
Abstract
Nine feet of eight patients with neurologic foot deformities caused from poliomyelitis, Charcot-Marie-Tooth disease, and traumatic nerve injury were treated with V-osteotomy and the llizarov method. A painless and plantigrade foot was obtained in all but one patient. A residual deformity occurred in this case because of the soft-tissue problems during the correction period. No major complication had been encountered by the latest follow-up at a mean of 42 months. The results of the current study indicate that the V-osteotomy and the llizarov method, while technically difficult, is an effective method for correcting neurologic foot deformities and obtaining a stable, plantigrade, painless foot, especially when complicated with other lower leg problems (i.e., leg length discrepancy, joint contractures).
INTRODUCTION
Paralysis of the muscles acting on the foot may result in various deformities and functional disability of the foot. Initially, muscle imbalance produces progressive deformity that is flexible. With skeletal growth, fixed soft tissue and bone deformities develop in the foot, especially in poliomyelitis and Charcot-Marie-Tooth (CMT) disease. 1,9,15 Additional complicating factors include instability due to muscle imbalance, sensation problems, poor soft-tissue conditions (previous surgery or bunions), knee and hip contractures, and leg length discrepancy (LLD).
Traditionally, correction of neurologic foot deformities has been managed through extensive soft-tissue releases, tendon transfers, osteotomies, or arthrodeses. 1,3,9,13 –16 The goal of all treatment methods is to provide a painless, plantigrade, stable foot that can fit into a shoe without undue difficulty. 9,15,16 In conventional techniques, acute correction of the deformity may result in neurovascular injury and soft tissue problems. In rigid foot deformities, tendon transfers must be performed after correction of the deformity. 2,4,6
The llizarov technique combined with a “V-osteotomy” may be successfully used in the foot with deformity secondary to neurologic impairment.
MATERIAL AND METHODS
A total of nine rigidly deformed neurologic feet belonging to eight patients, treated with the llizarov method, were included in this study (Table 1). The average age of the patients was 17.6 (range, 9 to 26) years. The causes of the deformities were poliomyelitis sequela in six patients, bilateral CMT disease in one, and traumatic nerve injury in one. Three of nine feet had undergone previous surgical intervention. In six cases, the mean LLD was 5.6 (range, 3 to 12) cm. The patients whose deformities had been caused from bilateral CMT disease and traumatic nerve injury were walking on the dorsolateral site of the foot. We performed corrections by utilizing a V-shaped osteotomy method in all feet. Additional procedures performed by external fixators were tibial osteotomy in three, femoral osteotomy in one, simultaneous tibial and femoral osteotomies in two patients for lengthening and deformity correction, knee contracture release in one, and simultaneous knee and hip contracture releases in one patient.
All patients received preoperative evaluation of both lower extremities. This evaluation consisted of range-of-motion measurement, neurovascular status assessment, two plane and posterior tangential radiographies, three-dimensional (3D) computed tomographic (CT) reconstruction of the foot, orthoroentgenography, and photography (Fig. 1).
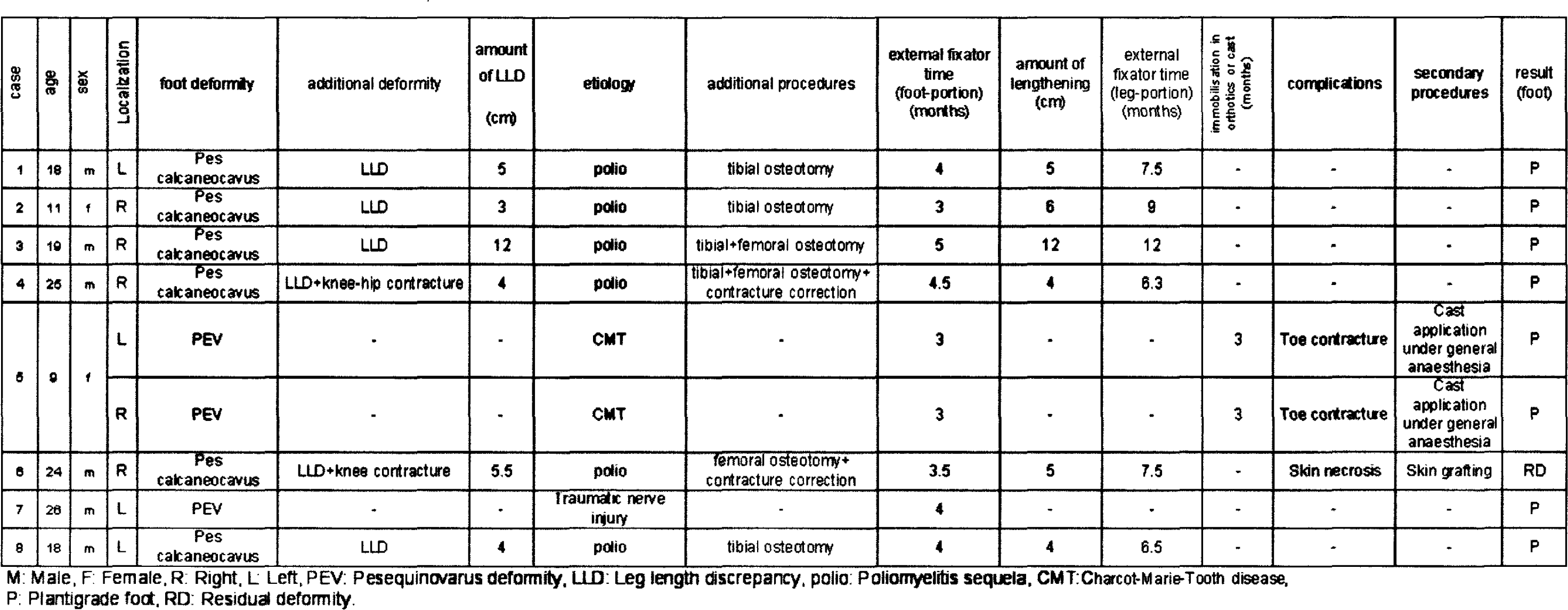
M: Male, F: Female, R: Right, L Left, PEV: Pesequinovarus deformity, LLD: Leg length discrepancy, polio: Poliomyelitis sequela, CMT:Charcot-Marie-Tooth disease, P: Plantigrade foot, RD: Residual deformity.
Surgical Method
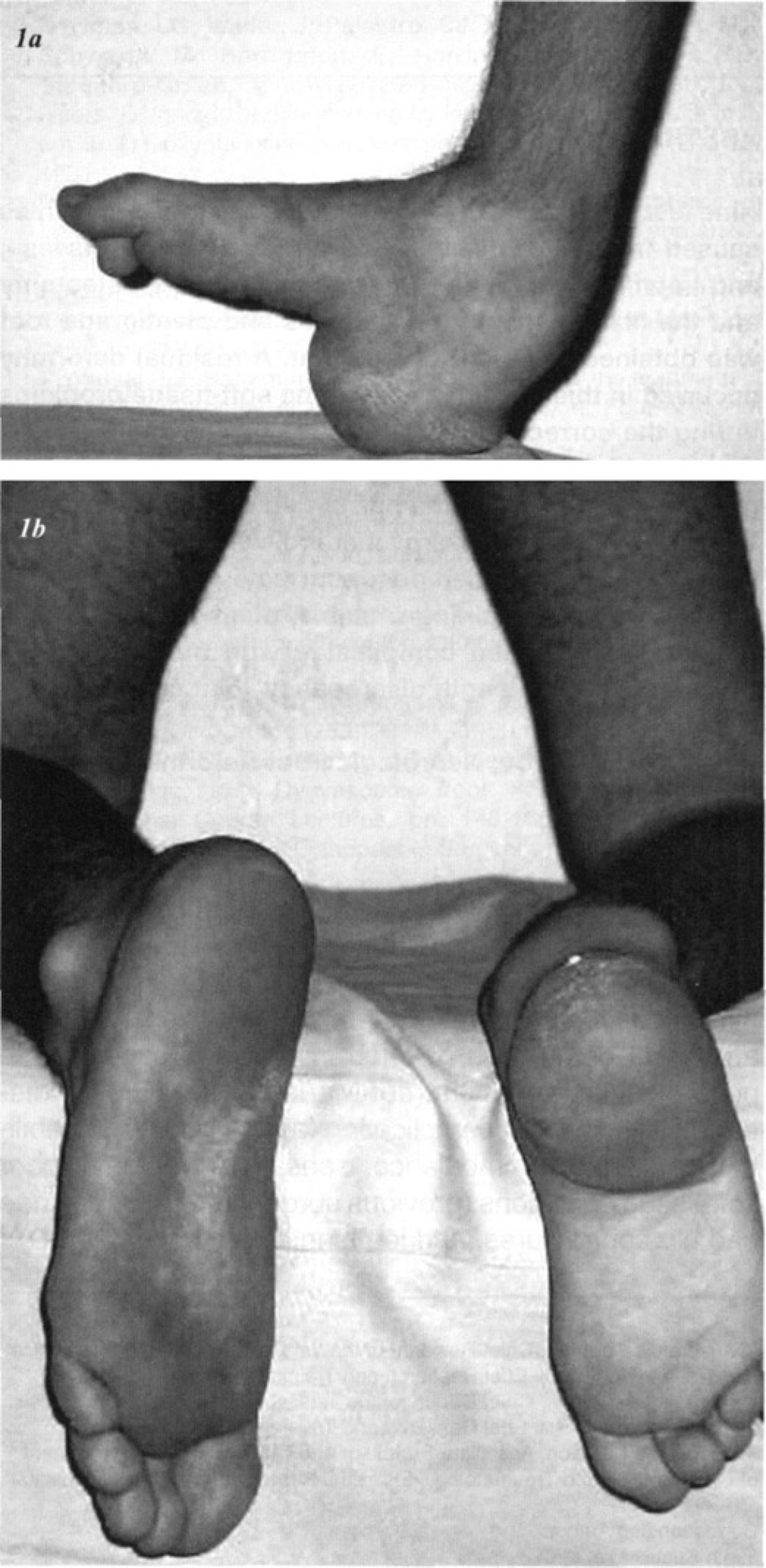
19-year-old male patient with poliomyelitis sequela (Table 1, case three). He had a 12-cm leg length discrepancy and pes calcaneocavus deformity on the same site. He was unable to bear weight due to instability of the foot.
In all cases, surgery was carried out under general anesthesia without neuromuscular blockade. Epidural anesthesia was also used in four patients as a postoperative analgesic and as an aid to rehabilitation. A radiolucent operating table and image intensifier were used in all cases. Osteotomies were performed with tourniquet control. Distraction of the ankle joint was performed in order to prevent crushing of the cartilage of the joint. The tarsal tunnel was decompressed to protect the neurovascular bundle and to prevent acute tarsal tunnel syndrome in seven feet. 10,11
The “V-osteotomy” is a double osteotomy, where the anterior part of the osteotomy begins at the neck of talus and passes through anterior part of the calcaneus. The posterior part is performed between the dorsum of the calcaneal tuberosity and plantar surface of the foot. These two osteotomies produce a V-shape in the sagittal plane 10,11 (Fig. 1c). Between these osteotomies a triangular middle bone segment is created within the bodies of the talus and calcaneus. This mobile bone segment was stabilized with one or two K-wires, and connected to the lower ring of the base frame to enable correction of the anterior and posterior segment in relation to the middle segment. A lateral-oblique incision and osteotome were used for the posterior part of the V-osteotomy (Fig. 2a). The Gigli saw technique was used for anterior part of the V-osteotomy. 10

Pes calcaneocavus deformity and planning osteotomy sites are shown on lateral weight bearing X-ray and 3D-CT.

Postoperative early clinical appearance is presented.

Radiological image of the case at second week postoperatively. Distraction of the tibial osteotomy site also can be observed.

Posterior calcaneal osteotomy was performed with a lateral-oblique incision.

Gigli saw position was checked before the anterior part of the V-osteotomy. Posterior calcaneal osteotomy also was shown on figure.

Anterior part of the V-osteotomy was performed with Gigli saw. As shown on figure, the distal end of the posterior calcaneal incision was used as the fourth incision.
Our Gigli saw technique is quite similar which was described by Paley. 10 Our technique involves three small incisions. A 0.5-centimeter incision is made through the lateral aspect of the talar neck under image intensifier control. From this incision, a long-bent hemostat is passed through between the dorsal aspect of the talar neck and extensor tendons. Another 0.5-cm incision is made between the lateral border of the tibialis posterior tendon and the medial aspect of the talar neck. The second incision should be placed at the end of the bent hemostat which was previously passed through the first incision. The Gigli saw is grasped and pulled away from the second incision by this hemostat. One more incision is necessary at the plantar aspect of the first incision. We used the distal end of the posterior calcaneal osteotomy incision as the fourth incision in our cases. The Gigli saw was employed around the talar neck and anterior part of calcaneus with similar manner. After checking the Gigli saw position with an image intensifier, the osteotomy is completed (Fig. 2b, 2c). Minor differences between our technique and Paley's technique are:
suture material is not used for passing of the Gigli saw around the bones and,
the distal end of the posterior calcaneal incision is used as the fourth incision.
We observed that during the passing of the Gigli saw around the bones by suture material, the tip of the Gigli saw was grasped by soft tissues even if the tip of the Gigli saw is smoothened.
The foot frame, which mimics foot deformity, was constructed preoperatively. The frame mainly consists of three parts:
the base frame, which is required on the leg,
the heel frame, and
the forefoot frame.
The base frame is composed of two rings that fix the tibia with a single K-wire and a single Schanz pin from each ring. If additional deformity required correction such as leg length discrepancy or joint contractures, a base frame was prepared for these deformities. The square heel frame is preferred to the half ring. The heel and forefoot frame were made of radiolucent material in order to obtain the best postoperative radiological images. Two crossed olive wires on the heel frame and two parallel olive wires going through the first and fifth, and under the second, third and fourth metatarsals on the forefoot frame were used. Additionally, one or two wires were used in the mobile bone segment created by V-osteotomies.
Correction was started on the second postoperative day instead of the seventh day, to prevent premature consolidation. The goal of the distraction procedure was to obtain a 1 mm/day opening at the osteotomy site. Distraction rate was reduced when excessive soft tissue tension was observed during the correction period. The fixator was removed after obtaining consolidation at the distraction site. In a patient who had bilateral CMT disease, the fixators were removed earlier than the others (at the third month) to provide patient mobility. She was protected with a cast and orthotics for an additional three months for complete adaptation of soft tissue in order to prevent recurrence of the deformity. In this patient, the toe contractures were occurred in fixator treatment, and corrected manually with cast application which was performed under general anesthesia at the time of frame removal.
RESULTS
At the time of fixator removal, a plantigrade foot was achieved in eight feet and leg length discrepancy was eliminated in six extremities. Compared to the preoperative status, all patients were satisfied with their gait. The length of follow-up from surgery averaged 42 (range, 26 to 48) months. The correction period varied from three to six weeks. The mean external fixation time was 3.8 (range, three to five) months in the foot portion of the frame and 8.1 (range, 6.3 to 12) months in the leg portion of the frame. In patients with LLD, the amount of lengthening obtained averaged six (range, four to 12) cm. In an 11-year-old patient with poliomyelitis sequela, a 3-cm overlengthening was performed (Table 1, case 2). Nonunion, hardware failure, psychological intolerance requiring fixator removal, and acute tarsal tunnel syndrome were not observed in any of our patients. The complications encountered in the study group included toe contractures (two feet) and skin necrosis at the distraction site of the foot (one foot). The toe contractures in a patient with bilateral CMT disease were treated manually with cast application under general anesthesia at the time of frame removal. In one patient, skin necrosis occurred during the distraction period and correction was discontinued. Skin necrosis at the distraction site of the foot required treatment with split thickness skin grafting. The final result of this case was residual deformity. Minor grade 1 and 2 pin tract problems according to Paley's classification 12 were observed in all cases. These superficial pin-site problems were controlled with local pin care. None of these complications required the removal of any K-wires. Combinations of arthrodesis and/or soft-tissue procedures such as tendon transfers, release of plantar aponeurosis or joint capsules were not required in the treatment period.
DISCUSSION
In this study, foot deformity due to poliomyelitis, CMT disease, and traumatic nerve injury were classified as “neurologic foot deformity.” Traditional management of the neurologic foot deformities required a combination of soft tissue and bony procedure for correction of many components of the deformity. 3 In selected patients, tendon transfer can be performed after correction of the deformity. 6,7 Previously described methods of triple arthrodesis may correct most of the deformities involving the midfoot. These methods can reduce the height of the foot, lower the malleoli, and cause difficulty in fitting shoes. The most commonly reported complications of triple arthrodesis are nonunion, residual deformity, recurrent deformity, and avascular necrosis of talus, which may require further operations. 1,3,13,14,16 In these conventional methods, possible reasons of deformity recurrence are associated deformities of the remainder of the limb, inability to maintain the position of fusion in cast, or nonunion accompanied with residual muscle imbalance. 16
There are two ways in which foot deformities can be corrected using the llizarov method: with osteotomy and without osteotomy. 5,7,8,10,11 In treatment without osteotomy, deformities are corrected via joints and physes rather than bone. Osteotomy treatment is recommended in cases of fixed-bone deformity in patients older than eight years and for patients with neuromuscular imbalance in whom soft-tissue correction would obtain but not maintain the correction, and in whom tendon transfer was not possible to maintain the correction. 7,8,10,11 In the current study, we used the llizarov method with osteotomy in cases with foot deformities and neuromuscular imbalance. We preferred the V-osteotomy in our patients because it produces a stiff subtalar joint. This characteristic of the V-osteotomy is especially important in the neurologic feet, which have instability due to muscle imbalance.
The llizarov method and V-osteotomy have some advantages over conventional methods: The llizarov method is able to correct all components of the deformity separately and provides a stable foot like the triple arthrodesis, but with lower complication rates. The neurologic foot deformities were usually accompanied with other problems such as LLD and joint contractures. All these problems can be treated with the llizarov method at the same time (Fig. 1). Also, in six of nine extremities which had LLD, an average 6 (range, 4 to 12) cm lengthening was accomplished. In an 11-year-old patient with poliomyelitis sequela who had growing potential at the time of treatment, a 3-cm overlengthening was performed. In the conventional methods, the final correction is achieved intraoperatively. The llizarov method, on the other hand, is amenable to adjustment during the entire treatment period. In this method, osteotomy is used instead of bone resection, the height of the foot is not reduced and shoe-fitting problems are prevented. 2,4 –7
A number of techniques have been described for triple arthrodesis. 1,3,9,13,14,16 The two-incision approach is often advocated to gain better access to the talonavicular joint. 14,16 This approach may increase morbidity, especially for neurological foot deformities. In the llizarov method the incisions are usually smaller, and extensive periosteal stripping and soft-tissue dissection are not required. This reduces the risk of tissue damage from surgery.
The goal in the treatment of foot with CMT disease is to produce a stable plantigrade foot. If a plantigrade foot is obtained by performing osteotomies and/or tendon transfers, the patient will have a pliant foot, which is generally more functional than a rigid one. If the deformity is too intense, stabilization procedures such as arthrodesis are required. 9 The patient with bilateral CMT disease who was able to walk on the dorsolateral site of the feet was treated with the llizarov technique because of the severe deformity (Table 1, case 5).
Clinical and radiological images after deformity correction are shown on figures respectively.
In the llizarov method, the risk of premature consolidation and/or incomplete osteotomy are more frequent in the foot compared to osteotomies of other bones. 5,10 –12 Paley stated that premature consolidation occurs from incomplete osteotomy or incorrect mechanical construct. 12 We think that the main shortcoming of the llizarov method and osteotomy treatment in the foot is the original status of the foot. If the distraction rate is regulated to obtain a 1 mm/day opening at the osteotomy site, excessive soft tissue distraction can be created at the concave side of the deformity, which may result in soft tissue necrosis. If the distraction rate is regulated to obtain a 1 mm/day soft tissue distraction, the osteotomy site may consolidate prematurely. For that reason, equilibrium of the distraction rate between the soft tissues and bone must be maintained. This regulation is more important in neuromuscular foot deformities, which may have problems in soft-tissue condition. We start the correction on the second postoperative day instead of the seventh day because of these problems. In the current study, only one residual deformity occurred. In this patient, equilibrium of bone and soft tissue distraction could not provided and skin necrosis developed on the medial side of the foot. During treatment of the skin necrosis with split thickness skin grafting, the osteotomy site consolidated. In this case no more correction could be obtained. While the Gigli saw technique is technically difficult, it eliminates the risk of incomplete osteotomy. In our series, Gigli saw technique was used in the anterior part of the V-osteotomy and incomplete osteotomy was not observed.
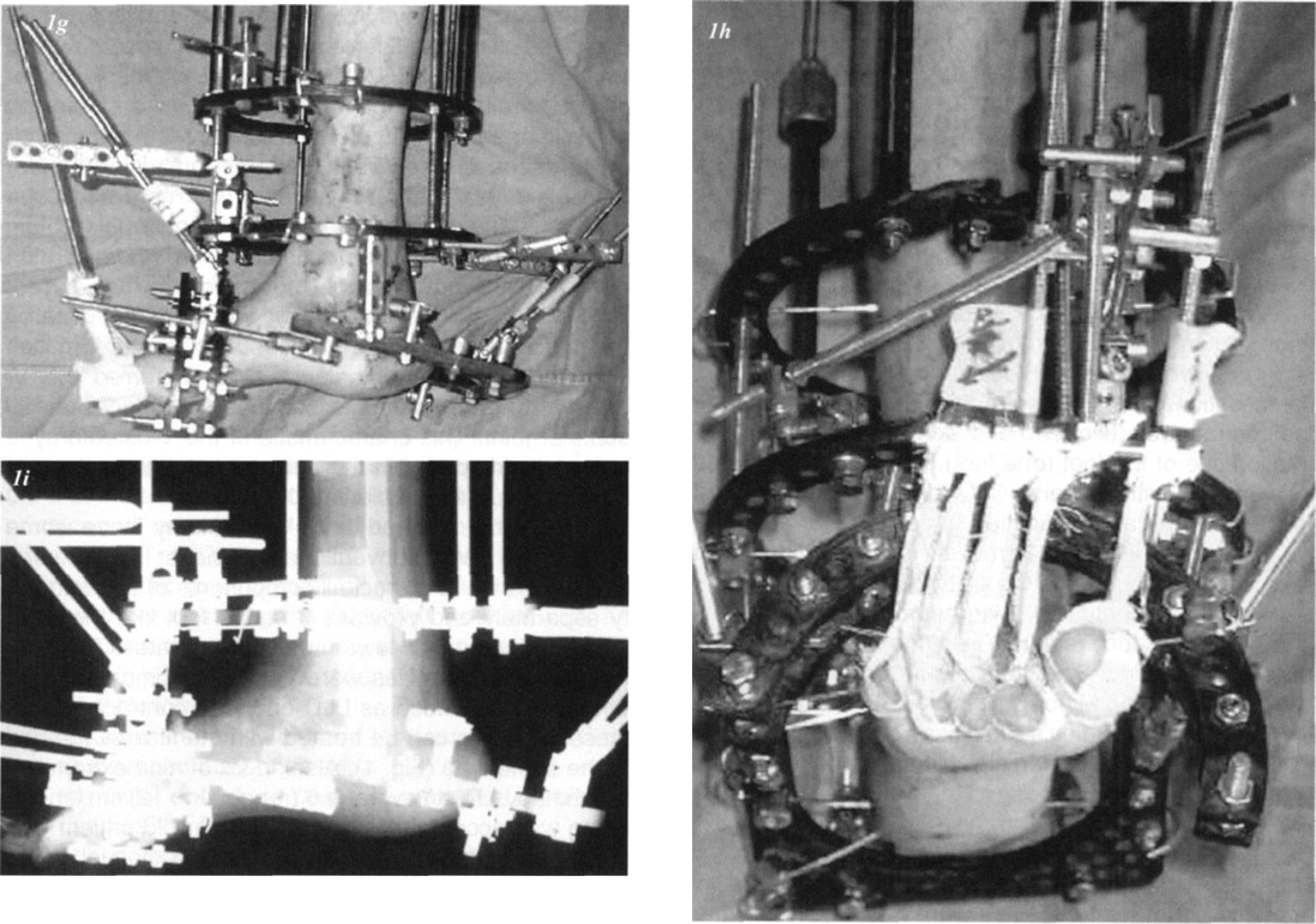
Toe contractures can be a common problem, especially in the medial column lengthening of the foot. 2 Prevention of toe contractures was achieved through the use of rubber slings or temporary K-wire fixation of the interphalangeal and metatarsophalangeal joints. 6,11 (Fig. 1g, 1h). In our study, toe contracture, which could not be prevented with conservative methods, recovered with fixator removal and cast application under general anaesthesia in one case.
Treatment of foot deformities by the llizarov method is technically difficult. Nonetheless, this method is particularly advantageous in treating neurologic foot deformities. Based on our findings, the llizarov method can successfully correct neurologic foot deformities.
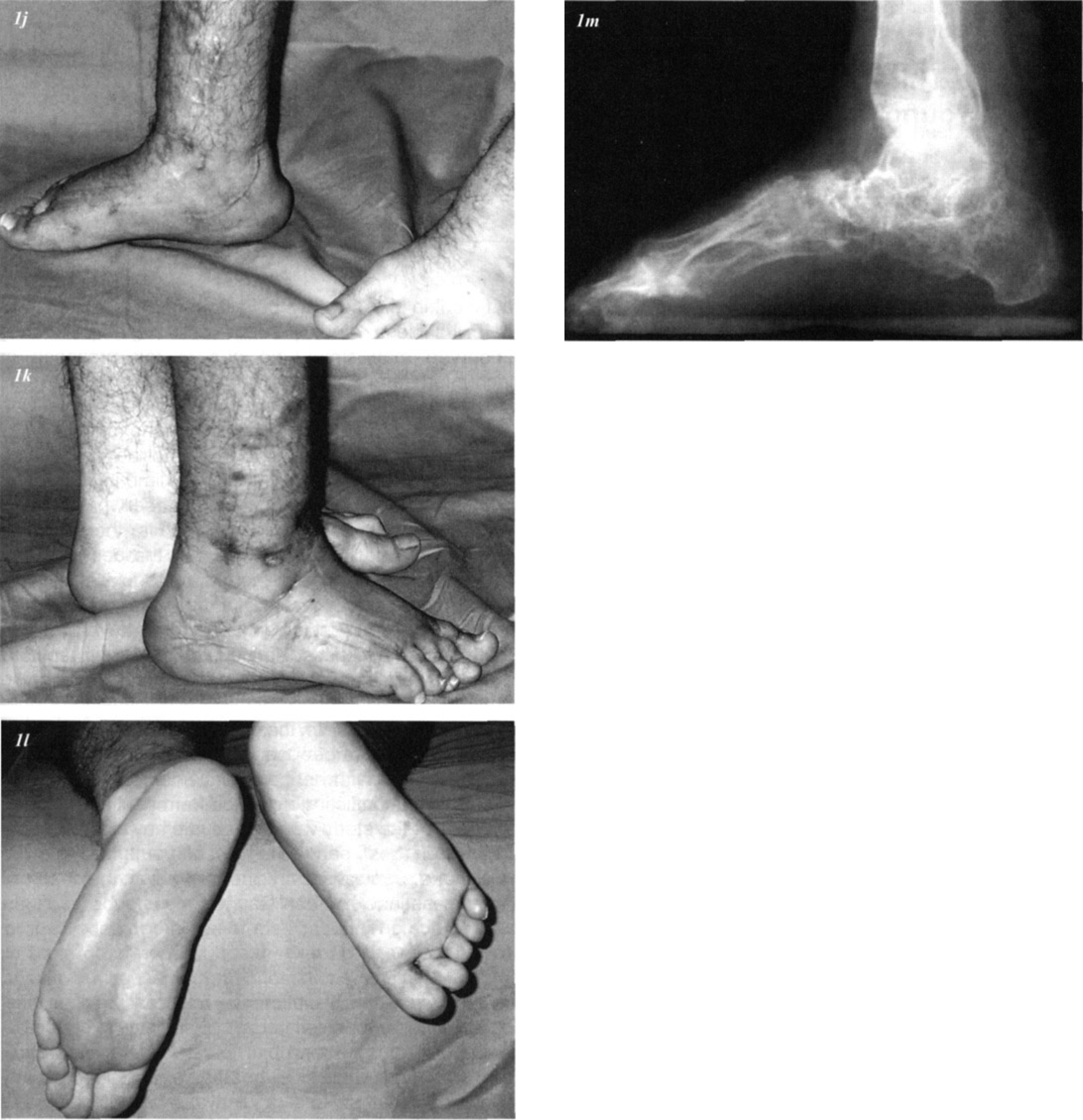
Foot part of the external fixator was extracted five months after the surgery. Plantigrade, stable, painless, normal sized foot was obtained.
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. No funds were received in support of this study.