
Abstract
Seventeen patients (20 feet) underwent Weil osteotomies of the second and third metatarsals for the treatment of central metatarsalgia and were reviewed at an average of 18 months postoperatively. Fourteen patients were completely satisfied with the results of their surgery (85%), one patient was satisfied, one patient satisfied with reservations and one patient was dissatisfied. The American Orthopaedic Foot and Ankle Society clinical rating scale improved by an average of 44 points. One patient had complete recurrence of symptoms, eight out of the 40 toes involved in surgery were floating, four toes were stiff, there were three cases of infection, and transfer metatarsalgia affected the fourth metatarsal in one case. The Weil osteotomy is an effective and safe procedure for the treatment of central metatarsalgia.
INTRODUCTION
Central metatarsalgia may be a primary mechanical problem or an iatrogenic problem affecting the second, third and sometimes fourth metatarsals. When nonsurgical methods fail, surgery may be considered. However, lesser metatarsal surgery is unforgiving 4 and traditional osteotomies such as the Helal 3 osteotomy are known to be fraught with complications such as non- or malunion, transfer metatarsalgia and floating digits. 6 Therefore, in recent years the Weil osteotomy has gained popularity.
The Weil osteotomy was first described by Dr. Lowell Scott Weil Sr., an American podiatric surgeon, and has been popularized in Europe by Dr. Louis Barouk, an orthopaedic surgeon. 1
The advantages of the Weil osteotomy (Fig. 1) over more traditional osteotomies include its stability. The geometry of the cuts are such that on weight bearing the fragments are pushed together. Also there is a large area of bone-to-bone contact, which allows the use of internal fixation, thus increasing primary bone healing and decreasing the risk of non- or malunion. 4 Recently, however, problems with the Weil osteotomy have emerged, especially that of floating stiff toes and transfer metatarsalgia. 7,8
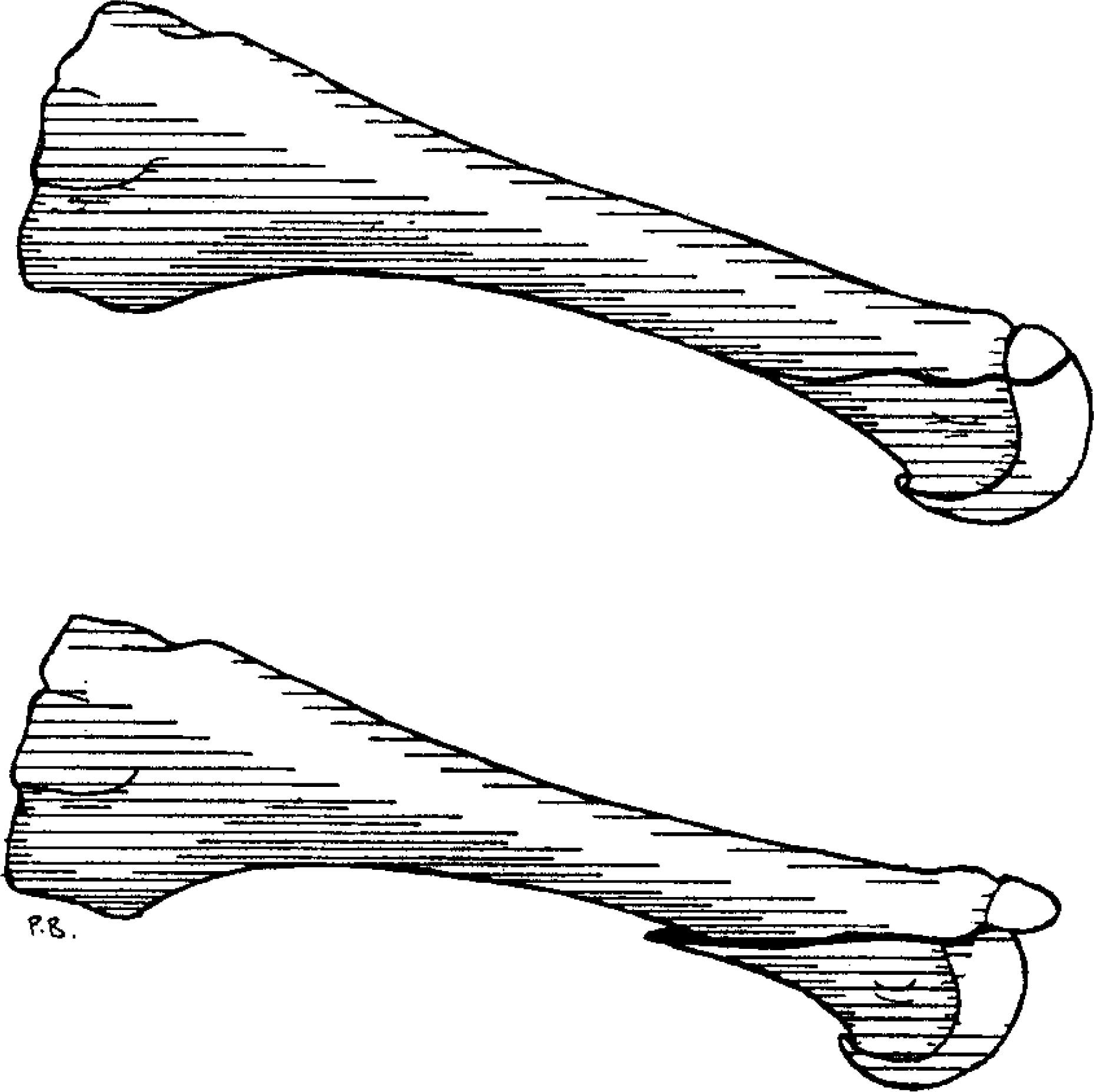
Diagram showing the Weil osteotomy.
Procedure selection is based on the following factors: metatarsal length, sagittal position of the second and third metatarsals, bone density, and the presence of degenerative joint disease at the metatarsal phalangeal joint. Metatarsal length and sagittal position are the most important factors in selecting the procedure. The Weil osteotomy should be used only in the presence of an abnormal metatarsal parabola. An elevating osteotomy may be the procedure of choice if the metatarsal heads are in a plantarflexed position. 4
PATIENTS AND METHODS
The first 19 patients undergoing Weil osteotomies of the second and third metatarsals performed by the senior author (TEK) were recalled for review at a mean follow-up of 18 months (average, 8.6 months). Seventeen patients (20 feet) returned for review and all were included in the study. Of the two who did not attend, one was deceased and one had been referred to a pain clinic with suspected complex regional pain syndrome. There were 16 females and one male. The average age at the time of surgery was 59 years (range 42 to 79). Three patients had bilateral surgery and 14 underwent unilateral surgery.
Twelve patients (13 feet) had previously undergone first metatarsal osteotomies consisting of: five Mitchells (for the correction of hallux valgus), five proximal plantar displacement osteotomies (for the correction of hallux limitus), two Keller's excisional arthroplasties and one Scarf/Akin osteotomy (for hallux valgus correction). The Scarf/Akin osteotomy patient had complained of central metatarsalgia prior to undergoing hallux valgus surgery. One patient had previously undergone a Weil osteotomy of the fourth metatarsal and subsequently developed transfer metatarsalgia of the second and third MTP joints.
Eight patients had other surgery at the same time as the Weil osteotomies. Twelve digital arthroplasties were performed on six patients, one patient had a neuroma excised and one patient had a Weil osteotomy of the fourth metatarsal.
The amount of shortening of the second and third metatarsals was measured using preoperative and final follow-up weight-bearing X-rays. The position and range of motion of the digits was also assessed.
The American Orthopaedic Foot and Ankle Society (AOFAS) (Fig. 2) clinical rating scale was used preoperatively and at follow-up. This is an objective measurement which measures the following five parameters: frequency and severity of pain, effect of foot problem on work and recreational activities, footwear requirements, joint motion and skeletal alignment/cosmetic appearance. Patients were also asked if they were completely satisfied with the result of their surgery, satisfied, satisfied with reservations or dissatisfied. All patients were asked if they would undergo surgery under similar circumstances again.

The American Orthopaedic Foot and Ankle Society Clinical Rating Scale used preoperatively and at final follow-up.
PROCEDURE
The amount of shortening required was determined by preoperative X-ray charting (Fig. 3). A method was used whereby a line was drawn between the first and fourth distal metatarsal articular surfaces. The protrusion above the line of the second and third metatarsal bisections determined the amount of shortening required.

X-ray showing preoperative charting.
The procedures were performed in all cases under local anaesthetic on a day-case basis and an ankle tourniquet was used.
The skin incision was made in the intermetatarsal space, which allows access to both metatarsals and also helps avoid digital contracture. 4 The capsule was then divided laterally, inferior to the extensor tendons and the metatarsal head exposed. This is essential for orientation, as without a view of the articular cartilage it is difficult to be certain where the metatarsal neck and shaft is. 4 The second-metatarsal osteotomy was performed first. The osteotomy cut was made as parallel as possible to the weight-bearing surface and the distal fragment displaced proximally (as determined by preoperative charting), fixed with one or two threaded 1.2-mm K-wires, and the overhang of bone removed with rongeurs. The osteotomy of the third metatarsal was then performed. It is important to assess the relative positions of the second and third metatarsals intraoperatively to ensure that the metatarsal parabola is maintained. The capsule was then closed using 3–0 vicryl sutures and the skin closed using 5–0 vicryl subcuticular sutures.
Postoperatively all patients wore a surgical shoe and used crutches for two weeks and were then encouraged to return to normal footwear and activities.
RESULTS
Seventeen feet had complete resolution of pain, two feet had partial resolution and one foot was no different than prior to surgery. Fourteen patients (17 feet) (85%) were completely satisfied with the results of their surgery; one patient was satisfied; one patient satisfied with reservations and the patient who had no resolution of foot pain was dissatisfied.
The second metatarsal was shortened an average of 5.2 mm and the third metatarsal an average of 5.4 mm.
The AOFAS clinical rating scale had a mean preoperative value of 44 (range 25 to 60) and a mean follow-up of 89 (range 53 to 100), showing an average improvement of 44.8 points. A paired t-test indicated a highly statistically significant improvement (p<0.0001) in AOFAS scores. All patients would be happy to undergo surgery again under similar circumstances if necessary.
COMPLICATIONS
The complications encountered were floating and stiff toes, soft-tissue infections, fixation irritation, transfer metatarsalgia and recurrence of initial symptoms.
Postoperatively, eight out of the 40 toes digits did not contact the ground on weight bearing (Fig. 4) and were said to be floating. Four toes were stiff. Three patients developed soft-tissue infections, which were all treated successfully with oral antibiotics. All the patients who had postoperative infections also presented with floating toes. One patient developed transfer metatarsalgia affecting the fourth metatarsal, which was treated nonoperatively with insoles and the patient is now pain-free. One patient had recurrence of her initial symptoms.

Floating toes following Weil osteotomies of the second and third metatarsals.
DISCUSSION
Weil osteotomies of the second and third metatarsals are an effective treatment for central metatarsalgia in the presence of an abnormal metatarsal parabola or as a salvage operation (Fig. 5) where the parabola has been altered by previous surgery. Ten feet (50%) in this study had previous shortening osteotomies of the first metatarsal, indicating the high incidence of transfer metatarsalgia associated with altering the metatarsal parabola. 5 All these patients are now pain-free following Weil osteotomies of the second and third metatarsals. This treatment should be considered when nonoperative methods fail and symptoms such as burning pain, a feeling of walking on pebbles or pain on the dorsal aspect of the joint persist.

X-rays showing pre and postoperative metatarsal lengths in a patient with central metatarsalgia following a Mitchells osteotomy.
The Weil osteotomy offers many advantages over more traditional osteotomies including stability, a large area of bone-to-bone contact, relatively easy application of internal fixation, control of shortening and return to normal weight-bearing activities at two weeks postoperatively.
Floating stiff toes are, however, now recognized as a common complication following the Weil osteotomy. 7,8 Trnka reported an incidence of 14 floating toes in 30 patients who underwent Weil osteotomies 7 and Vandeputte an incidence of 15%. In this study we found 20% of patients had floating toes and 10% stiff toes. However all these were asymptomatic. Trnka et al. have investigated this phenomenon of floating toes using three-dimensional sawbone analysis and cadavers. The results of Trnka's study indicate that it is impossible to make the Weil osteotomy cut parallel to the ground, which leads to plantarflexion of the metatarsal head as it is displaced proximally. 7 In the normal foot the interosseus muscle functions as a stabilizer and plantarflexor of the MTP joint. However, the axis of motion of the MTP joint changes with plantarflexion of the metatarsal head and the interosseus muscle acts as a dorsiflexor rather than plantarflexor, resulting in dorsal contracture of the MTP joint. 7
In this study all the patients with floating toes had required digital arthroplasties at the same time as the Weil osteotomies or had previous digital surgery indicating that the position of the digit prior to surgery was altered. All patients who developed postoperative infections had floating toes.
Shortening has been suggested as a cause 2 of floating toes. However, in this study, the amount of shortening ranged from 2–10.5 mm and increased shortening did not correlate with increased floating or stiffness.
CONCLUSION
We recommend the Weil osteotomy for the treatment of central metatarsalgia in the presence of an abnormal metatarsal parabola be it iatrogenic or primary in origin when nonoperative methods have failed.
In a group of 17 patients (20 feet) high levels of satisfaction were achieved. There were no cases of mal- or nonunion; no serious complications were encountered and no revision surgery necessary. Floating toes and restricted metatarsophalangeal joint motion may be encountered. However, this was not a cause of patient dissatisfaction in this study and the clinical significance of floating stiff toes has yet to be established.