
Abstract
Fifty-eight patients with 60 talar fractures were retrospectively reviewed. There were 39 men and 19 women. The age average was 32 (range, 14–74). Eighty six percent of the patients had multiple injuries. The most common mechanism of injury was a motor vehicle accident. Twenty-seven (45%) of the fractures were neck, 22 (36.7%) process, and 11 (18.3%) body. Forty-eight fractures had operative treatment and 12 had non-operative management. The average follow-up period was 30 months (range, 24–65). Thirty-two fractures (53.3%) developed subtalar arthritis. Two patients had subsequent subtalar fusion. Fifteen fractures (25%) developed ankle arthritis. None of these patients required ankle fusion. Fractures of the body of the talus were associated with the highest incidence of degenerative joint disease of both the subtalar and ankle joints. Ten fractures (16.6%) developed avascular necrosis (AVN), only one of which had subsequent slight collapse. Avascular necrosis occurred mostly after Hawkins Type 3 and 2 fractures of the talar neck. Three rating scores were used in this series to assess the outcome: the American Orthopedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Score, Maryland Foot Score, and Hawkins Evaluation Criteria. The outcome was different with every rating system. However, the outcome with AOFAS Ankle-Hindfoot Score and Hawkins Evaluation Criteria were almost equivalent. Assessment with the three rating scores showed that the process fractures had the best results followed by the neck and then the body fractures.
Keywords
INTRODUCTION
It has been concluded that good results of talar neck fractures depend on anatomical reduction and fixation. The importance of an active rehabilitation program has been emphasized.4,8,11,17 Hawkins (1970) 6 proposed a classification system for talar neck fractures. Canale and Kelly (1978) 1 modified the original Hawkin's classification with an additional type IV. They also described a radiographic view which better delineated the talar neck. Szyszkowitz et al (1985) 16 reviewed 85 talus fractures treated by open reduction and internal fixation and concluded that stable fixation by lag screws and early motion improved the prognosis.
Complications of talar injuries include AVN of the body and head, malunion and nonunion, bony ankylosis, skin necrosis, infection, impaired joint mobility, neurovascular compromise, and tendon trapping. The late development of posttraumatic degenerative joint disease of the ankle, subtalar, and midtarsal joints has been reported.4,5,10,12,14,16
The purpose of this study was to report the experience of two Level One Trauma Centers with talus fractures regarding their incidence, methods of treatment, assessment of the outcome results and complications.
MATERIALS AND METHODS
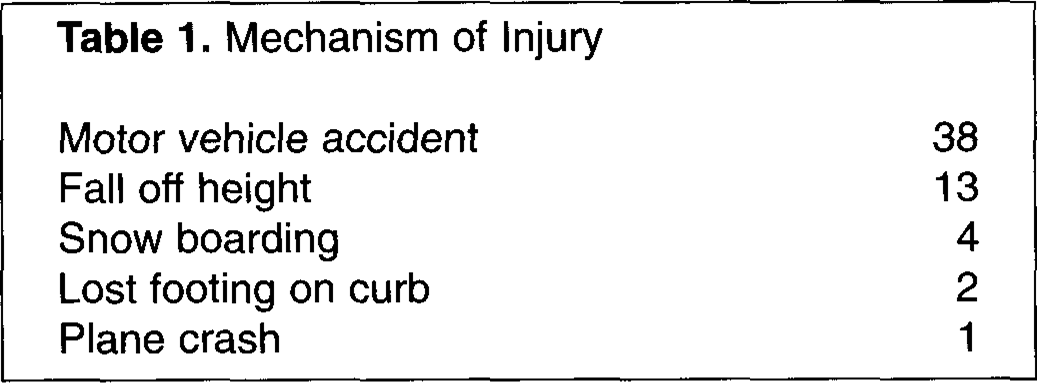
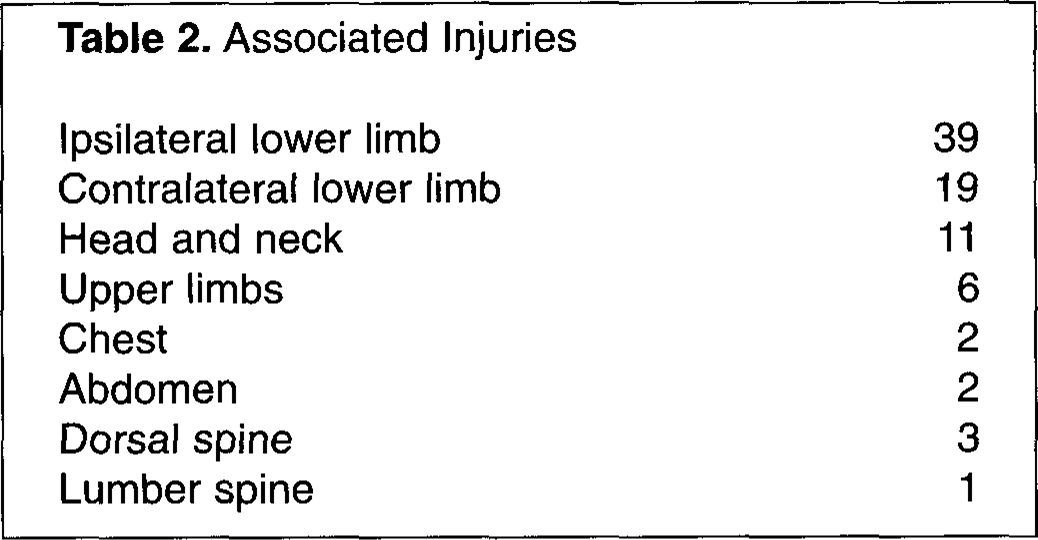
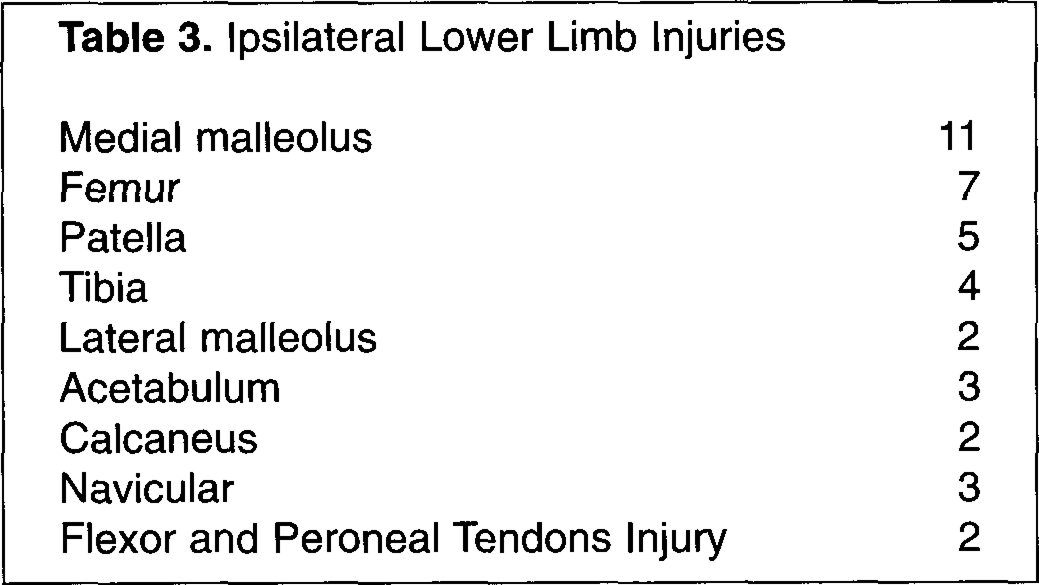
A retrospective study was undertaken to assess the outcome in all patients with talus fractures who were admitted to two level one Trauma Centers between 1992 and 1997. Computerized medical records showed that during this five year period patients with talus fractures represented 1.68% of all the trauma cases. The patients with talar fractures were contacted by telephone or mail and were requested to attend reassessment in the fracture clinic. Fifteen patients were excluded, 13 were unable to attend for clinical examination and two patients had below knee amputation for severe associated neurovascular, lower tibia and calcaneus injuries. Fifty-eight patients with 60 talar fractures attended for review. There were 39 men and 19 women. The average age at the time of the injury was 32 (range, 14–74). The side of the fracture was right in 37 and left in 23. Table 1 shows the mechanism of injury. The two bilateral talar fractures occurred after motor vehicle accidents. All patients but eight had other injuries; 39 patients had other injuries in the ipsilateral lower limb. The most common ipsilateral injury was fracture of the medial malleolus. Tables 2 and 3 show the associated injuries.
Mechanism of Injury
Associated Injuries
Ipsilateral Lower Limb Injuries
The Difference between the Three Rating Systems
ASSESSMENT OF RESULTS
Clinical evaluation was performed using three different rating systems:
American Orthopedic Foot and Ankle Society, Ankle-Hindfoot Score (100 points; excellent 90-100, good 75–89, fair 50–47, failure <50).
9
Maryland Foot Score (100 points; excellent 90–100, good 75–89, fair 50–47, failure <50).
15
Hawkins Evaluation Criteria (15 points; excellent 13–15, good 10–12, fair 7–9, failure 6 or less).
6
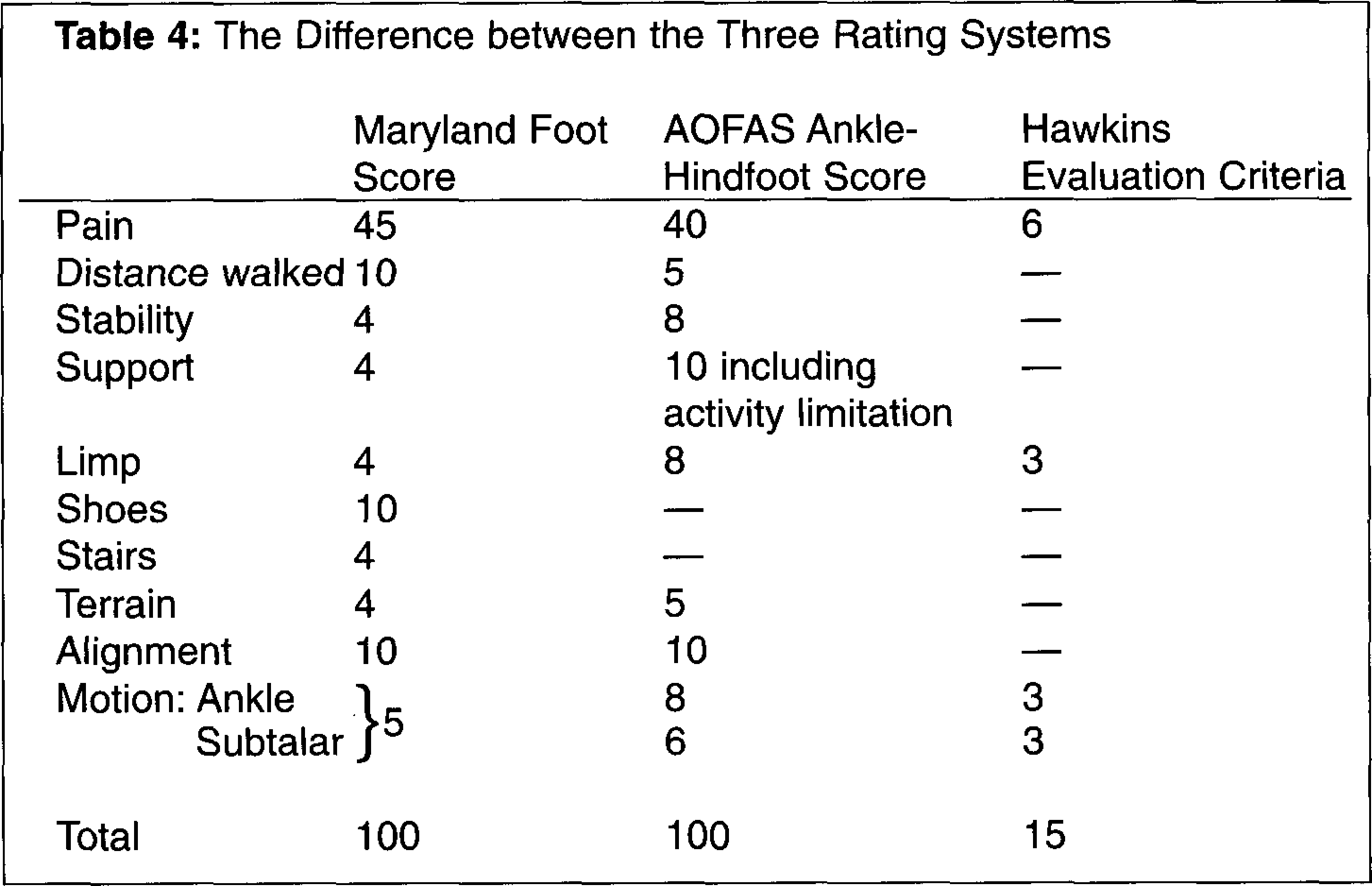
The difference between the three scoring systems is shown in Table 4.
The assessment involved review of the plain radiographs, CT scans, and MRI.
A computer statistical program SPSS 8.0 for Windows was used to analyze the data. A Fisher's test was used to compare the results with the three rating systems. Significant differences were determined as P 0.05.
RESULTS
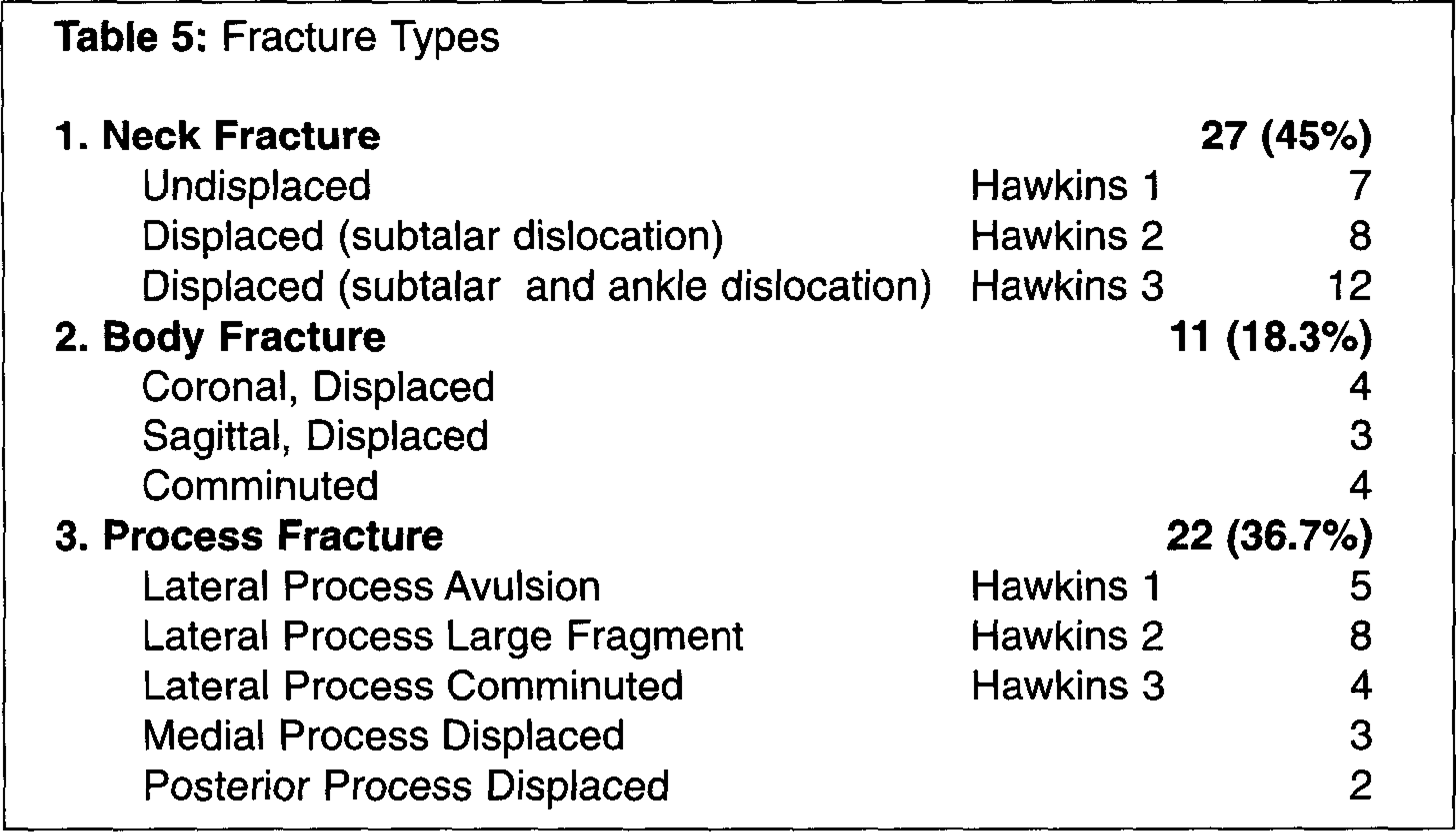
Out of the 60 fractures, 27 (45%) were neck (Fig 1), 22 (36.7%) process, and 11 (18.3%) body (Fig 2 and 3). Twelve (20%) fractures were open. Table 5 shows the fracture types.
Twelve cases had non-surgical treatment. One patient had primary tibiocalcaneal fusion (Blair's fusion) for open comminuted body fracture; the outcome was poor. One case of open comminuted body fracture was treated with an external fixator. Four cases had excision of comminuted lateral process.
Forty-two cases had open reduction and internal fixation. The most common method used for fixation of neck fractures was two 4.0 mm cancellous screws inserted from the anteromedial side without medial malleolar osteotomy. Minifragment and Herbert's screws were used for fixation of body and process fractures. Titanium screws were used in order to allow subsequent MRI scanning of the talus if AVN developed.
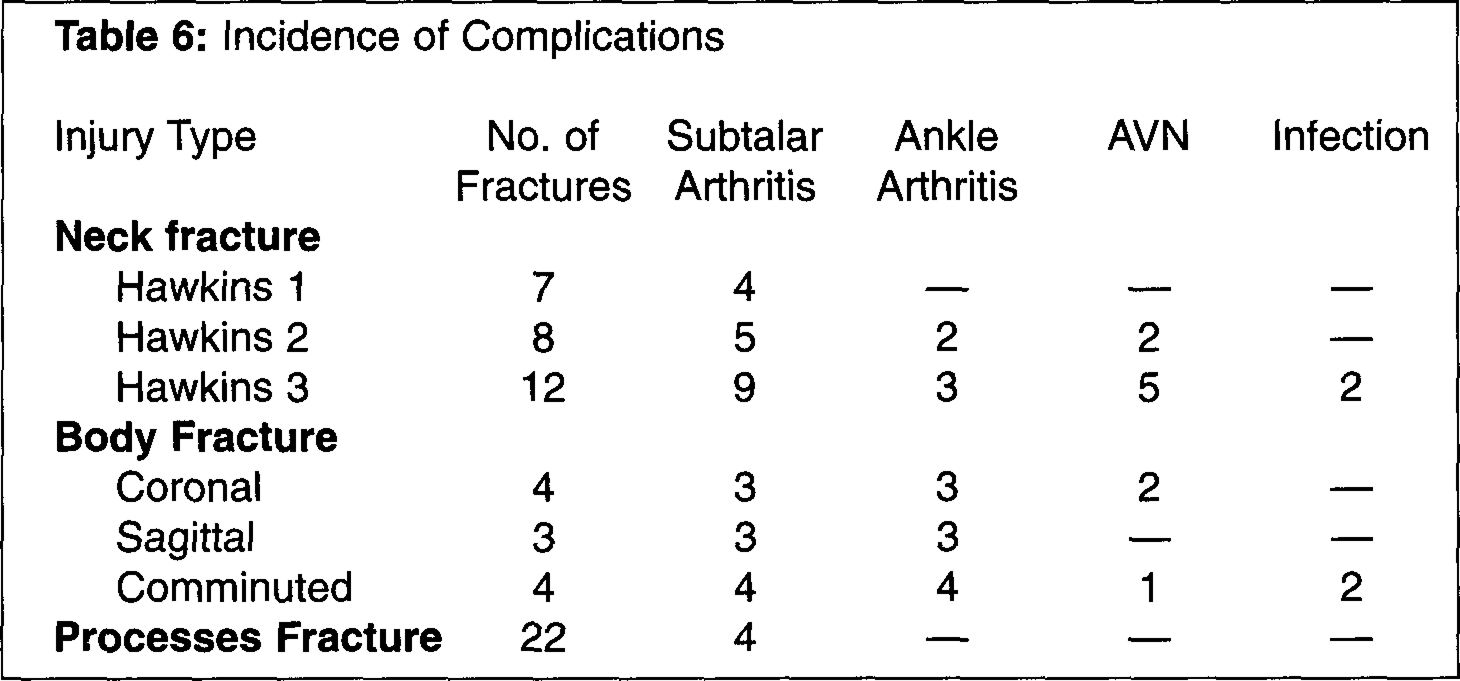
The average follow-up period was 30 months (range, 24–65). Thirty-two cases (53.3%) developed subtalar arthritis. Two patients had subsequent subtalar fusion. Fifteen cases (25%) developed ankle arthritis. None of these patients required ankle fusion. Fractures of the body of the talus were associated with the highest incidence of degenerative joint disease of both the subtalar and ankle joints. Ten fractures (16.6%) developed avascular necrosis. However, only one patient had subsequent collapse, and it was slight. Avascular necrosis occurred in 7 (25.9%) out of 27 patients with neck fractures and in 3 (27%) out of 11 patients with body fractures. Four cases had infection (6.6%); three of them were open fractures. One case developed talar shortening and cavovarus deformity and required triple fusion. Table 6 shows the incidence of complications with each fracture type.
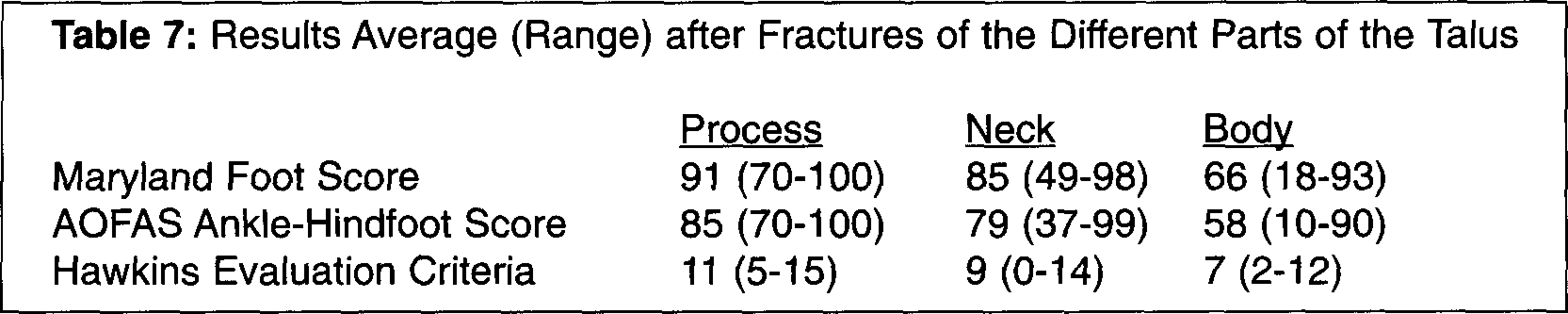
In this study three rating systems were used to assess the patients. The overall results with Maryland Foot Score were 34 excellent, 12 good, 10 fair, and 4 failure. According to American Orthopedic Foot and Ankle Society, Ankle-Hindfoot Scale 9 fractures had excellent results, 34 good, 11 fair, and 6 failure. According to Hawkins Evaluation Criteria 8 fractures had excellent results, 32 good, 8 fair, and 12 failure. There was a statistically significant difference in the results between Maryland Foot Score and AOFAS, Ankle-Hindfoot Scale (P & 0.01). There was also a statistically significant difference in the results between Maryland Foot Score and Hawkins Evaluation Criteria (P & 0.01). No statistically significant difference was detected in the results between AOFAS, Ankle-Hindfoot Scale and Hawkins Evaluation Criteria (P = 1.00) (Fig 4). All the three rating scores showed that the process fractures had the best results followed by the neck and then the body fractures. Table 7 shows the results with different fracture types.

(a) Preoperative lateral plain radiograph showing Hawkins Type III fracture neck of talus associated with fracture of the lateral malleolus,
DISCUSSION
Computed tomography scanning was done preoperatively in most of the cases and was helpful in planning the method of treatment. The difficulty of diagnosing some acute talar injuries with plain radiograph has been demonstrated. Computed tomography scanning has been shown to be a superior modality when clinical circumstances suggest a fracture.3,7 Titanium screws were used for fixation in order to allow for MRI scanning of the talus if AVN developed.
Displaced central fractures of the talus are associated with a high percentage of permanent disability.4,16 Although fractures of the body of the talus in our series were less frequent than fracture of the neck or talar process, they had the highest incidence of degenerative joint disease of both the subtalar and ankle joints. Four patients had comminuted body fracture; two of them were open. One case was managed with external fixator and the other patient had primary tibiocalcaneal fusion (Blair's fusion); the outcome for both was poor. Two patients had reconstruction of the body with minifragment and Herbert screws. The three rating scores used in the current study showed that the two patients who had reconstruction of the body had better results than the cases that have been managed by external fixator or primary tibiocalcaneal fusion. Preservation of the talus and reconstruction of the body, if possible, should be considered in all cases.

Fracture Types
Incidence of Complications
Results Average (Range) after Fractures of the Different Parts of the Talus
This study confirmed that AVN was not as common a problem as some of the literature suggested.2,6,14 Ten fractures (16.6%) developed avascular necrosis; 7 of them had Hawkins Type 2 or 3 neck fractures. Out of the ten patients who had AVN only one developed partial collapse. None of these patients required further surgery. The finding that the most common and disabling complication in this series was degenerative joint disease of the subtalar and ankle joints agreed with Szyszkowitz et al. 16 and Frawley et al. 4 who found similar results in their series.
The three rating scores used in this series to assess the outcome have combinations of subjective and objective parameters of the function of the foot.6,9,15 The outcome was different with every rating score. However the outcome with AOFAS, Ankle-Hindfoot Score and Hawkins Evaluation Criteria were almost equivalent. Maryland Foot Score does not differentiate between the ankle and subtalar motion and gives both collectively 5 points; in addition it involves 14 points on shoes and stairs.
This study showed that fractures of the body of the talus were associated with the highest incidence of degenerative joint disease of both the subtalar and ankle joints. We thought that the low incidence of AVN in the current study has been attributed to early anatomical reduction and stabilization of the fracture as presumed by other authors. 4
