
Abstract
We describe a rare manifestation fibroma in a tendon-sheath in an 83-year-old man. The patient complained initially of a slowly progressive spreading, apart of the right second and third toes. A mass was found in the plantar aspect of the foot. It was completely excised at surgery. Histological examination revealed sparse spindle or stellate cells with slit-like vessels in the dense collagenous matrix. There had been no recurrence at follow-up 17 months after surgery.
INTRODUCTION
Fibromas of a tendon-sheath in the feet are rare. Chung and Enzinger observed them in only six of the 139 cases in their pioneering study. 2 Since then, sporadic case reports of this tumor in the feet have been added. 1,4,6,10,13 To our knowledge, there have been less than 20 such cases published in English. The clinical manifestation in our case was unusual. Most patients with fibromas of a tendon-sheath, including cases in the feet, complain of small, painless nodules or mild pain. 1,2,6,9,10,13, This patient initially complained of deformity of the toes.
CASE REPORT
An 83-year-old man sprained his right foot in March, 1998. The acute symptoms diminished within a week, but a slight swelling over the right toes remained for several weeks. He began to notice a spreading apart of his right second and third toes in May, 1998. He consulted a dermatologist in June, 1998. An exploratory puncture between the toes revealed no pus or discharge at that time. He underwent follow-up without any treatment for several months, but, in October, 1998, began to feel discomfort while walking. The spreading apart of the toes had continued to progress slowly. He was referred to our hospital in March, 1999.
Physical examination noted swelling and spreading apart of the patient's right second and third toes. Both toes were slightly hyperextended, and the nail of the third toe was rotated externally. A soft tissue mass was palpated in the plantar aspect of the toes. It was firm, ill-defined, and slightly tender. The overlying skin was normal. His previous medical history included diabetes mellitus and hypertension.
Radiographic examination revealed an increased density in soft tissue between the right second and third toes on which proximal phalanges were deviated (Fig. 1). In magnetic resonance imaging, the mass demonstrated homogeneous low-signal intensity on T1-weighted images, and a mixture of low- and high-signal intensity on T2-weighted images (Fig.2). A fine needle aspiration biopsy yielded no malignant cells.

Anteroposterior radiograph revealing an increased density in soft tissue between the right second and third toes (arrows). The second and third proximal phalanges are deviated.

T1-weighted magnetic resonance image revealing a hypointense soft tissue mass in the plantar aspect of the right foot.
Surgery revealed the mass to be densely adherent to the plantar aponeurosis and extending into the space between the second and third toes (Fig. 3). It was excised totally along with the involved aponeurosis. On gross examination, the tumor, measuring 4 × 2.5 × 2 cm, was white and rubbery and exhibited multinodular growth. Histopathological examination revealed sparse spindle or stellate cells associated with a dense fibrous stroma, as well as slit-like vessels (Fig. 4). The cells were arranged randomly and were devoid of cellular pleomorphism. There were some foci of myxoid degeneration in the matrix. A follow-up in August, 2000, showed no local recurrence, and the patient's toes clinically appeared normal.

Intraoperative photograph of fibroma of a tendon-sheath, exhibiting multinodular growth.
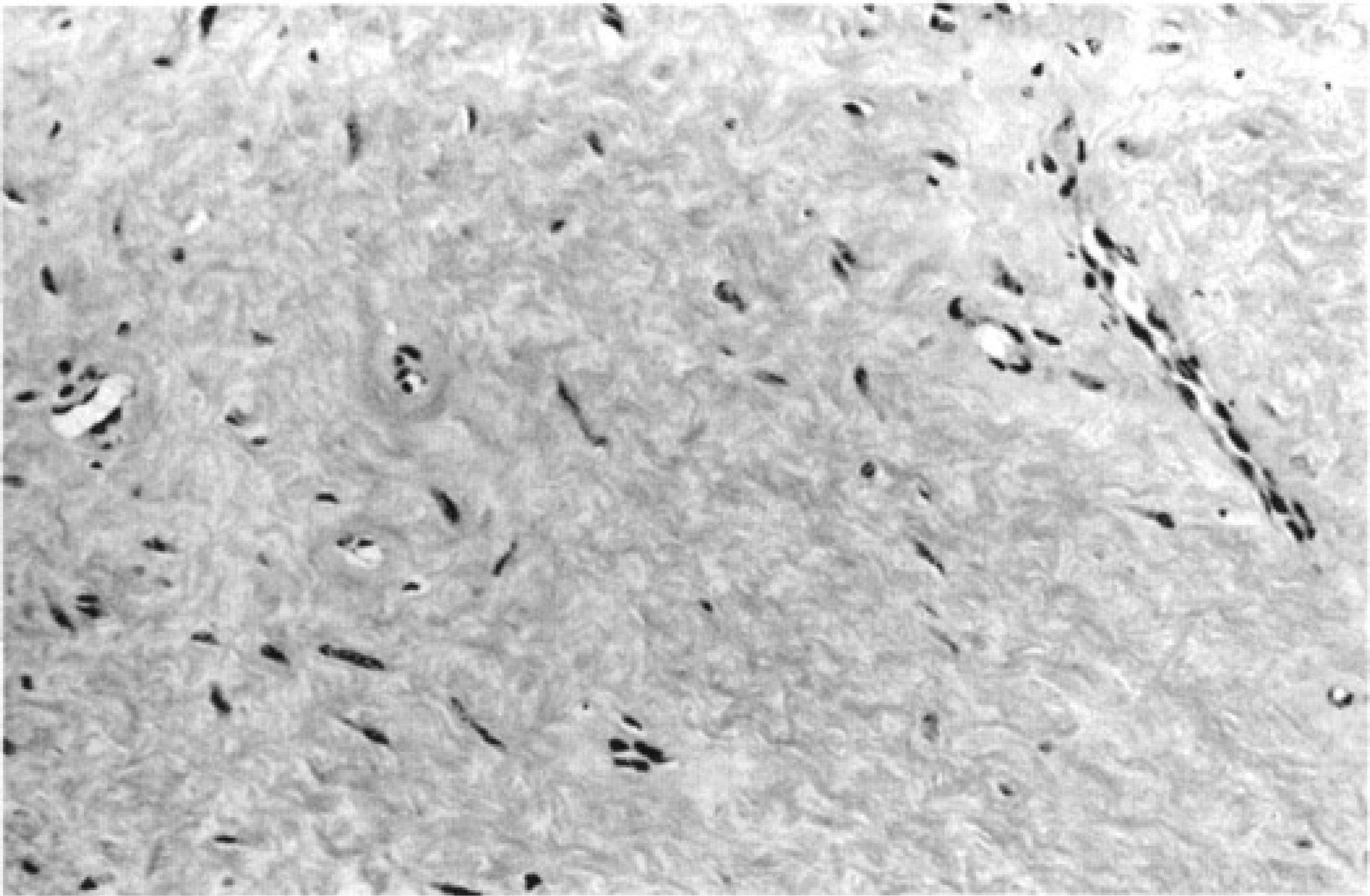
Photomicrograph of fibroma of a tendon-sheath. The tumor consisted of sparse spindle or stellate cells associated with a dense fibrous stroma (hematoxylin and eosin, original magnification × 200).
DISCUSSION
Fibroma of a tendon-sheath is a benign, uncommon tumor first described by Chung and Enzinger in 1979. 2 Most cases feature a slowly growing, painless, firm mass adherent to tendon-sheaths of the hands, wrists and fingers. The mean age of patients undergoing excision is 30 to 35 years, and men outnumber women. 2,9 Histologically, the tumors consist of benign-looking spindle cells scattered in a dense fibrous matrix. In many cases, slit-like vascular spaces are prominent. 2,5,7,9,12 Some patients with the disease, as in this case, have a history of antecedent trauma (6% to 9%). 2,9 Histologically, the tumor should be distinguished from other fibrous tumors. The Dupuytren type of fibromatosis more commonly causes a contracture or deformity of the fingers and toes. On gross examination, fibromas of a tendon-sheath resemble Dupuytren fibromatoses and extra-abdominal desmoid tumors, both of which are white and have firm masses, but, fibromas of a tendon-sheath grow in a multinodular fashion, while the other two lesions extend in a diffuse pattern. 3 Histologically, fibromas of a tendon-sheath are paucicellular, and their fibroblasts are arranged haphazardly in a dense collagenous stroma. 5,7,12 In contrast, extra-abdominal desmoid tumors and Dupuytren fibromatoses are composed of parallel fascicles of collagen fibers with hyper-cellularity. 3 Some recent reports note a histological transition between fibromas and giant cell tumors of a tendon-sheath. 8,11 The presence of giant cells and histiocytic cells arranged in a sheet is the key to diagnosing giant cell tumors of a tendon-sheath.
We concluded that orthopaedic surgeons should be aware of the possibility of encountering uncommon fibromas of a tendon-sheath in the foot. It may appear to be a soft tissue tumor. Tumors causing mechanical displacement should be included in the differential diagnosis when patients are seen with foot and toe deformities. Fibromas of a tendon-sheath should be included in the differential diagnosis when examining patients with deformities of the toes.