
Abstract
Thirty-five ankles in 34 subjects with non-surgically managed stage 5 (chronic) osteochondral lesions of the talus (OLT) were reassessed an average of 38 months post diagnosis—88 months post symptom onset. The overall clinical result was rated good or excellent in 54%, fair in 17% and poor in 29%. Six patients opted for surgery—arthroscopic drilling—after a trial of one year of nonsurgical treatment and were therefore rated as poor. Tomogram or CT scans at the time of diagnosis and follow-up were compared in 25 patients. We found no significant change in lesion size and there was a poor correlation between change in lesion size and clinical outcome.
X-rays performed at follow-up on 20 patients showed mild degenerative changes in 13 of 20 ankles with OLT. No correlation was found between the presence of degenerative changes and the clinical outcome. We conclude that:
Non-surgical management of stage 5 OLT is a viable option with little or no risk of developing significant osteoarthritis. Most lesions remain radiographically stable. There is a poor correlation between changes in lesion size and clinical outcome. However, the few patients with lesions which decrease significantly in size tend to do well and those with lesions which increase significantly in size do poorly. The development of mild radiographic changes of OA does not correlate with clinical outcome. The general course of stage 5 OLT is benign with over half of the patients improving to good or excellent results with non-surgical management. Lateral lesions tend to do better than medial ones. Adult onset lesions tend to do better than juvenile onset lesions.
INTRODUCTION
Osteochondral lesions of the talus (OLT) are a relatively common cause of chronic post traumatic ankle pain that can pose a diagnostic and management challenge. Many current studies are based on plain X-rays 2,4,11,12,13 and include all types of lesions. It is now clear that plain X-ray is inadequate when assessing OLT. 1,9,10 Tomogram, CT scan, and MRI have allowed us to recognize that up to 77% of chronic OLT are radiolucent defects. 1,5,7,9,10,14,15 These lesions do not fit into the Berndt and Harty 4-stage classification system (Fig. 1) 3 and we have, therefore, designated them as stage 5 (Fig. 2). 9 Many have been found to arise from lower stage (acute) Berndt and Harty lesions 1,3,7,9,10 and their pathology has been described as fibrous 9 with granulation 5,9 and small bone fragments. 15 The literature contains multiple reports on the results of surgical treatment for OLT but no reports could be found which dealt exclusively with stage 5 lesions and none on non-surgical treatment. We therefore undertook this study to determine the outcome of non-surgical treatment of stage 5 OLT.
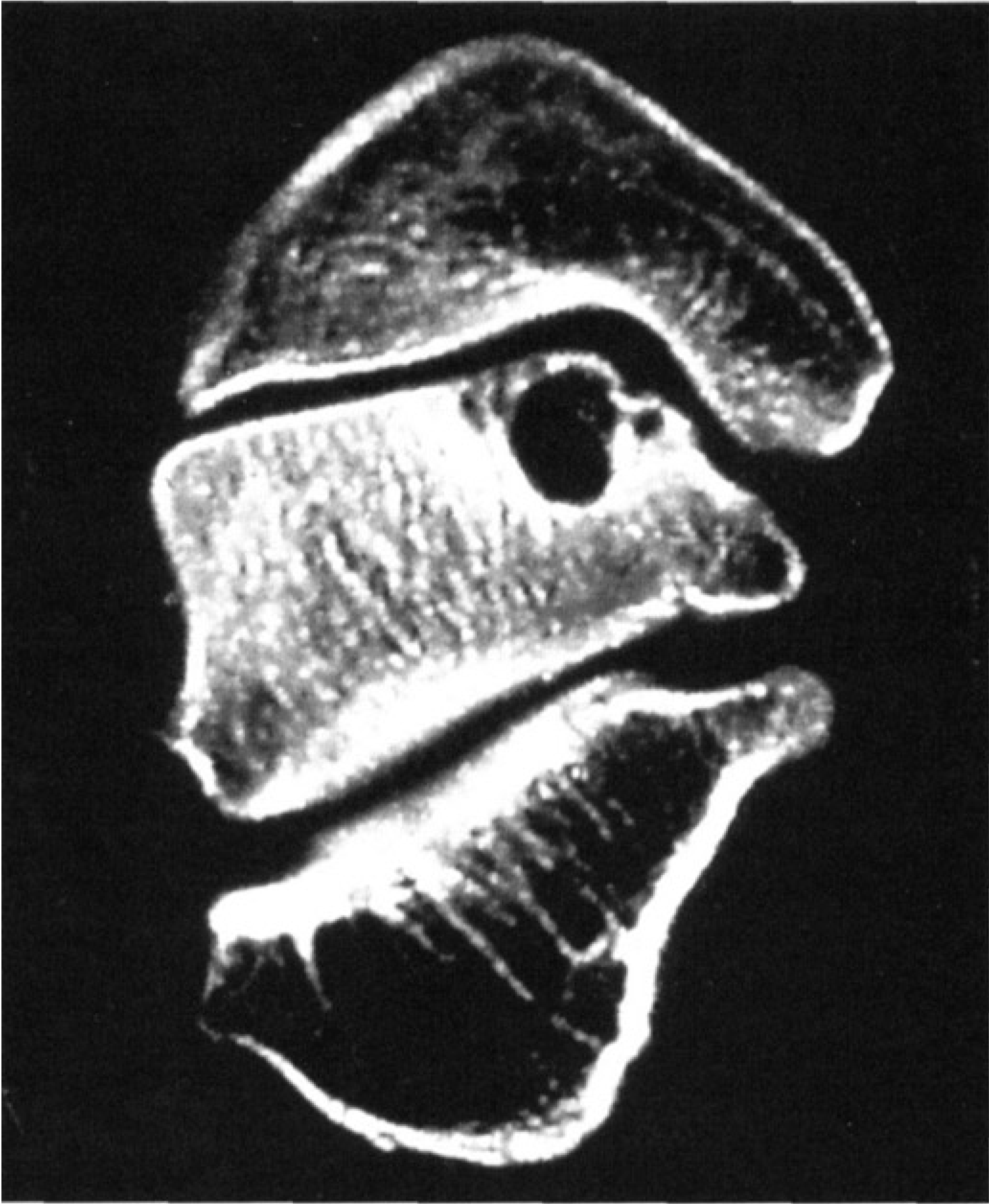
Example of a stage 5 OLT.
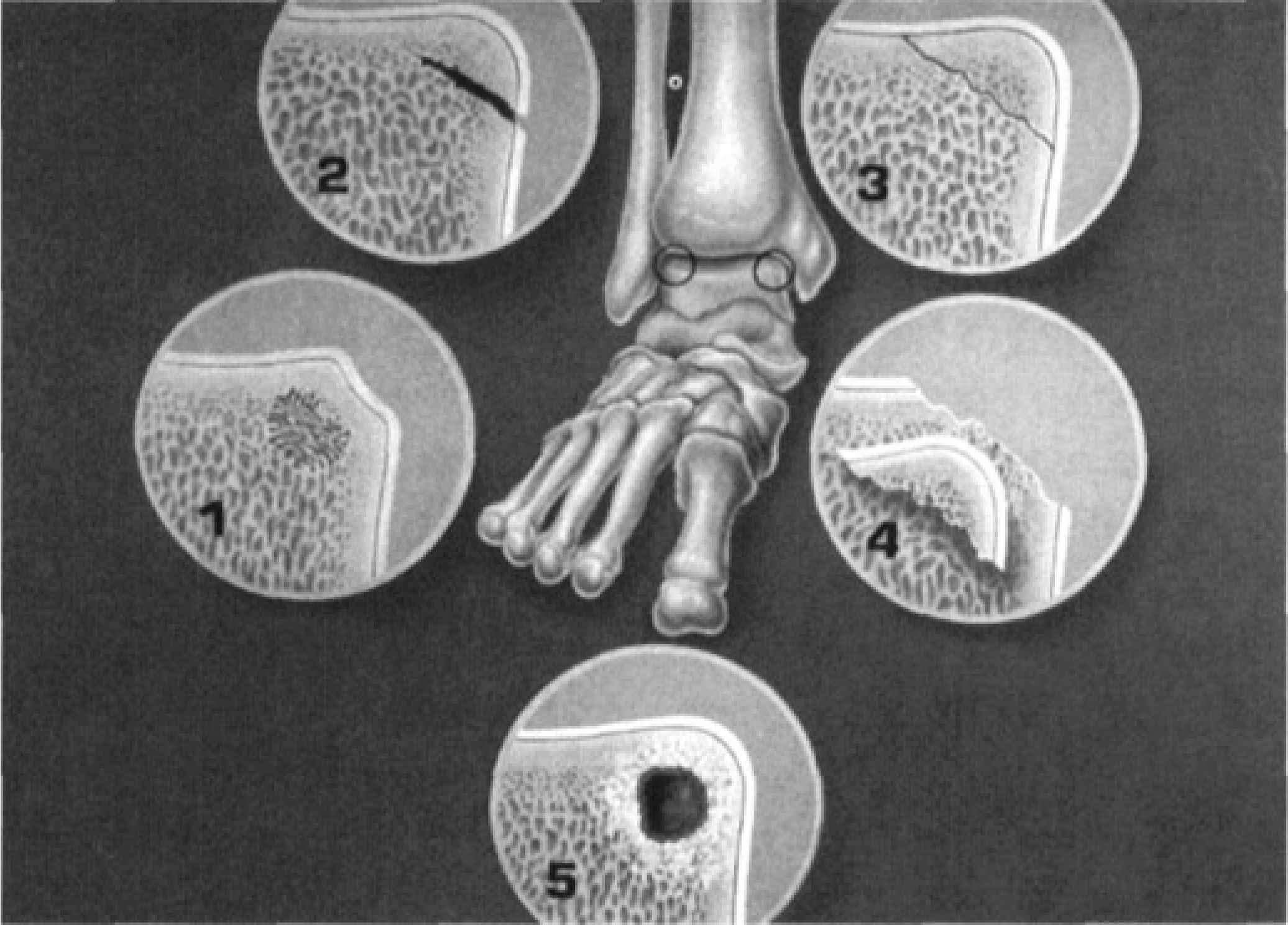
5-Stage OLT Classification System.
MATERIALS AND METHODS
Subjects were selected from our senior author's files and were considered eligible if they were at least two years post diagnosis of a symptomatic stage 5 OLT and were managed non-surgically. All patients were referred from primary care physicians, sports medicine physicians, or orthopedic surgeons and had had trials of various non-surgical means including activity modification, NSAIDs, orthotics, braces and physiotherapy. They were informed of the alternatives and likely consequences of surgical and non-surgical treatment and chose non-surgical treatment. Subsequent non-surgical treatment by the senior author consisted of “benign neglect” with the advice that they could continue with all activities as tolerated.
A clinical result was determined based on symptom persistence, sport limitation, and pain frequency according to the criteria in Table 1. Any subject subsequently opting for surgical treatment was given a poor result.
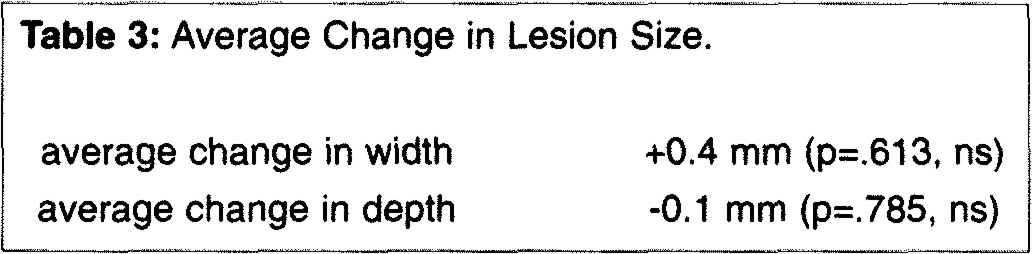
Imaging: Maximal lesion width and depth in the coronal plane were calculated using scales on the CT scans or magnification factors as suggested by the radiologists for the tomograms. A change in size of twice the standard deviation represented a significant size change with 95% confidence limits. The average width and depth at the time of diagnosis were compared to those at follow-up by repeat measure t-test. 6
Twenty-five subjects had had CT scans or Tomograms at the time of diagnosis which were of sufficient quality to permit comparison with the follow-up CTs. The typical chronic OLT is a well defined, mildly irregular radiolu-cency with or without sclerotic borders and occasionally bone fragments within or adjacent to the defect.
Clinical Result Determination.
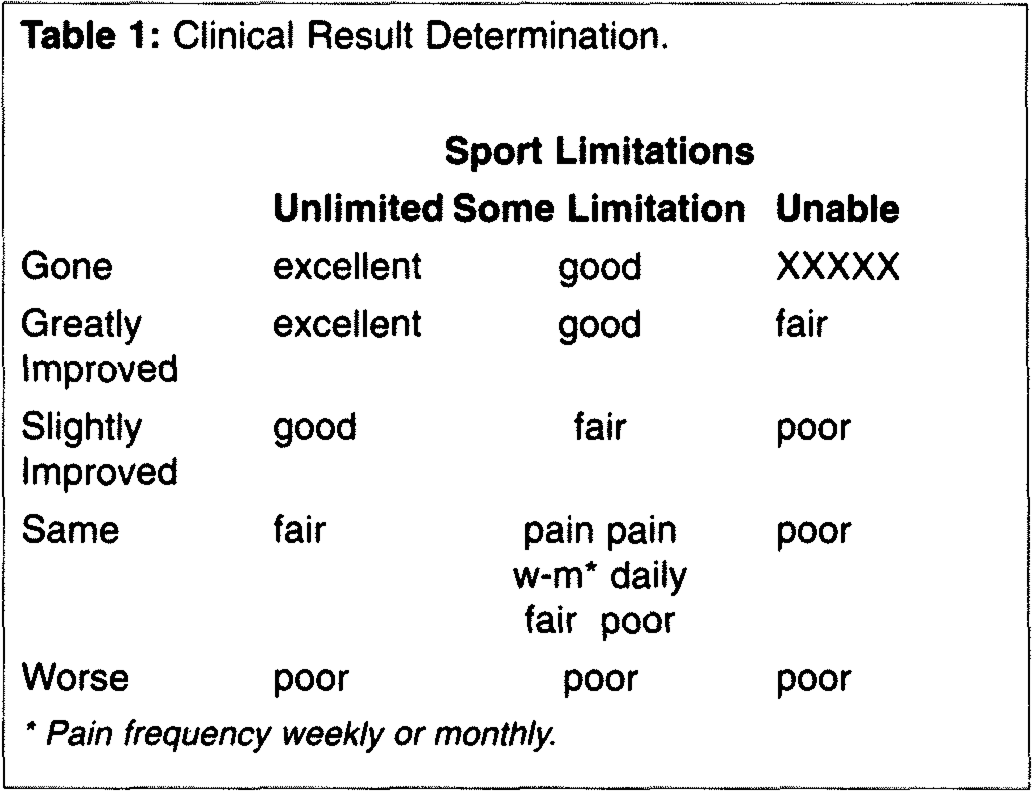
Pain frequency weekly or monthly.
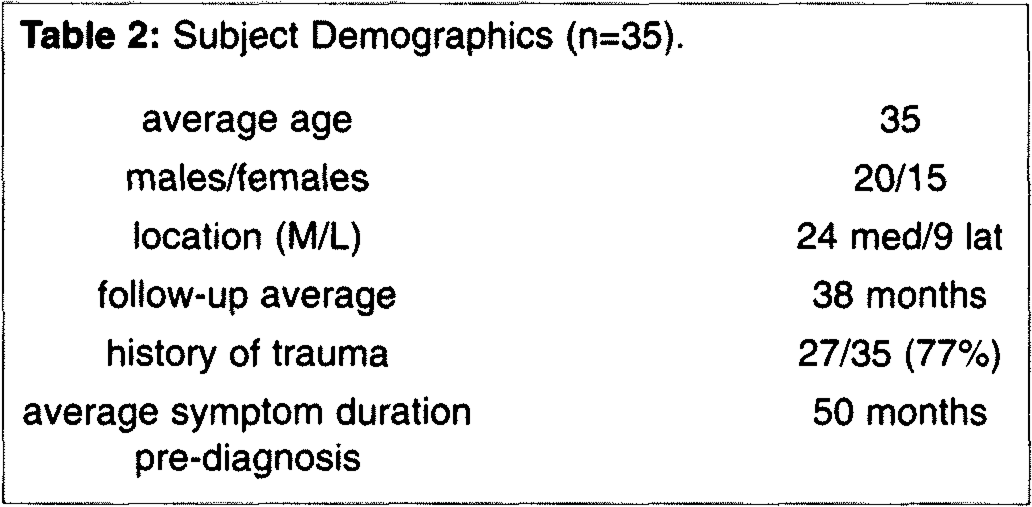
Subject Demographics (n = 35).
Average Change in Lesion Size.
Degenerative changes were considered present if X-ray revealed tibial, fibular, or talar osteophytes, subchondral sclerosis, or joint space narrowing. The clinical result in cases with and without degenerative changes was compared to determine the relationship between the development of OA and clinical results.
The clinical result was analyzed with respect to significant changes in lesion size, location of lesion (medial vs. lateral), and age of subject at diagnosis (juvenile if less than 20 years at diagnosis, adult if 20 years or greater).
SUBJECTS
Forty-one patients were identified who were at least two years post diagnosis and conservatively managed. Thirty-five ankles in 34 subjects were contacted and all agreed to participate for an 83% retrieval rate. The average time from diagnosis to follow-up was 38 months (range, 17 to 85 months). Five of the six patients who opted for surgery had less than 24 months of follow up. The average time from symptom onset to diagnosis was 50 months (range, four to 252 months). Demographic data is presented in Table 2.
There were 24 medial and nine lateral lesions (two subjects had both a lateral and a medial lesion in the same ankle and are therefore excluded from this section). Eight of nine lateral lesions (89%) and 16 of 24 medial lesions (67%) gave a history of trauma at the onset of their symptoms. There were nine patients under the age of 20 at the time of diagnosis (juveniles) and 26 subjects over the age of 20 (adults).
CLINICAL RESULTS
The overall clinical results based on a combination of symptom persistence, sport limitation, and pain frequency was 34% excellent, 20% good, 17% fair, and 29% poor. For purposes of clarity we shall hereafter combine excellent and good grades into a single number.
Clinical Results and Age at Diagnosis
The nine juvenile subjects had 33% excellent or good, 11% fair, and 56% poor results. The 26 adults had 62% excellent or good, 15% fair, and 23 % poor.
Clinical Result and Lesion Location
The 24 subjects with medial lesions had 50% excellent or good, 17% fair, and 33% poor results. The nine subjects with lateral lesions had 78% excellent or good, no fair, and 22% poor results.
Changes in Lesion Size
Six lesions were found to increase significantly in size and two lesions were found to decrease significantly in size. The remainder of the lesions were the same size at the time of follow-up.
Changes in Lesion Size and Clinical Result
The six subjects with a significant increase in lesion size had one excellent, one fair, and four poor results. The two subjects with a significant decrease in lesion size both had excellent results.
Eight subjects with follow-up CT scans had complete resolution of their symptoms. One of these eight had complete and one had partial radiographic resolution of their lesions. The remaining six had no significant change in lesion size. Six of these eight had returned to 100% of pre-injury activity level.
Radiographic Changes of OA
We found plain X-rays to be superior to CT scans in determining the presence of OA. Thirteen of 20 patients X-rayed at follow-up had degenerative changes. Most of these were minor, consisting of a tiny osteophyte with or without sclerosis. Three subjects had more significant radiographic evidence of OA with narrowing or large osteophytes.
Clinical result and degenerative changes
The 13 subjects with degenerative changes had 62% excellent or good, 23% fair, and 15% poor results. The seven subjects with no degenerative changes had 57% excellent or good, no fair, and 43% poor results. Of the three subjects with more significant degenerative changes one was excellent, one fair and one poor.
DISCUSSION
Data from our series of 220 OLT show 77% to be chronic, i.e., stage 5 lesions. 9,16 Typical stage 5 lesions present with chronic activity related pain following an inversion injury. Plain X-rays can miss 50% of these lesions 9 and bone scan, Tomogram, CT or MRI are often required. The 4-stage Berndt and Harty OLT classification system (Fig. 1) has been generally accepted by the orthopedic and sports medicine communities. However, the relatively common radiolucent talar dome defect does not fit into this system. We feel that the 5-stage classification system (Fig. 2) is more appropriate as we have found radiolucent defects arising from stage 1, 2, 3 and even stage 4 lesions.
We arbitrarily chose the age of 20 to divide juvenile from adult lesions because of the long time from symptom onset to diagnosis (average 50 months). We have no explanation for the trend towards poorer results in the juvenile patients except perhaps their higher level of expectations.
Lateral lesions tend to do better than medial ones. This contradicts previous author's findings; however they did not describe exclusively chronic lesions.
The lack of correlation between change in lesion size and result suggests that we do not yet understand the relationship between the presence of OLT, its change in size, and symptoms of pain and swelling.
We decided to accept the presence of minimal osteophytes as well as subchondral sclerosis, and narrowing as sufficient criteria for OA. We realize that this is controversial but we were interested in knowing whether the presence of even minimal degenerative change was related to the result. We found no relationship between the clinical result and these minor degenerative changes. This lack of relationship holds true even for the three cases with more significant radiographic OA.
The average follow-up of 38 months post diagnosis—88 months post symptom onset—is perhaps a bit short to draw conclusions about the natural history of stage 5 OLT considering that a similar condition in the knee (osteochondritis dissecans) can appear benign three-years after diagnosis and still lead to significant osteoarthritis later in life. 8 In our experience with stage 5 OLT dating back to 1982, no patient has returned requesting treatment beyond that described here. To our knowledge no fusions have been carried out for any of them. 16 We realize that longer term follow-up is necessary to determine if these minor changes will progress to clinically significant osteoarthritis.
Since the only universal symptom of stage 5 OLT is pain, and functional impairment was usually restricted to sports, our clinical rating scale reflected this. We looked at other foot and ankle scores but all were for patients and conditions with much more impairment than ours and we therefore found them unusable.
Treatment Recommendation
We recommend the patient consider initial non-surgical management for stage 5 lesions unless symptoms are disabling or if the CT scan shows a loose body. We explain to the patient that the likelihood of developing disabling OA is very low and that we have no reason to believe this risk would be decreased by surgery.
CONCLUSIONS
We conclude that:
Non-surgical management of chronic stage 5 OLT is a viable option with 54% good and excellent results and little or no risk of developing significant osteoarthritis (OA), Most lesions remain radiographically stable, There is a poor correlation between changes in lesion size and clinical outcome, The development of mild radiographic changes of OA does not correlate with clinical outcome, The general course of stage 5 OLT is benign with over half of the patients improving to good or excellent results with conservative management, Lateral lesions tend to do better than medial, and Adult onset lesions tend to do better than juvenile.