
Abstract

Intravascular papillary endothelial hyperplasia is an unusual lesion typically seen in the upper extremity, trunk, head, and neck. 4 Masson 9 described it in 1923 and regarded it as a hyperplasia of endothelial cells. Several investigators have suggested more recently that it represents an exuberant reparative response to vascular injury. 1,6 It is important to differentiate this benign lesion from malignant processes to avoid overly aggressive surgical management.
Case report
A 44-year-old woman was referred for evaluation of a recurrent painful left plantar forefoot mass which had developed insidiously over 2 years without antecedent trauma. An excisional biopsy was performed shortly after the mass had been noticed. However, the mass recurred within a few weeks and enlarged slowly over the ensuing months. It was subsequently aspirated. Three milliliters of sanguineous fluid were withdrawn, but the mass immediately reformed.
The patient complained of tenderness directly over the mass that interfered with ambulation and prevented any athletic activity. Partial relief was obtained from a soft doughnut-shaped pad placed around the border of the mass. The patient was employed as a computer specialist. There was no history of fever, chills, night sweats, or weight loss. Review of systems, family, and social history were noncontributory.
On physical examination, a compressible bluish cystic nodule, 2 cm in diameter, was located on the plantar forefoot, slightly proximal to the second metatarsal head (Fig. 1). No bruits were appreciated. The mass was fixed to the dermis and subcutaneous tissues, but not to the underlying fascia or tendons. It was painful to direct palpation. Digital pressure could decrease the size of the mass, but it immediately reformed when pressure was removed. There was no surrounding erythema or edema. No lymphadenopathy was present. The remainder of the examination was unremarkable.
Radiographs of the foot showed no mineralizations within the soft tissues. A magnetic resonance imaging scan taken with and without gadolinium administration was obtained which showed a 2-cm heterogeneous plantar mass (Figs. 2 and 3) confined to the subcutaneous plantar soft tissue. The nodules demonstrated low signal on T2-weighted images and intermediate signal on T1-weighted sequences.
An excisional biopsy (Fig. 4) was performed. The defect was closed primarily. Microscopically, a benign-appearing fibrous stroma surrounded dilated vascular spaces (Fig. 5). These spaces contained endothelial-lined papillary structures composed of hylanized collagen.
Two years following removal, there has been no recurrence. She has no discomfort with ambulation and does not require an orthosis. She has returned to all athletic activities.
Discussion
Intravascular papillary endothelial hyperplasia (IPEH) is described in two forms. 4 A pure form exhibits the typical histologic picture of papillary structures composed of hylanized collagen within dilated vascular spaces. A single layer of plump endothelial cells lines the papillae. This variety is commonly subcutaneous. The mixed form shows the described microscopic findings, but an associated underlying lesion, commonly a hemangioma or pyogenic granuloma, is also present. It is intramuscular in 50% of patients. 4 A similar lesion, extravascular papillary endothelial hyperplasia, is sometimes included in this classification. It is associated with hematoma.
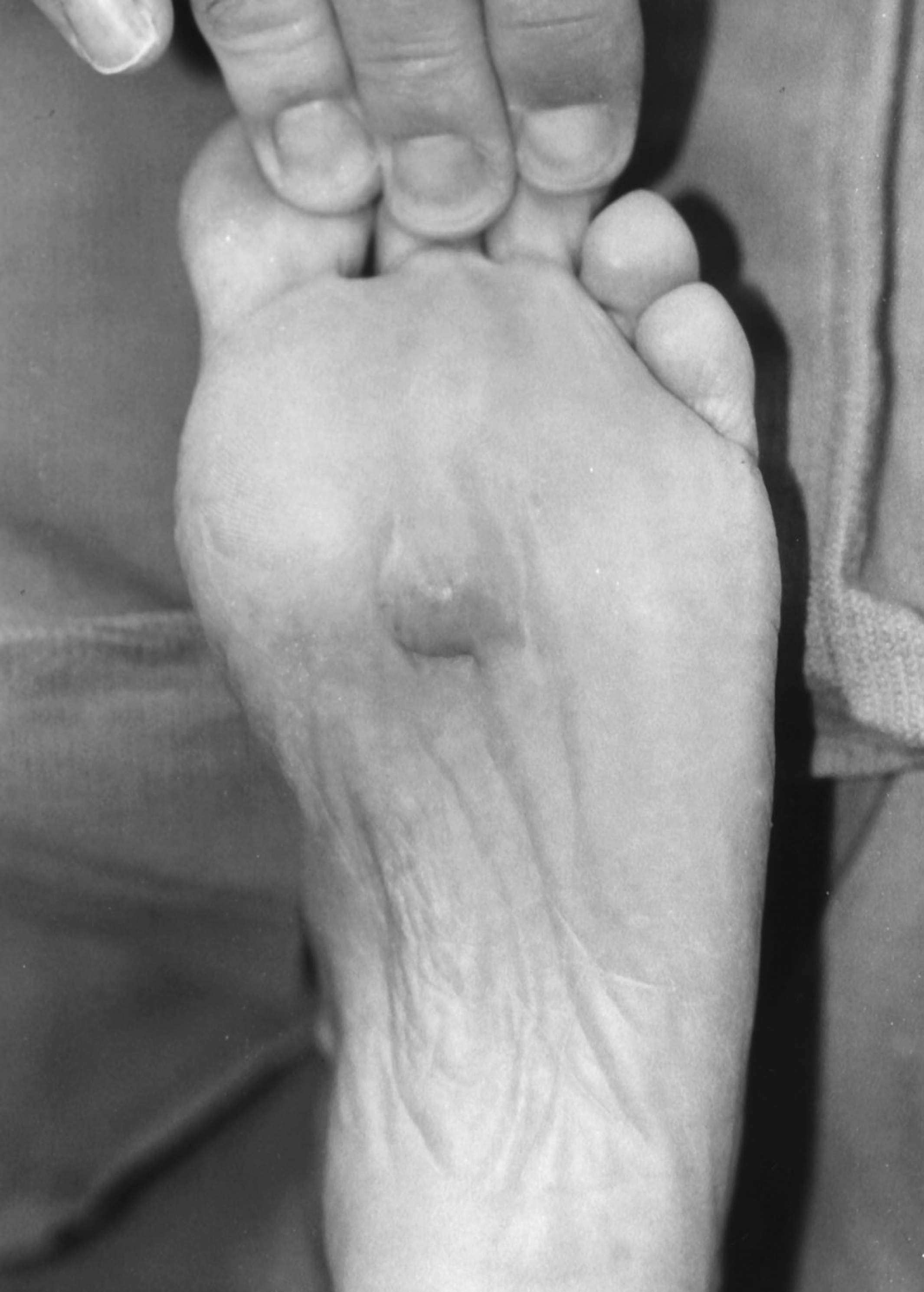
Plantar foot mass in a 44-year-old woman presenting with progressive pain over 2 years.
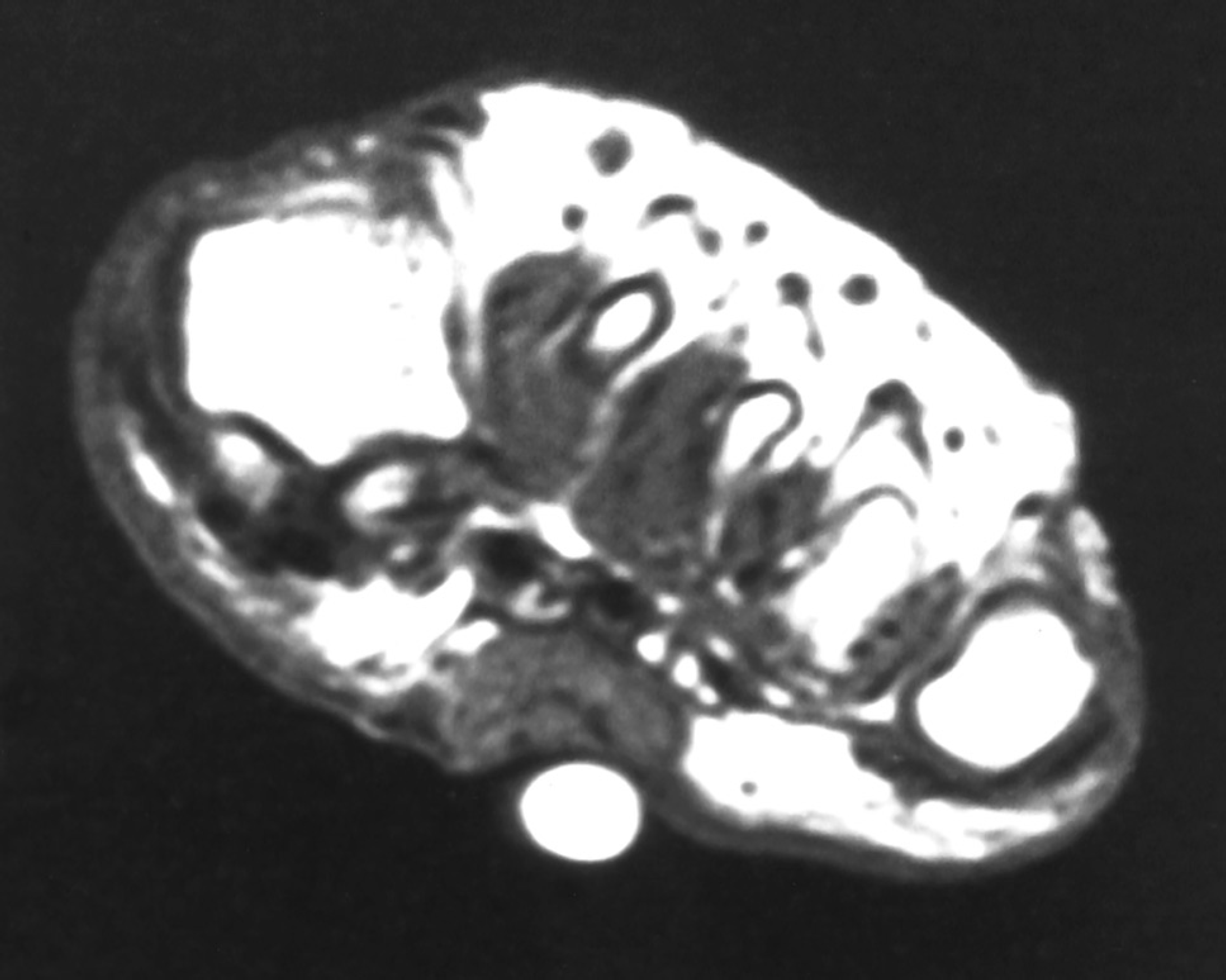
Coronal T1-weighted (TR 595 TE14) MRI image showing a discrete subcutaneous mass with intermediate signal intensity.
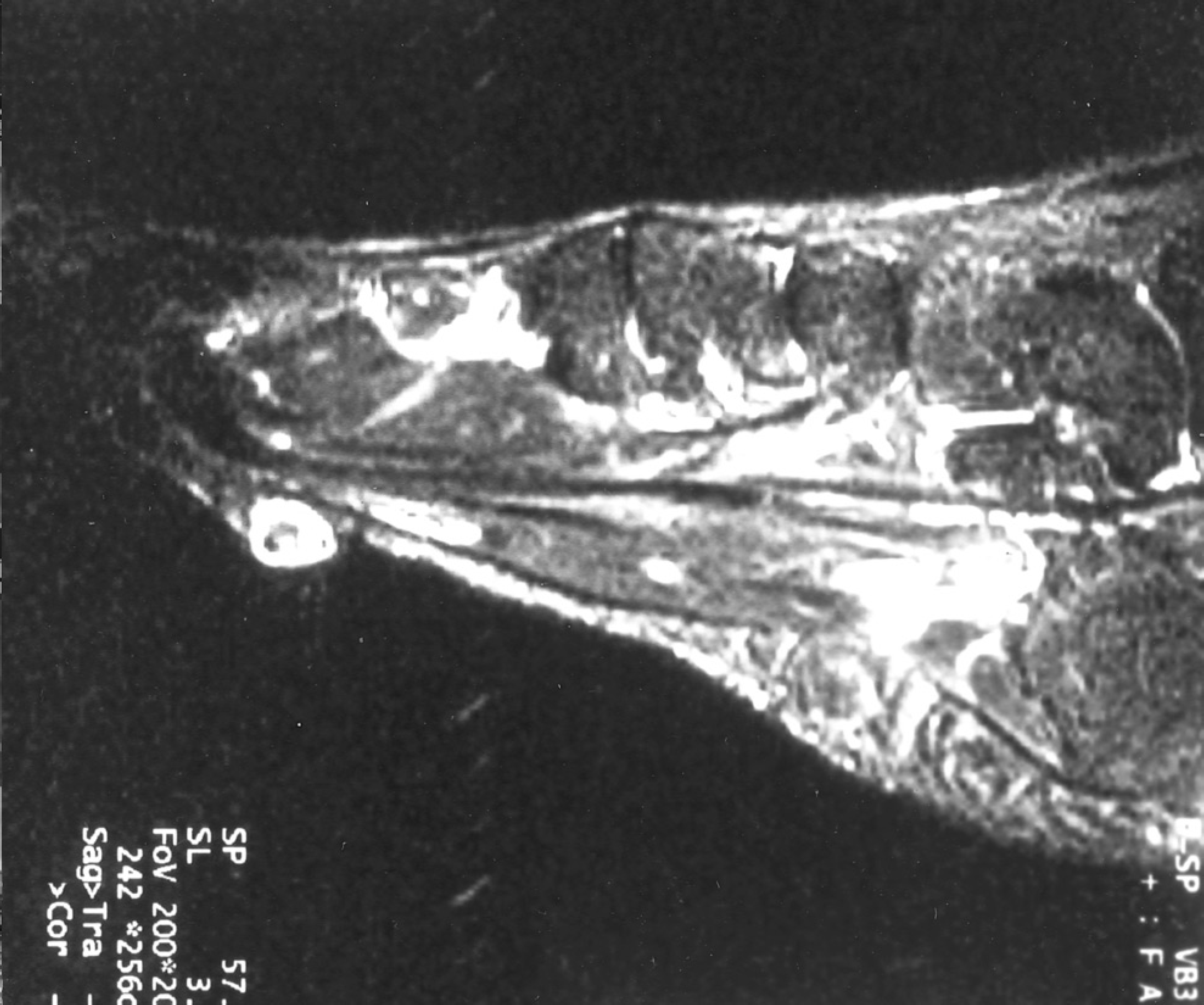
Sagittal gadolinium-enhanced T2-weighted (TR 7500 TE 60) MRI image showing peripheral enhancement of a discrete subcutaneous mass in the plantar foot.
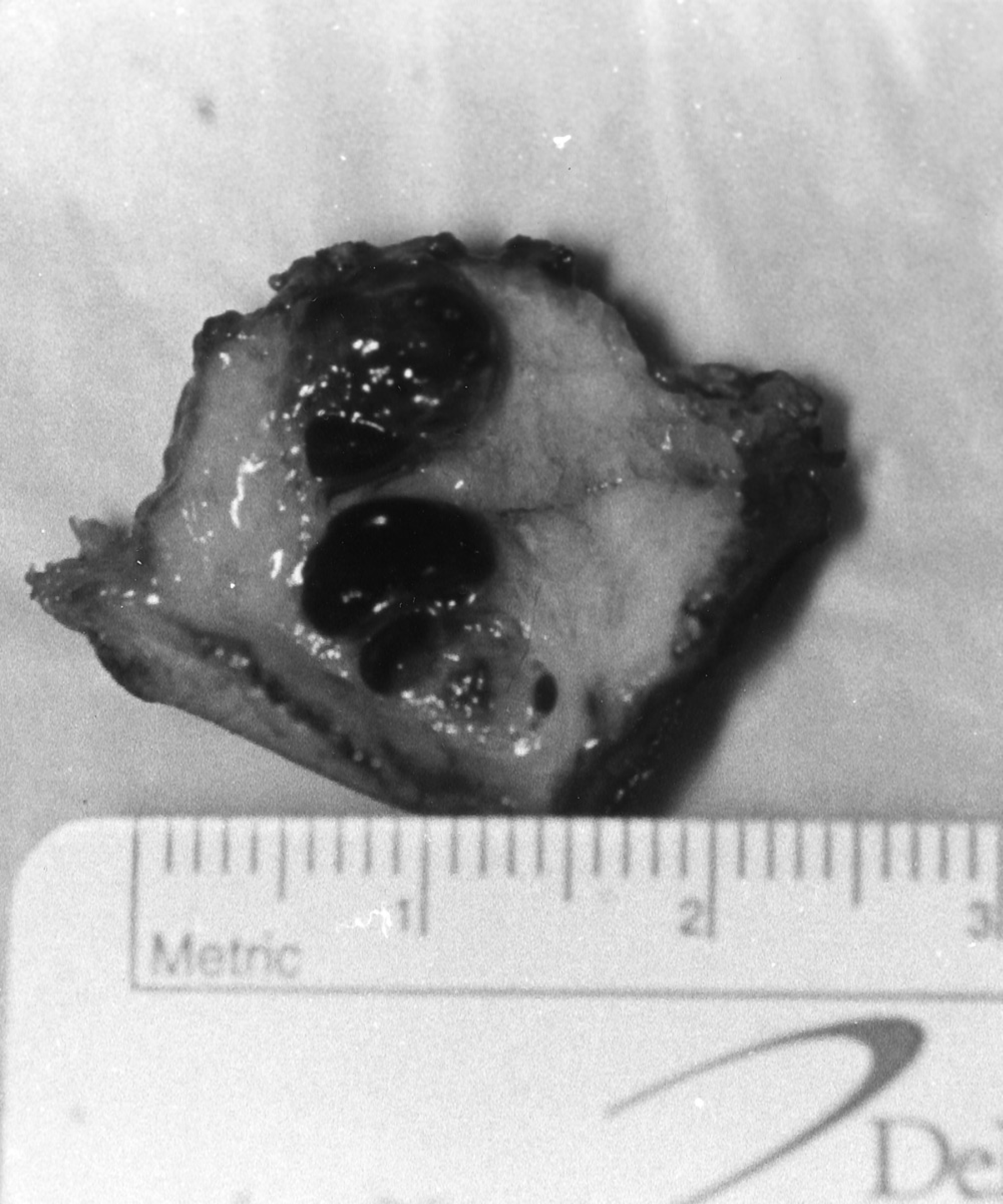
Gross specimen consisted of dense connective tissue surrounding several dilated vascular structures.
The pathogenesis of this lesion is unclear. Microscopically, it resembles granulation tissue. 6 High levels of basic fibroblastic growth factor found within IPEH lesions suggest that it may be an exuberant reparative response to vascular damage. 8 However, a history of trauma is rarely elicited in patients with this tumor. 4 In addition, although thrombus is commonly associated with IPEH, it is not universally present. Some authors have questioned whether thrombosis occurs as result of venous stasis caused by sludging from the presence of IPEH within the lumen, 10 or if the thrombus forms a matrix within which the IPEH develops. 3 Kuo 7 reported one case that developed multiple satellite lesions after excision. He observed endothelial sprouting within the recurrent lesions, which he thought represented an early form of IPEH. Multiple lesions have been reported in one case, suggesting individual susceptibility to this lesion.
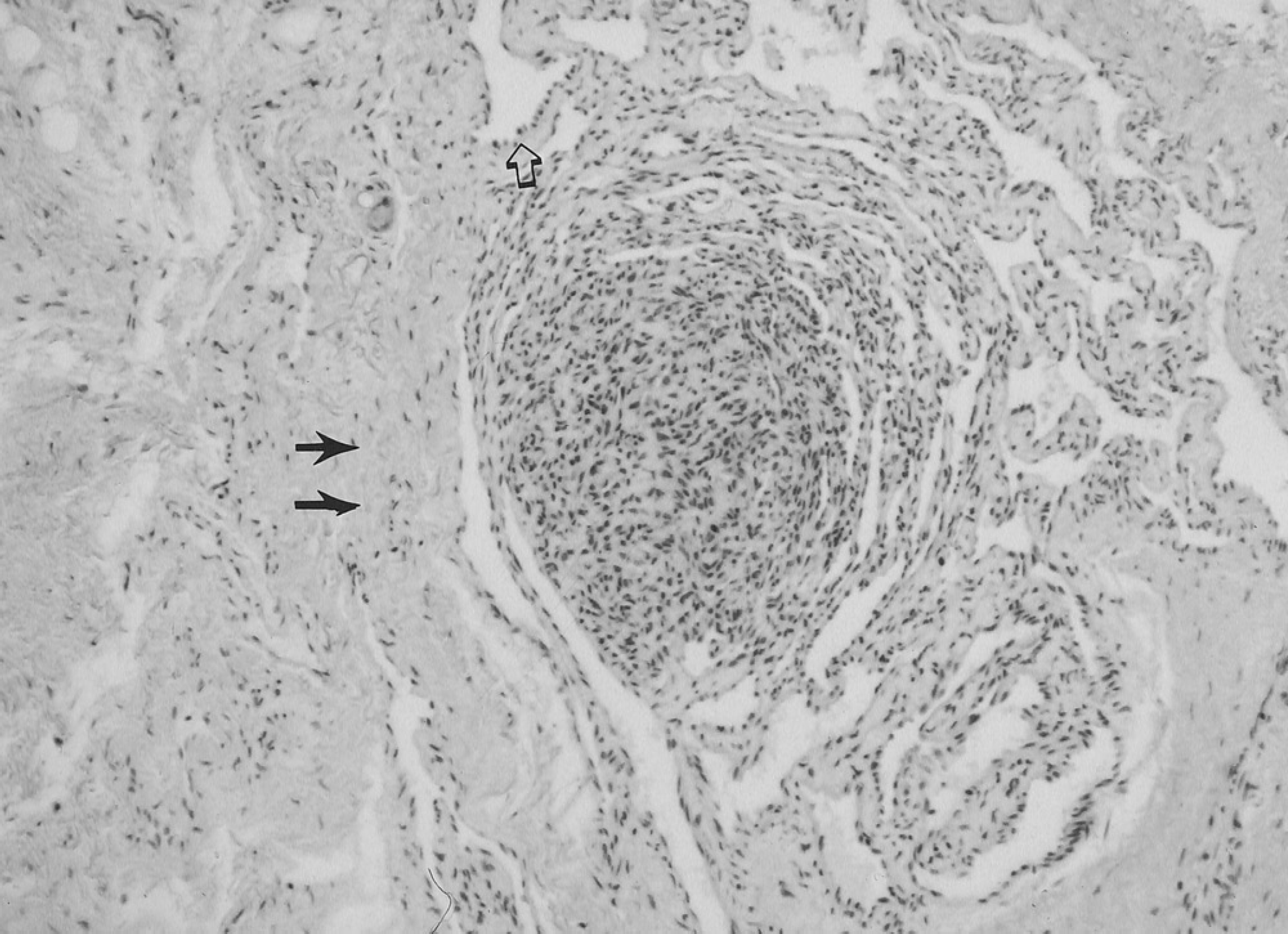
Characteristic histopathology showing areas of dense connective tissue with prominent vessels (solid arrows), endothelial lined fibrous septae and larger vascular spaces lined with a single layer of plump endothelial cells (open arrow). (Hematoxylin and eosin ×100)
Intravascular papillary endothelial hyperplasia is most commonly reported in the hand, upper extremity, trunk, head, and neck. 1,3,4 Hashimoto 4 reported three cases localized to the foot out of a total of 91 cases. Of 44 cases of IPEH, Clearkin 3 noted four in the foot. Of four case reports of IPEH in the foot, 2,5,12 three were localized to the plantar skin of the forefoot and one to the toes.
Intravascular papillary endothelial hyperplasia represents 2–4% of vascular tumors of the soft tissue. 1,4 A lack of awareness of this lesion, as well as its gross resemblance to hematoma or venous malformation, has probably led to an understatement of its incidence. The clinical appearance of this lesion suggests its vascular nature. The color can vary from reddish to purple. Other major diagnostic possibilities include venous malformation, glomus tumor, angiolymphoid hyperplasia with eosinophilia, pleomorphic hylanizing angiectatic tumor of soft parts, intravenous atypical vascular proliferation, and cutaneous angioleiomyomas. Malignant considerations include malignant melanoma, Kaposi's sarcoma, hemangioendothelioma, and, even, angiosarcoma.
Histologically, the superficial resemblance of IPEH to angiosarcoma has given it the pseudonym “Masson's pseudoangiosarcoma.” However, IPEH rarely demonstrates the malignant clinical characteristics of angiosarcoma. 1 Ulceration, necrosis, and local satellite metastases characteristic of angiosarcoma are rarely seen in IPEH. Microscopically, the differentiation can usually be made from its lack of malignant features. Pleomorphism is minimal and mitoses are rare. Necrosis is uncommon, and there is no evidence of infiltration of extravascular tissue.
Although spontaneous resolution has been reported, 11 the lesions can persist for several years. 4 In a series reported by Hashimoto, 4 33% of lesions were painful. Therefore, complete surgical excision is recommended for diagnosis and definitive treatment. Recurrence was noted in 8% and is more common in the mixed form. This may be related to incomplete excision of the underlying lesion. Distant metastases have not been reported.
Intravascular papillary endothelial hyperplasia is a benign process that presents as a chronic vascular mass that is sometimes painful. When seen in the foot, it is commonly located within the plantar skin. It may represent an overly exuberant reparative response to thrombosis or a hyperplasia of endothelial cells. It can be confused histologically with angiosarcoma and other vascular tumors, but can be differentiated by its benign clinical course and cytologic characteristics. Surgical excision is generally curative, but recurrence is not uncommon.