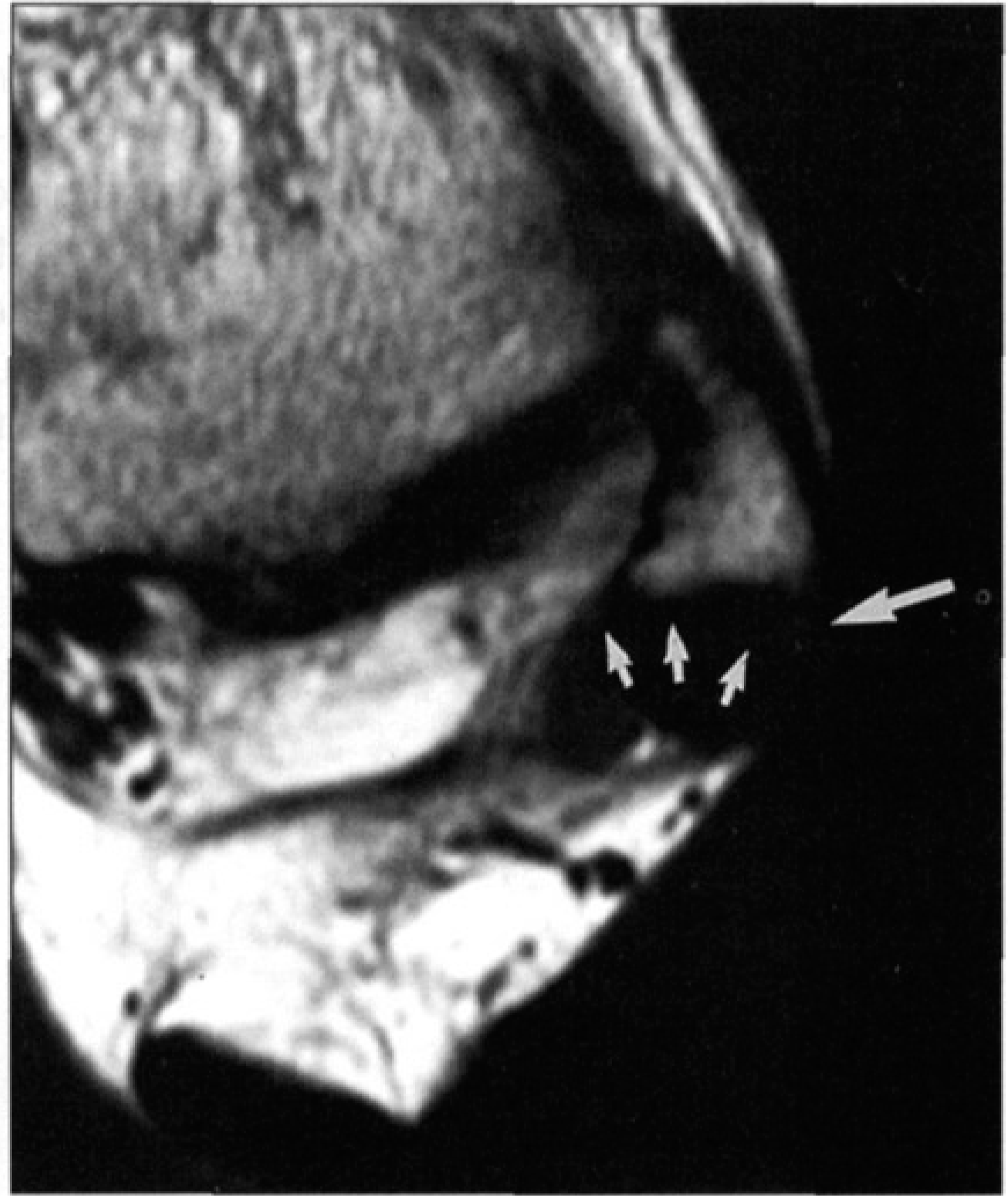
The axial T2-weighted image (2000/80) shows high signal in the peroneus brevis tendon (arrow).
RESULTS
All twenty-two patients in this study had a longitudinal split tear of the peroneus brevis located at the level of the peroneal groove with some proximal and distal extension. All patients had sustained an ankle inversion injury. The tendon demonstrated a chevron shape on axial imaging in fifteen patients (68%) (Fig. 1A, 2) (Table). High signal was identified in the peroneus brevis in 11/22 (50%) on the T2 weighted images (Fig. 1B, 3A). Subluxation of the peroneus tendons was noted in 6/22 (27%), two of the subluxations were lateral and four were medial. The superior retinaculum was abnormal in appearance (either torn or thickened) in 8/22 (36%) (Fig. 2, 3B). Bone changes were identified in 21/22 (95%). These included a flattened peroneal groove in 17/22 (77%) (Fig 2, 3B), osteochondritis dissecans of the talus in 4/22 (18%), fracture, contusion or degenerative changes of the tibiotalar joint in 3/22 (14%). A lateral fibular spur was present in 12/22 (55%) (Fig. 2, 3B). The soft tissue changes seen on MR examination included abnormal anterior talo-fibular ligament 19/22 (86%) (torn in 10/22 (45%); or thickened in 9/22 (41%)). A peroneus quartus muscle was identified in 6/22 (27%) (Fig. 2, 3B).
Within the control group of twenty patients, 11 (55%) patients had a round peroneal brevis tendon while 9/20 (45%) had a flat tendon. Nineteen of the 20 (95%) patients demonstrated no abnormal signal in the peroneal tendon. Three patients showed subluxation of the tendons (2 medially and one laterally). Osseous changes were identified in the talus in 7/20 (35%). These changes included a contusion in the talus, a fracture of the medial process of the talus, OCD and degenerative changes in the tibiotalar or talonavicular joint. The lateral ligaments were found to have abnormalities in 6 of the 20 patients. The anterior tibiofibular ligament was torn in 3 of the 6 patients and the anterior talofibular ligament was torn in 5 of the 6 patients. One of the 20 (5%) patients demonstrated a fibular spur. Two of the 20 (10%) patients showed a flattened peroneal groove. Four of the 20 (20%) patients demonstrated a peroneus quartus.
DISCUSSION
The peroneal tendons are uniquely prone to stress. Longitudinal split tears of the peroneus brevis occur in a segment of the tendon that bends around the lateral malleolus during tendon excursion. A proposed mechanism of tearing may be as a result of the inner side of the tendon being forced against the bone as it passes around the lateral malleolus. 8 In addition, the peroneus brevis tendon bears compressive forces produced during contraction of the peroneus longus muscle. The constant location of peroneus brevis split tears at the posterior edge of the fibula indicates that the tears are most likely due to mechanical trauma. 6 In addition, the findings of peroneus brevis tears in the elderly and young, athletic, healthy population are consistent with this mechanism. 2
Another reported mechanism of injury is that the peroneus brevis tendon subluxes and is split by the posterior margin of the lateral malleolus under the compression of the peroneus longus tendon. 8 Once a defect is created, motion of the ankle allows the peroneus longus tendon to move into the longitudinal cleft in the brevis tendon. This prevents healing of the defect and ultimately results in a chronic tenosynovitis with pain, swelling and limitation of motion. It is noteworthy that the vascular supply to the peroneus brevis is attenuated at the level of the peroneal groove within the fibula. 7 Anatomic factors, such as a shallow fibular groove or the presence of an anomalous low-lying peroneus brevis muscle belly or peroneus quartus tendon, are reported to play a role in this mechanism by interfering with the competence of the superior peroneal retinaculum. 3
The muscular variants such as the anomalous trifurcation or bifurcation of the tendon, low-lying peroneus brevis muscle belly, or a muscles peroneus quartus can cause crowding of the peroneus tendons in the region of the fibular groove. The superior retinaculum would be stretched and predisposed to tearing. The relative risk of longitudinal split of the peroneus brevis is reportedly doubled in the presence of an anomalous peroneus quartus. 6
We found that it can occasionally be difficult to differentiate a low-lying peroneus brevis muscle from a peroneus quartus, a frequent variant (13–22%) of normal individuals. The peroneus quartus tendon is a separate, smaller tendon which is located both posterior and medial to the peroneus longus and brevis and is generally smaller than the longus and brevis tendons. The peroneus quartus should be distinguishable from a tendon split of the brevis on MR exam by its course on serial images and by its regular margin and round contour.
The peroneal tendons are best evaluated on the axial MR images with the foot in slight plantar flexion. The normal appearance of the peroneus brevis at the level of the peroneal groove on axial MR imaging may be round or flat. The axial images around the tip of the fibula should be closely scrutinized, as this is the usual level for tendon splits. 4,7,8 The peroneus brevis tendon should be uniformly low in signal on the T2WI. It is located slightly anterior or medial to the peroneus longus. 11
Anatomic variations of the appearance of the peroneus brevis tendon exist. They may occur in as many as 13% of tendons, and include an anomalous trifurcation of the tendon. 8 A traumatic longitudinal cleft in the peroneus brevis tendon at the level of the fibular malleolus may be difficult to differentiate from a bifurcated insertion of the peroneus brevis tendon. The latter is an anatomic variant, and reportedly a rare cause of peroneal tenosynovitis. 7,8
A longitudinal tendon split should be considered on MR imaging when the tendon has multiple tendon slips in the peroneal tunnel. This suggests a separation of tendon fibers. This appearance is more specific than severe flattening of the brevis which can be seen in asymptomatic patients. When torn, the tendon becomes chevron shaped and envelopes the longus tendon. 11 The two separate tendon portions of the brevis reunite below the longitudinal split.
Comparison of associated findings in longitudinal split tears of the peroneus brevis and control group
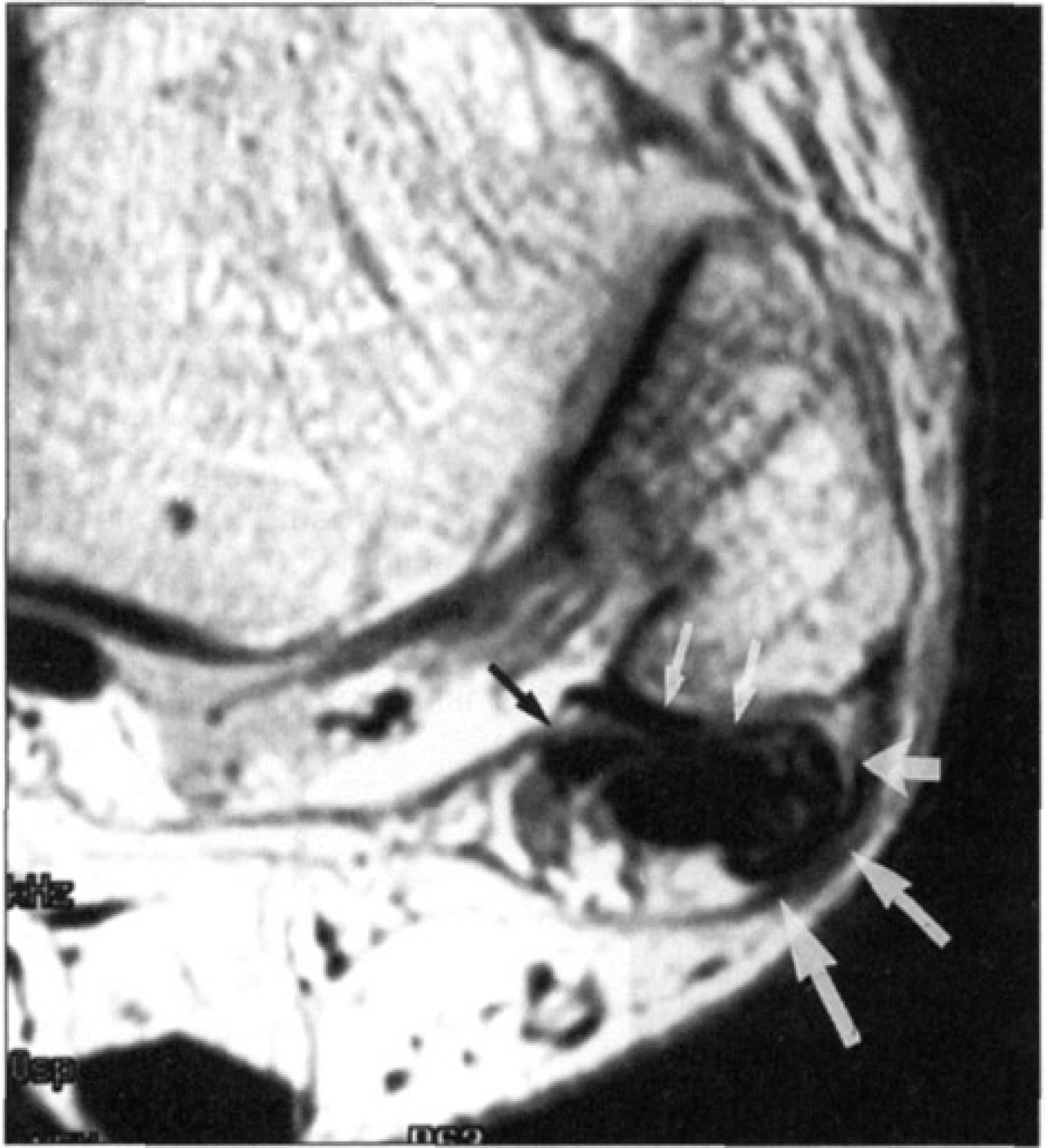
The axial proton density image (3000/20) shows a fibular spur (short white arrow), flattening of the peroneal groove (thin white arrows), thickening of the superficial retinaculum (long white arrows), flattening of the peroneus brevis, and a peroneus quartus (thin black arrow).
Occasionally, artifactual signal changes in the tendon can result in a chevron shape appearance of the brevis on T1 or proton density images. This is called the magic angle phenomenon and it occurs when the tendons change direction below the tip of the fibula (Fig 4). The magic angle phenomenon occurs in tissue which has parallel fibers, such as tendons and ligaments. These tissues demonstrate intermediate to high signal on MR images with a short TE (< 40 msec) when the tissue is aligned at or close to 55° to the bore of the magnet. 12 Evaluating the T2-weighted (TE > 40 msec) images helps to resolve this artifactual signal change. That is, if the signal or shape of the tendon remains abnormal on the T2-weighted image, the tendon is abnormal.
In our series, subluxation of the peroneal tendons was identified in 6/22 patients. Four of our cases demonstrated medial subluxation. In the literature to this date, medial subluxation has not been reported. When the peroneal tendons sublux, the usual situation is they will relocate lateral to the fibula. We had four patients whose tendons subluxed in a medial direction out of the fibular groove to rest medial to the normal location of the tendons within the fibular groove.
Treatment of longitudinal split tears of the peroneus brevis includes conservative management with antiinflammatory medication, orthotics, bracing and decreasing activity. If no improvement occurs then surgical intervention should be considered. Surgical options include primary repair of the split tendon, resection of the tendon, or tenodesis. Tendon grafts may also be used when necessary. At the time of surgery, associated conditions such as torn retinaculum, deepening of a shallow peroneal groove, resection of spurs and decompression of a peroneus quartus should be addressed.

Axial proton density image (2000/20) shows high signal in the peroneal tendon (arrow).
Axial T1-weighted image (600/13) reveals a fibular spur (white arrow), and peroneus brevis draped over the peroneus longus (short white arrows). Additionally, the peroneal groove is flat and the superficial retinaculum is torn.
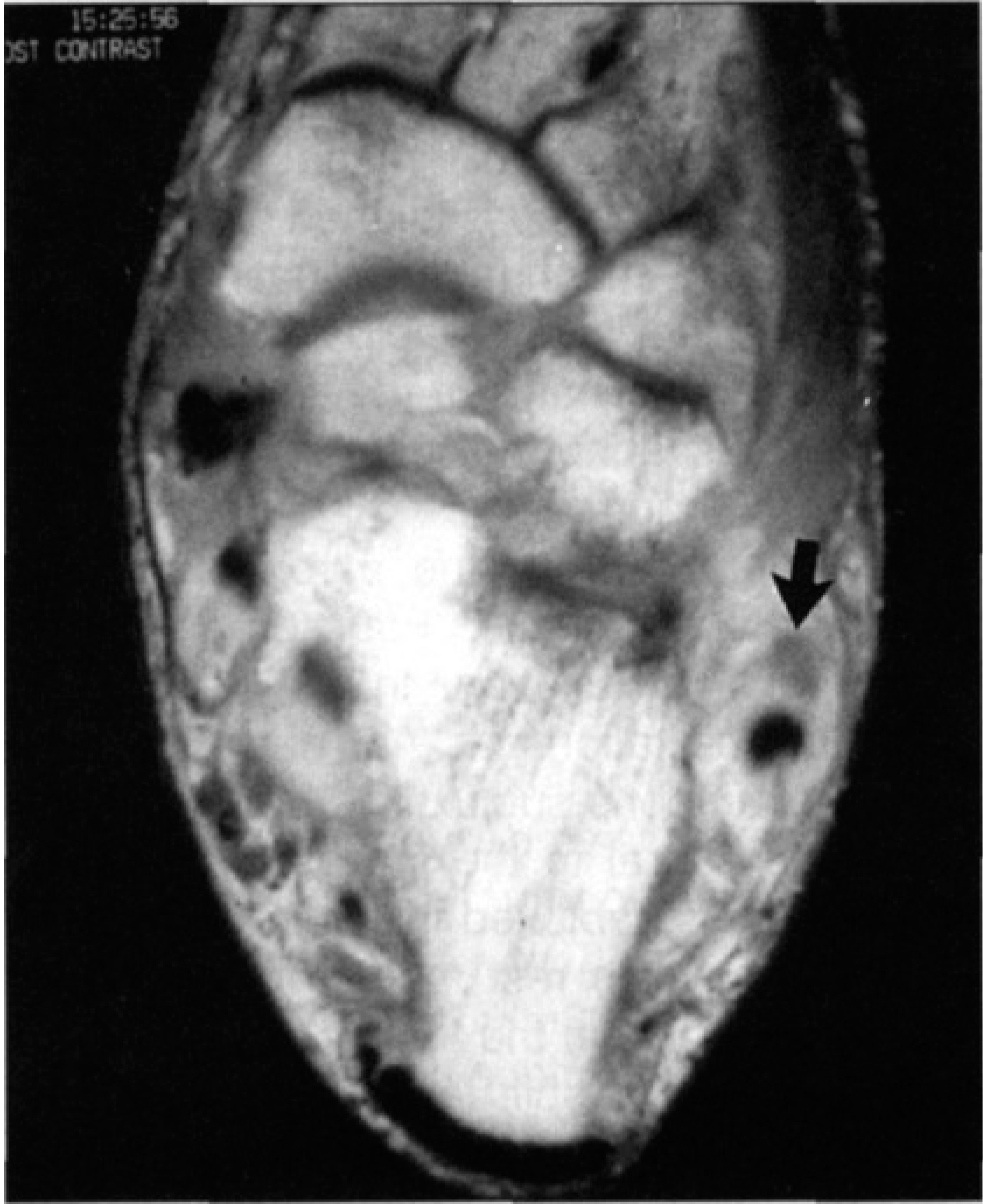
Axial T1-weighted image (600/13) shows a grey appearing peroneus brevis (black arrow). A tendon with myxoid degeneration or edema could have this appearance.

Axial T2-weighted image (2000/80) shows the tendon to be normal in signal. This is an effect of magic angle phenomenon.
The findings in this study associated with longitudinal split tears of the peroneus brevis which are statistically significant are a chevron shaped peroneus brevis, and high signal in the peroneus brevis on T2-weighted images, osseous changes, a flat peroneal groove, a lateral fibular spur, and abnormal lateral ligaments (Table). Flattening of the peroneus brevis, subluxation of the peroneal tendons, abnormal superior retinaculum, and presence of a peroneus quartus were not statistically significant associated findings.
CONCLUSION
Longitudinal split tears of the peroneus brevis tendon are uncommon, the possibility should be entertained in patients with chronic lateral ankle pain, swelling and instability, or suspected subtalar joint pathology. MR can show the extent of the abnormality and the additional findings of soft tissue and/or osseous abnormalities which must be addressed at the time of surgery.