
Abstract
Glomus tumors may present as either diffuse pain in the area of the nailbed or as very localized acute pain experienced when pressure is applied with a pointed object such as a pen over the lesion under the nail. 1,5 -8 To date, no etiological factors in the development of glomus tumors have been identified. Despite the relative rarity of this entity, one must be aware of the possibility of glomus tumor when a patient presents with persistent pain around his or her nailbed and has experienced previous unsuccessful surgery for pain.
The differential diagnoses for this type of nail pain include melanoblastoma, melanoma, neurinoma, chronic paronychia, gout arthritis, and foreign-body granuloma. Patients with glomus tumors commonly experience temperature hypersensitivity and are especially sensitive to cold. The glomus tumor seems to be a controlled arteriovenous anastomosis or shunt between terminal vessels with the function to regulate peripheral blood flow in the digit. It is also referred to as a neurovascular nodule or a neuromyoarterial apparatus.
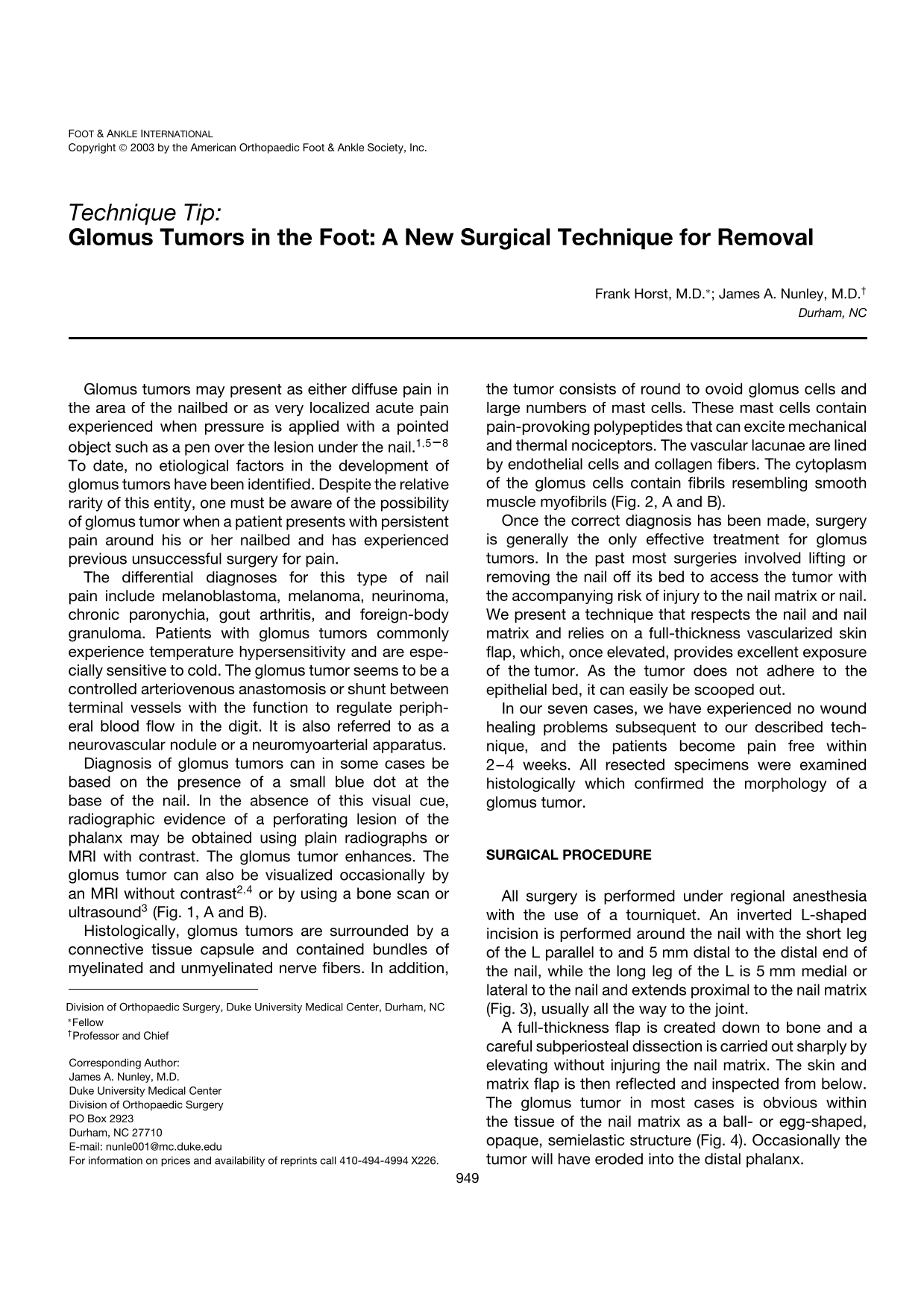
Diagnosis of glomus tumors can in some cases be based on the presence of a small blue dot at the base of the nail. In the absence of this visual cue, radiographic evidence of a perforating lesion of the phalanx may be obtained using plain radiographs or MRI with contrast. The glomus tumor enhances. The glomus tumor can also be visualized occasionally by an MRI without contrast 2,4 or by using a bone scan or ultrasound 3 (Fig. 1, A and B).
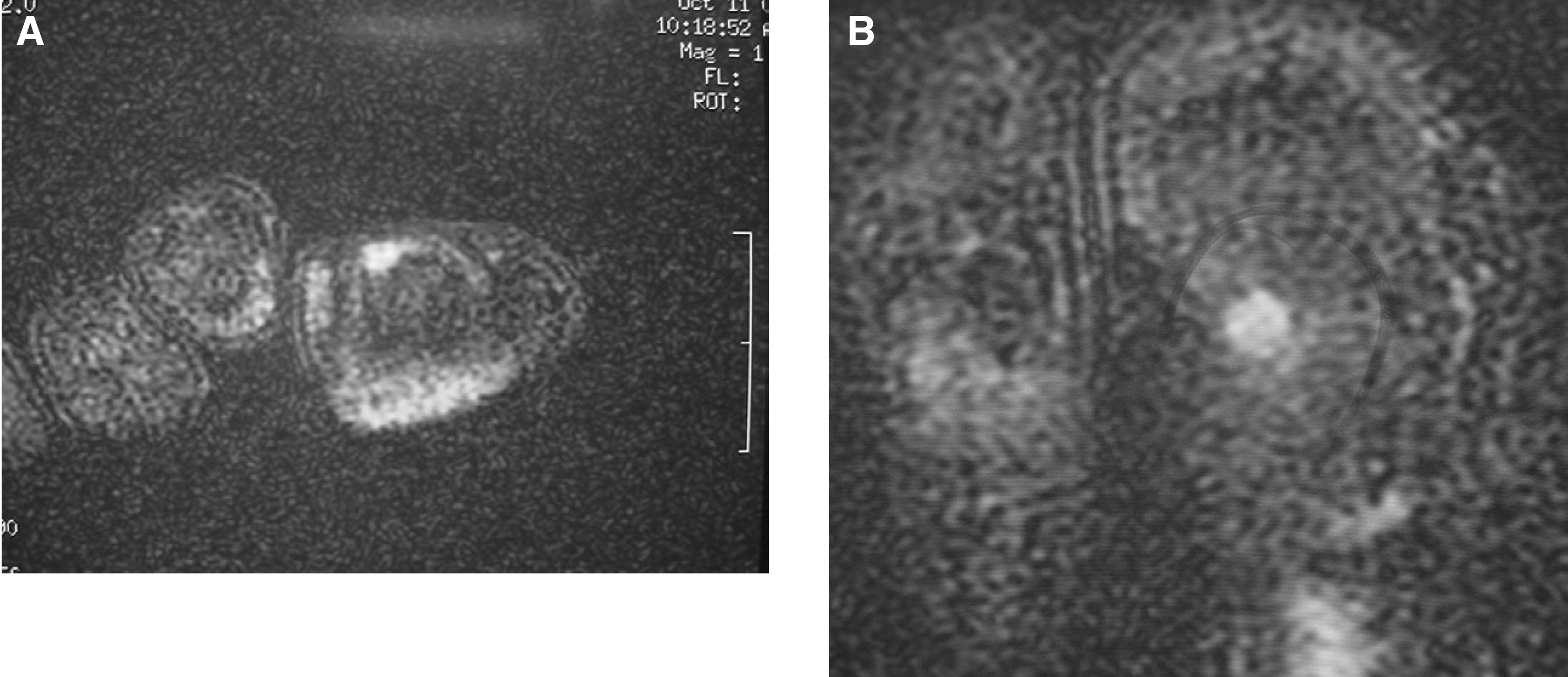
Histologically, glomus tumors are surrounded by a connective tissue capsule and contained bundles of myelinated and unmyelinated nerve fibers. In addition, the tumor consists of round to ovoid glomus cells and large numbers of mast cells. These mast cells contain pain-provoking polypeptides that can excite mechanical and thermal nociceptors. The vascular lacunae are lined by endothelial cells and collagen fibers. The cytoplasm of the glomus cells contain fibrils resembling smooth muscle myofibrils (Fig. 2, A and B).
Once the correct diagnosis has been made, surgery is generally the only effective treatment for glomus tumors. In the past most surgeries involved lifting or removing the nail off its bed to access the tumor with the accompanying risk of injury to the nail matrix or nail. We present a technique that respects the nail and nail matrix and relies on a full-thickness vascularized skin flap, which, once elevated, provides excellent exposure of the tumor. As the tumor does not adhere to the epithelial bed, it can easily be scooped out.
In our seven cases, we have experienced no wound healing problems subsequent to our described technique, and the patients become pain free within 2–4 weeks. All resected specimens were examined histologically which confirmed the morphology of a glomus tumor.
Surgical Procedure
All surgery is performed under regional anesthesia with the use of a tourniquet. An inverted L-shaped incision is performed around the nail with the short leg of the L parallel to and 5 mm distal to the distal end of the nail, while the long leg of the L is 5 mm medial or lateral to the nail and extends proximal to the nail matrix (Fig. 3), usually all the way to the joint.
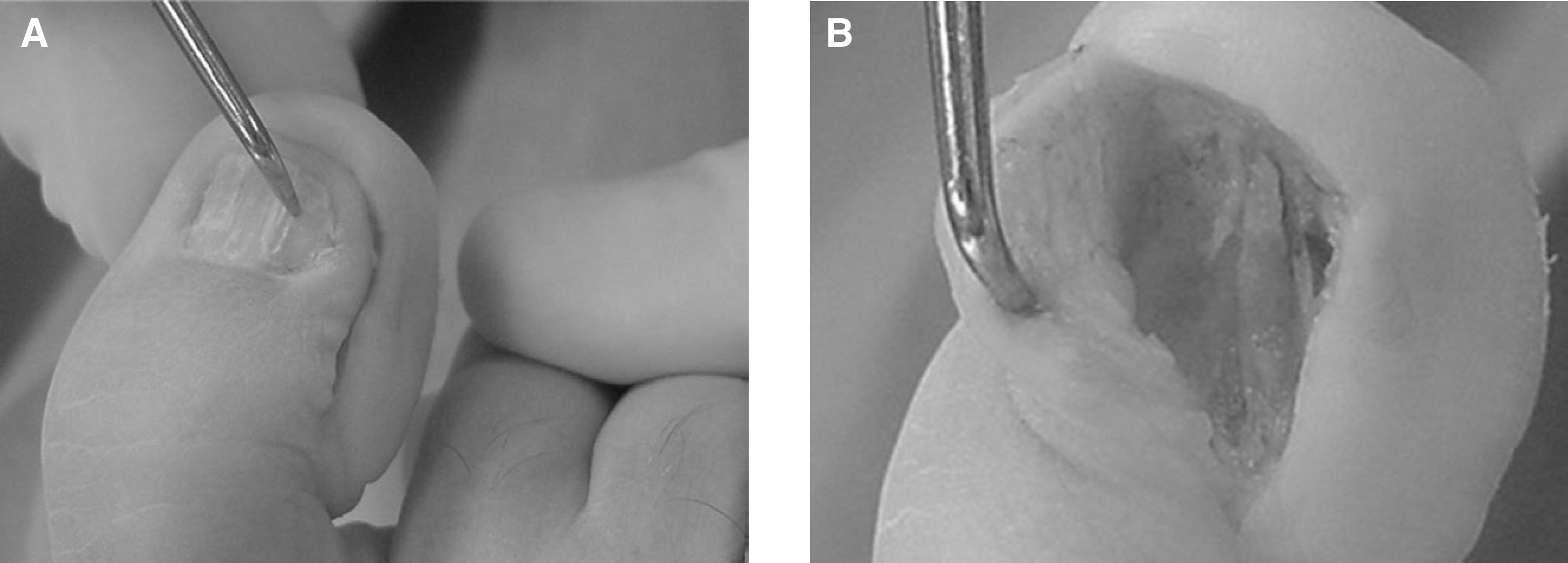
A full-thickness flap is created down to bone and a careful subperiosteal dissection is carried out sharply by elevating without injuring the nail matrix. The skin and matrix flap is then reflected and inspected from below. The glomus tumor in most cases is obvious within the tissue of the nail matrix as a ball- or egg-shaped, opaque, semielastic structure (Fig. 4). Occasionally the tumor will have eroded into the distal phalanx.
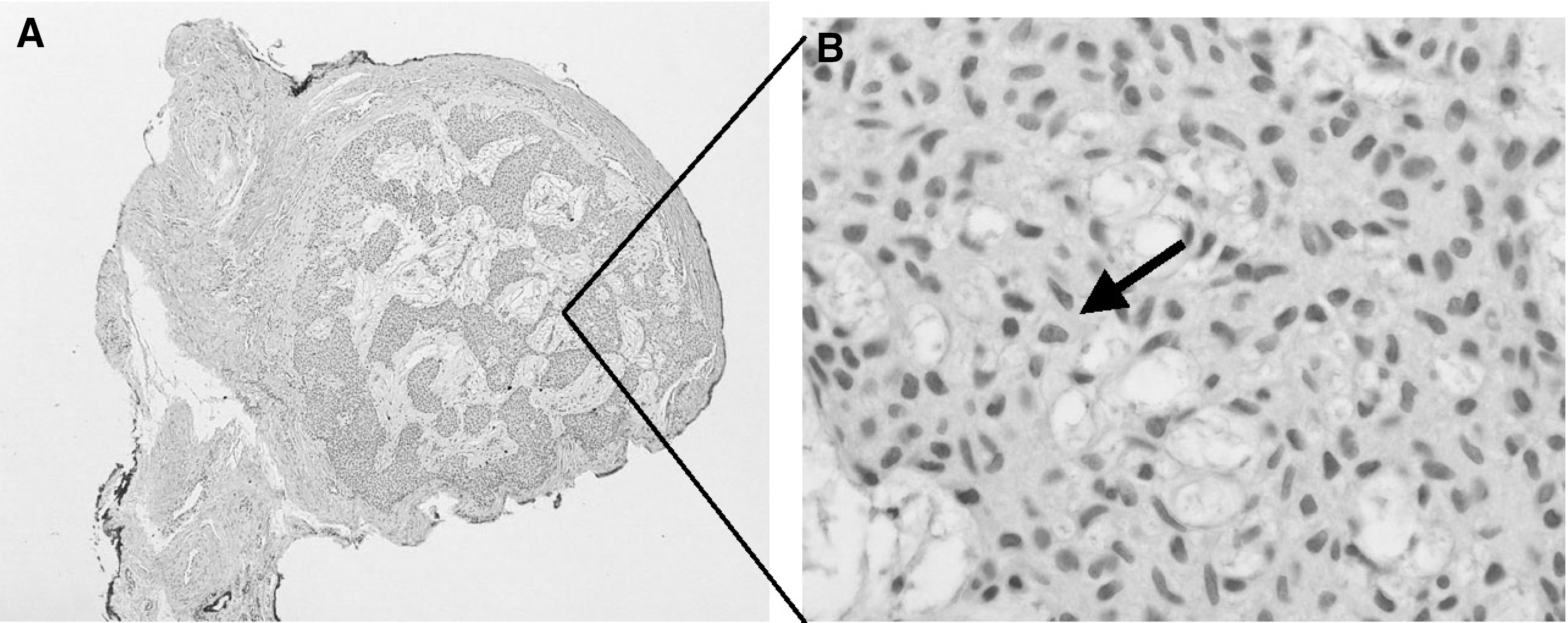
L-shaped full-thickness flap elevating the whole nail with nail matrix and glomus tumor.
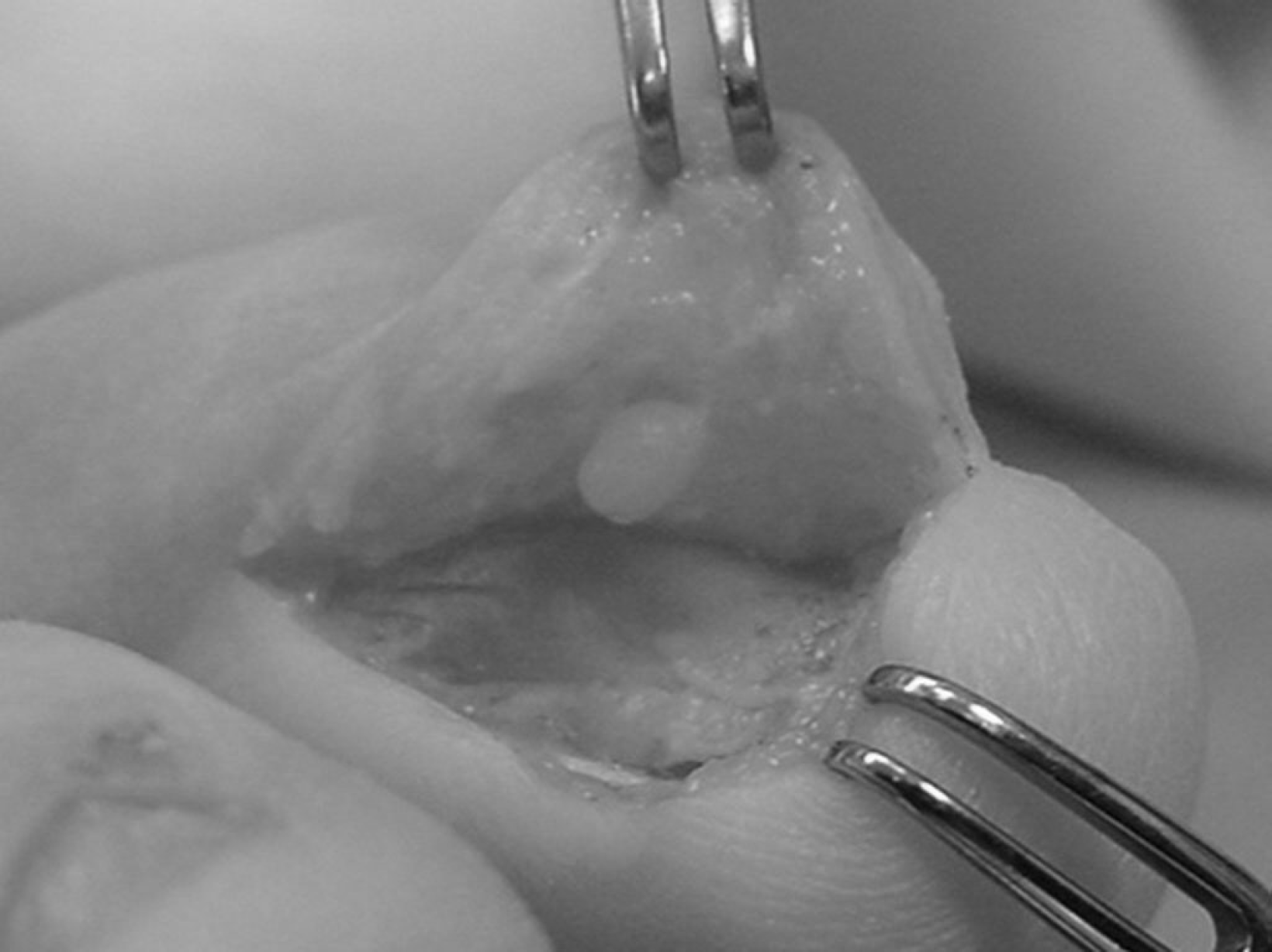
Glomus tumor in epithelial bed underneath the flap.
The tumor is normally well encapsulated and can be easily excised with a small knife or curette. The tourniquet is then released and bleeding is carefully controlled with bipolar electrocautery. The wound is closed in one layer with nylon interrupted suture, and the patient is then supplied with a hard-soled shoe for use during the wound healing period.
Patients were usually pain free to touch after 4 weeks, but all were pain free at final assessment after 3–6 months. There were no recurrent tumors in any patient and no nail irregularities occurred.