
Abstract
Hypothesis: Rheumatoid arthritis is a common disabling form of arthritis that frequently affects the hands and feet. With time, the majority of affected individuals will become disabled. Methods: Sixty-nine consecutively selected mild to moderately affected individuals with rheumatoid arthritis provided demographic data and agreed to complete the Short Musculoskeletal Function Assessment (SFMA) instrument. Focus group subjects selectively used minimally adaptive nonprescription footwear. Control subjects had similar disease expression, but did not alter their choice of footwear due to their disease. Results: Adult patients with rheumatoid arthritis demonstrate a significant negative impact on their quality of life with mild or moderate disease expression, as evidenced by poor scores in all six domains of the SFMA. Subjects who used even mildly adaptive nonprescription footwear demonstrated a statistically significant negative impact in mobility (p <.044) and functional index (p <.052) domains as compared with the control population having similar overall disease expression. Focus subjects also demonstrated a trend to less favorable scores in the arm and hand domain. Mean scores of the daily activity, emotional status, and bother index domains fared worse than population norms, but there was no statistical difference between subjects using, or not using, adaptive footwear. Conclusions: Individuals affected with mild to moderate rheumatoid arthritis are disabled as compared with the general population. There is a severe negative impact on mobility and functional capacity when the disease process begins to affect their feet.
Introduction
Musculoskeletal injury and disease affect up to 43 million people in the United States, causing serious disability and lost work time. 1 Nearly $65 billion in medical care costs and indirect expenses, such as lost wages, are a result of musculoskeletal conditions. 5 As the population grows older, musculoskeletal problems will only become more predominant. It is estimated that by the year 2020 there will be 60 million individuals in the United States with some form of arthritis. 3
Rheumatoid arthritis (RA) is a common disabling form of arthritis, greatly impacting on the lives of affected individuals, producing over 9 million physician office visits and 250,000 hospitalizations annually. 8 Within 10 years of diagnosis, 50% of all RA individuals will be unable to be fully employed, and within 20 years, 90% will be clinically disabled. 8 The disease presently affects an estimated 5 million Americans, with women being more often involved. 2 The primary onset is between a person's third and fifth decades, significantly impacting on their productive earning years. The course of the disease can be variable, but usually is progressive and chronic. Foot deformities are present in 90% of affected individuals. 2,6,12
Multimodality treatment combines medications, physical therapy, and orthotic devices. Surgery is only advised when destructive synovitis persists in spite of medical treatment or deformity severely impairs function. The disease greatly affects many facets of the individual's life. An accurate indicator of disease impact and treatment success is based on individuals' own evaluation of their self-described pain levels and their capacity to perform activities of daily living. Outcome measures have been shown to assess accurately individuals' functional limitations over time with both clinical accuracy and cost-effectiveness. 4,10,11
The goal of this study was to evaluate the daily function and health-related quality of life of individuals with RA and mild foot involvement requiring only simple footwear accommodation. This premise was based on the knowledge that individuals with multiple trauma appear to have poorer quality outcomes when their multiple injuries include foot injury. 13 The null hypothesis states that there is no significant difference in the health-related quality of life between individuals with RA comparing those individuals with foot involvement and those without foot involvement.
Outcomes Assessment Tool
Outcomes measurements are a proven valid and reliable method for testing the functional outcome of medical or surgical treatment. The data from the individual are unique because they quantify the function of the individual as a whole. This information is also unique in the fact that it is an assessment of an individual through his or her own point of view. While clinical outcomes, such as radiography or blood tests, have been the traditional method for quantifying the success of interventions, outcomes measurements should be used in combination to produce a complete conclusion. Outcomes measurement can also be used as the sole method of assessment, providing an evaluation of aspects of subjects' function, including physical function, pain, health status, work activity, activities of daily living, and emotion status. 10
The Short Musculoskeletal Function Assessment (SMFA) is a validated outcomes measurement tool shown to be reliable and valid in assessing the health status of an individual. The SMFA can be used easily in a clinical setting to provide information about several different areas of the affected individual and the disease progress. First, the SMFA provides standardized measurement of the physical limitations and the disease impact on the subject. Second, the disease impact over time can be assessed. Third, the data from one subject may be compared to other subjects or the subject population as a whole. And finally, the SMFA can be used to pool disease-specific data to evaluate the effectiveness of treatment and interventions, severity of the disease, and healthcare policies. 11 This article reports on the initial enrollment data of a population of individuals with mild to moderate disease expression, who will be followed longitudinally to determine how their disease process affects their quality of daily life.
Methods
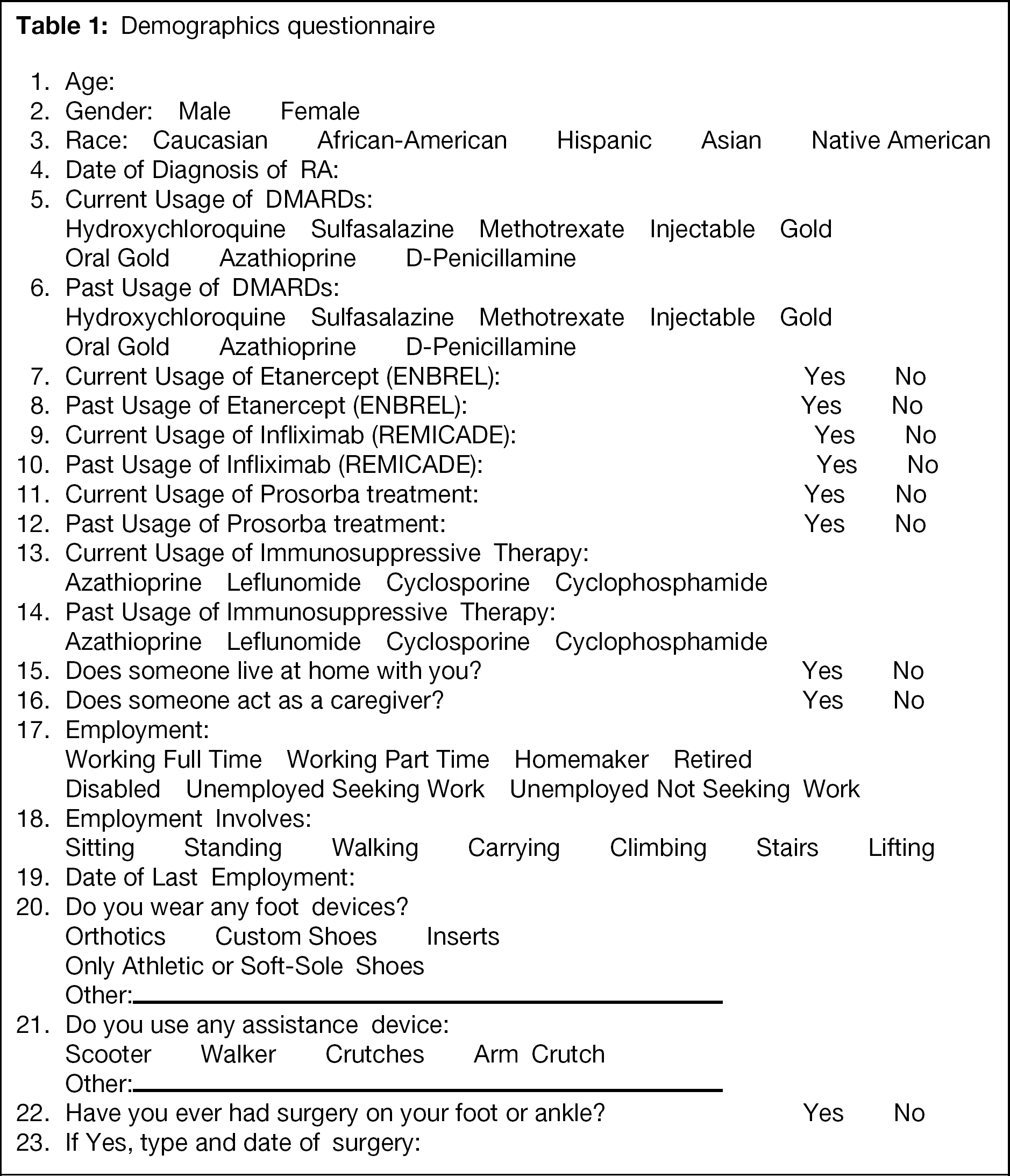
As part of a 3-year observational study, 69 consecutively selected individuals affected with RA agreed to complete the SMFA and a demographics questionnaire (Table 1) at enrollment, and annually for a minimum of 3 years. 14 Inclusion criteria included: (1) greater than 18 years of age, (2) stage 2 or 3 RA, 9 and (3) no evidence of terminal illness or cognitive-affecting diseases. The individual's disease staging was determined by the Board-certified rheumatologist (RK) responsible for the medical management of his or her disease, using the following grading scheme:
Stage 1: No destructive changes on roentgenographic examination. Radiographic evidence of osteoporosis may be present.
Stage 2: Radiographic evidence of osteoporosis, with or without slight subchondral bone destruction; slight cartilage destruction may be present. No joint deformities, although limitation of joint mobility may be present. Adjacent muscle atrophy. Extra-articular soft-tissue lesions, such as nodules and tenosynovitis may be present.
Stage 3: Radiographic evidence of cartilage and bone destruction, in addition to osteoporosis. Joint deformity, such as subluxation, ulnar deviation, or hyperextension, without fibrous or bony anklylosis. Extensive muscle atrophy. Extra-articular soft-tissue lesions, such as nodules and tenosynovitis may be present.
Stage 4: Findings of stage 3 plus joint fibrous or bony ankylosis. 9
Subjects with stage 1 disease were excluded due to usual lack of diagnosis at this early point in the disease. Subjects with stage 4 disease were excluded due to the obvious severity of disease impact in these individuals.
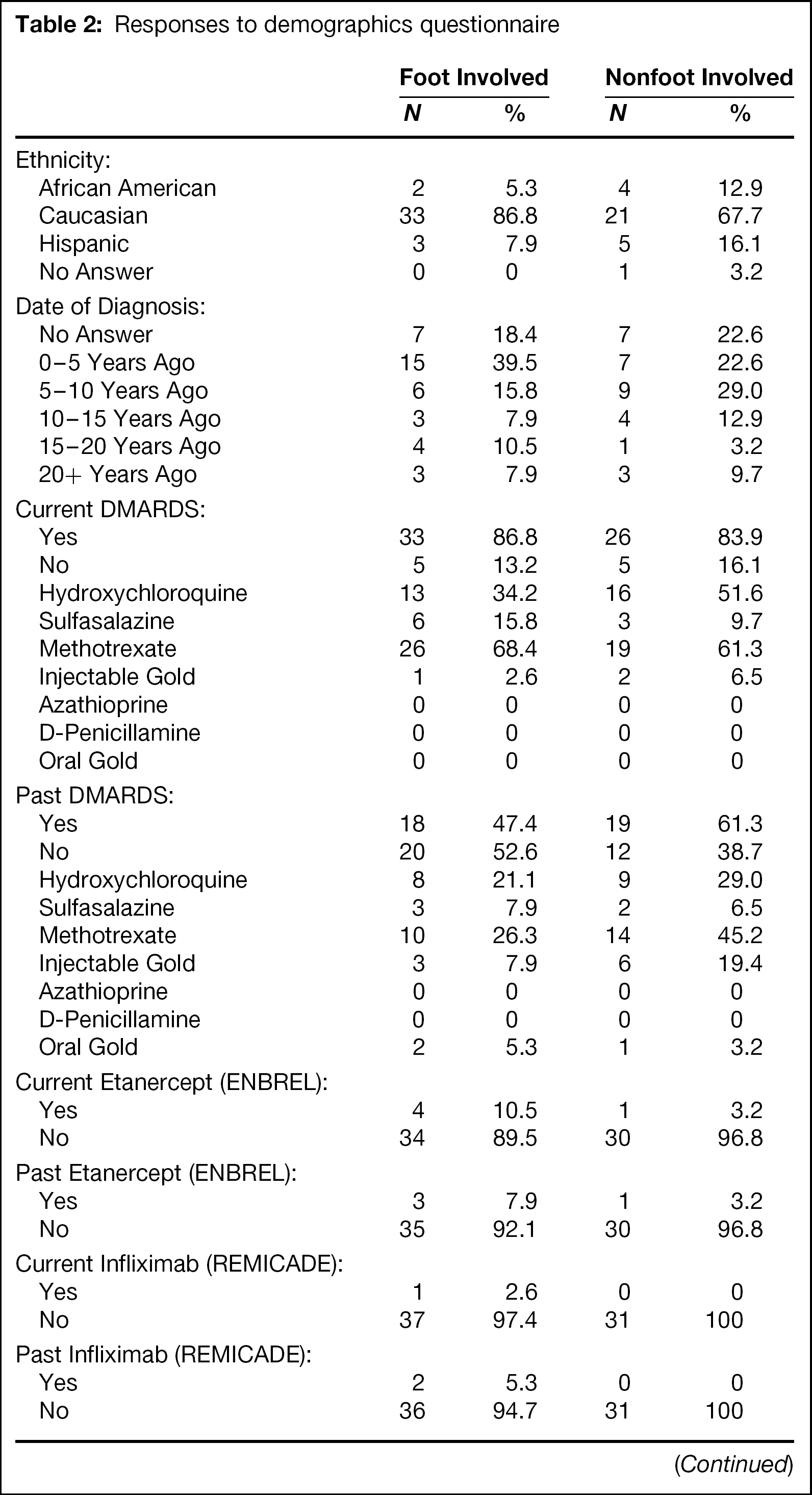
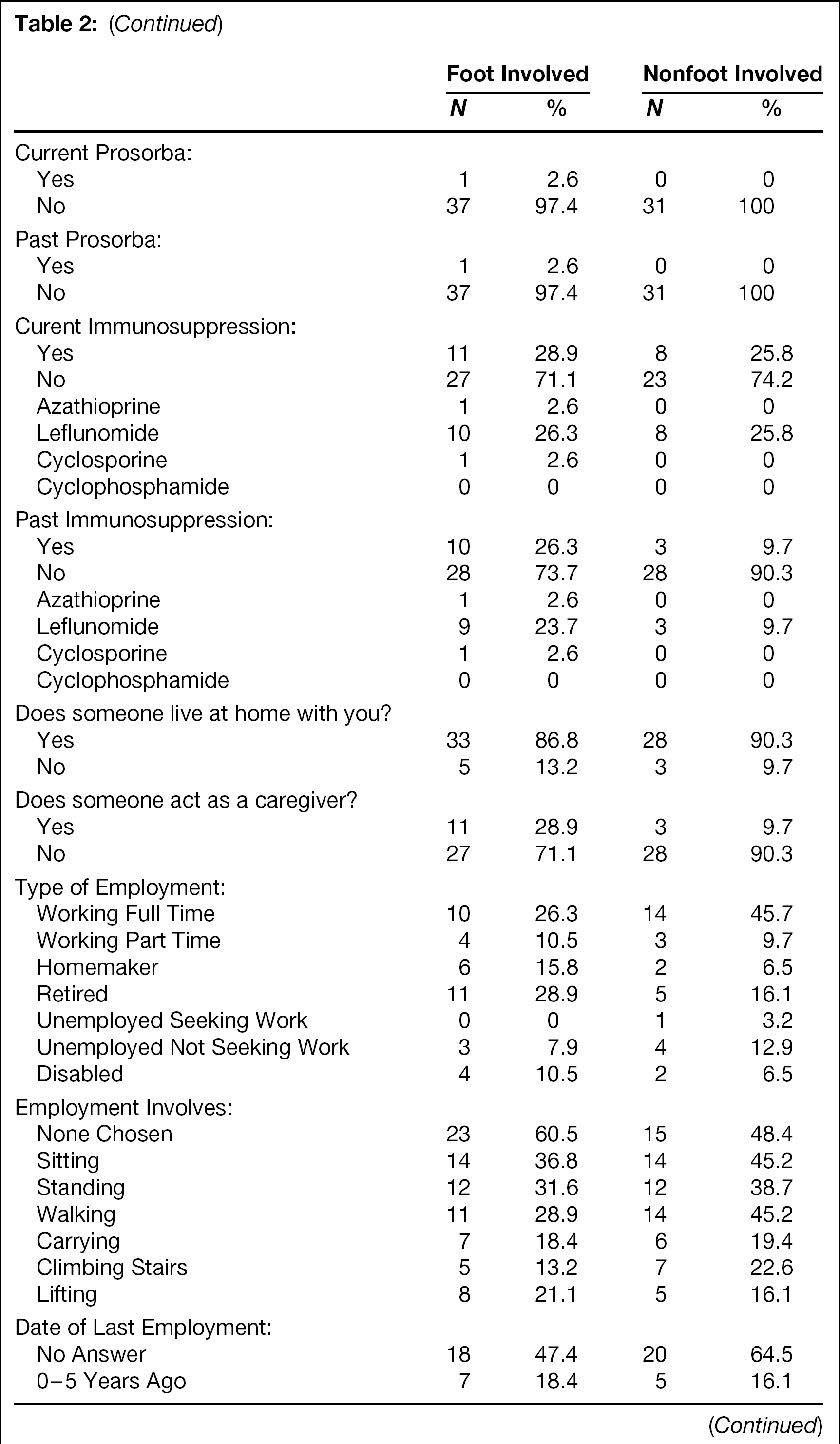
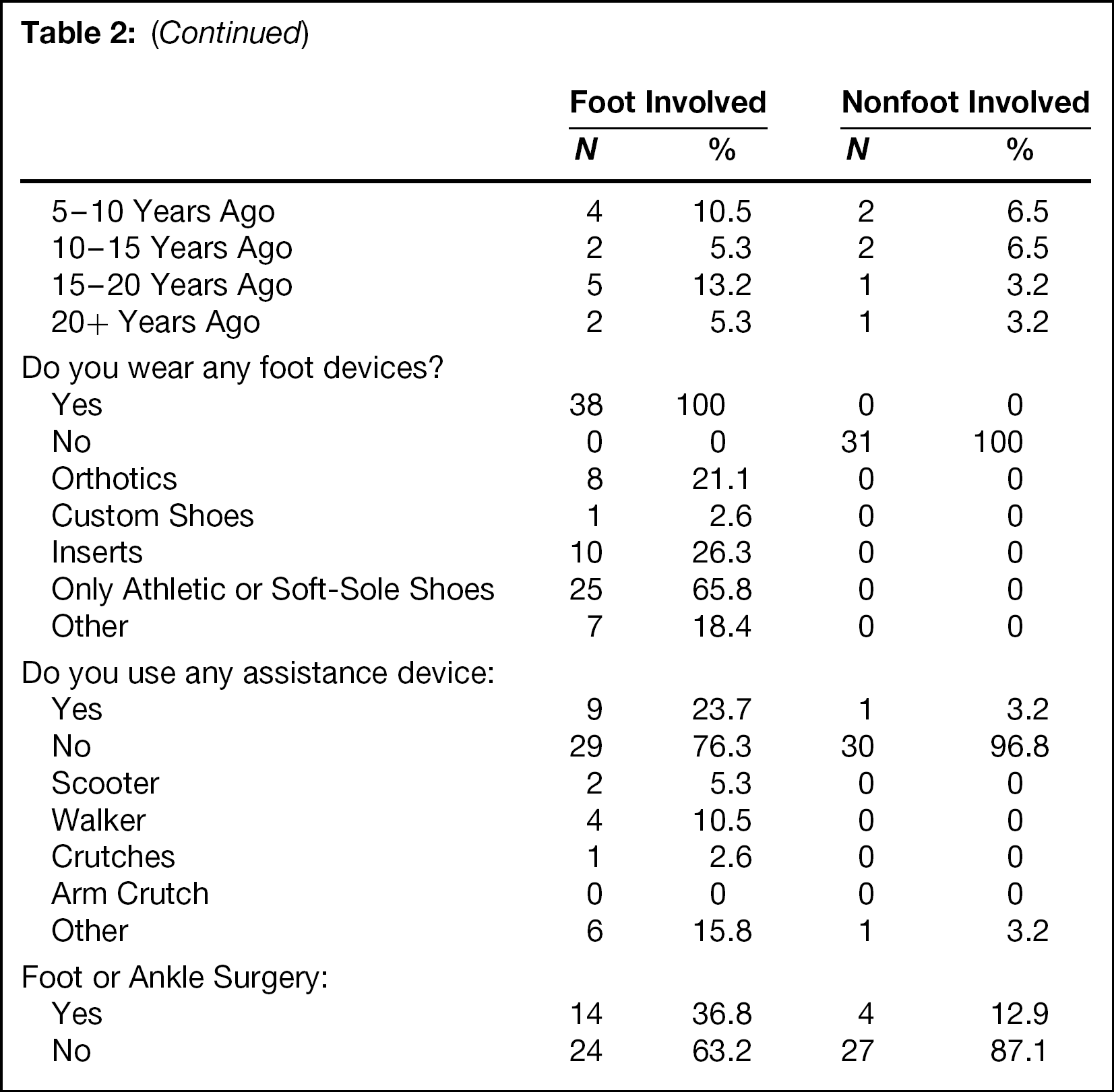
Subjects were divided into control and focus groups based on their response to question 20 from the demographics questionnaire (Tables 1 and 2). A positive response to the use of orthoses, custom shoes, inserts, only athletic or soft-sole shoes allowed them to be included in the focus group (individuals with RA and foot involvement). Of the 69 individuals enrolled, 31 had no foot involvement (control group) and 38 had foot involvement (focus group).
The SMFA was chosen as the measurement tool due to its sensitivity in assessing individuals' health-related quality of life, including physical, physiological, and social well-being. 7 Data derived from the six domains of the SFMA were compared between the control and focus groups. Both the focus and the control group were separately compared to the normative population SMFA data. Collected data were processed using AAOS procedure to obtain SMFA indices on daily activities, emotional status, arm and hand function, mobility, overall function, and bother. Statistical analysis on these indices was performed using Kruskal-Wallis and two-sided Wilcoxon rank-sum tests on SPSS software. Statistical significance was set at p < .05.
Demographics questionnaire
Results
Sixty-nine subjects completed the demographics questionnaire and enrollment SFMA. The average age of the focus group was 59.5 ± 13.8 and the control group was 51.6 ± 18.6. Sixty-one were female (focus group, n = 34; control group, n = 27) and eight were male (focus group, n = 4; control group, n = 4). Responses from the demographics questionnaire are listed in Table 2.
Responses to the SMFA are listed in Table 3. There were significant differences in the Mobility and Functional Indices (p < .044 and .052, respectively). Scores in the Daily Activities, Emotional Status, Arm and Hand Function, and Bother domains were not significantly different.
The normative data, compiled by the AAOS from 1891 subjects, were compared to both the focus group and the control group separately. These results are listed in Table 4. There was a significant difference between the normative population and both the focus and control groups in all six domains of the SMFA: Daily Activities, Emotional Status, Arm and Hand Function, Mobility, Functional Index, and Bother Index.
Responses to demographics questionnaire
Short musculoskeletal functional assessment: domain scoring in RA patients with foot involvement (focus group), as compared to similar patients without foot involvement (control)
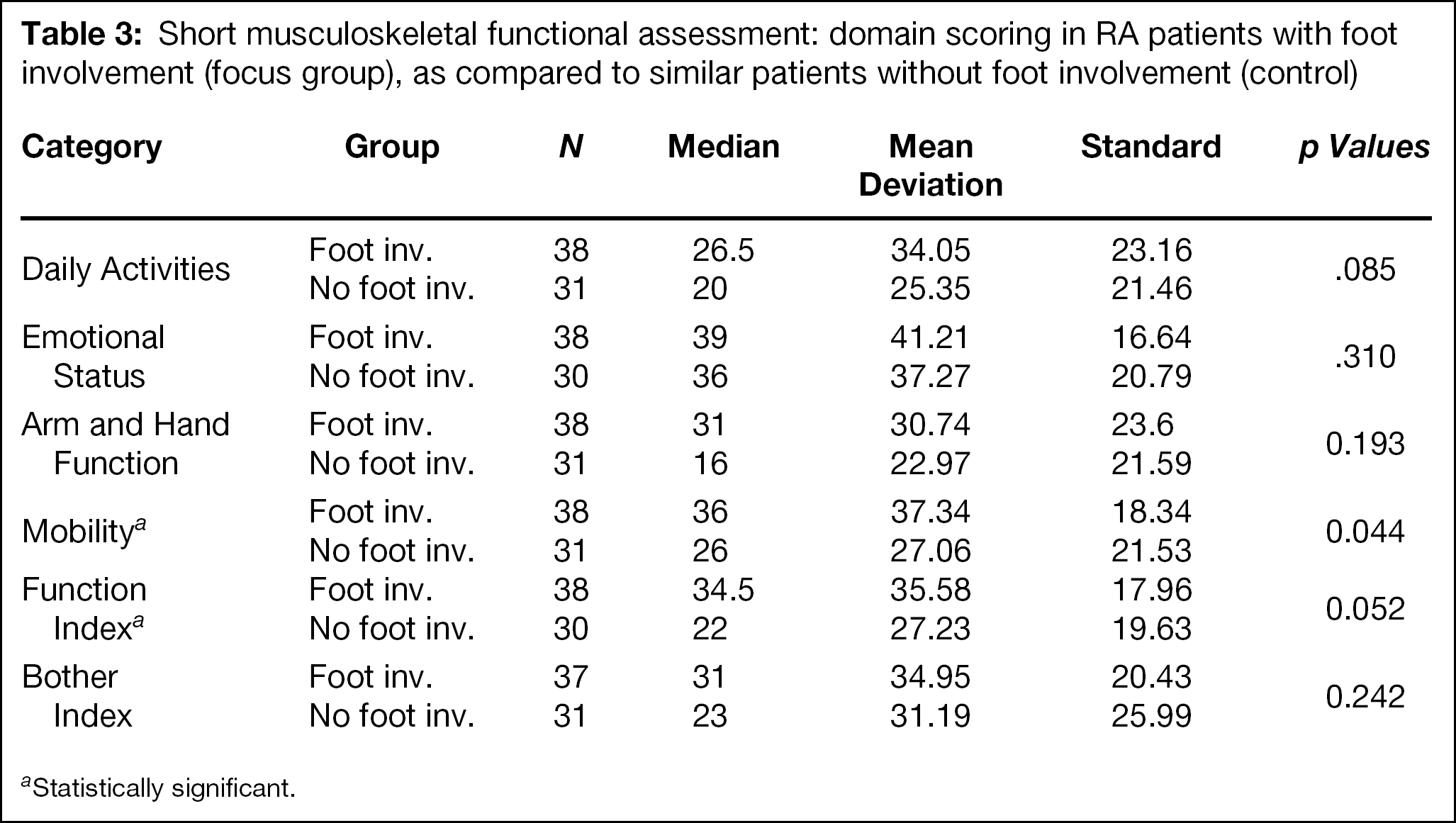
Statistically significant.
Domain scoring in RA patients with foot involvement (focus group), RA patients without foot involvement (control), and population norms for the short musculoskeletal functional assessment
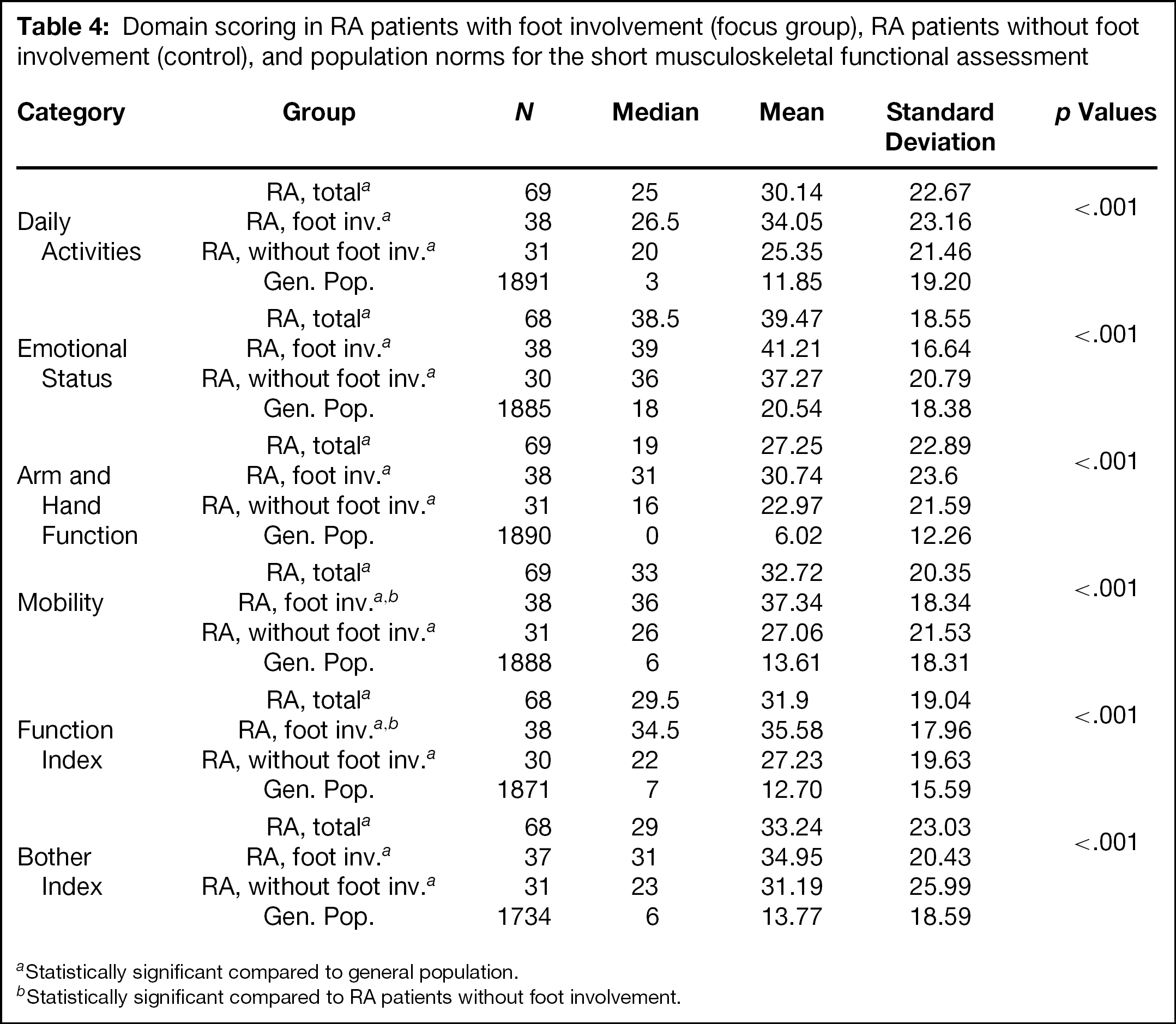
Statistically significant compared to general population.
Statistically significant compared to RA patients without foot involvement.
Conclusions
Individuals with RA have a statistically significant impairment in health-related quality of life. Individuals affected with mild to moderate RA, regardless of foot involvement, demonstrate a severe negative impact in all of the domains of the SFMA. With even mild expression of the disease process in their feet, this negative impact is worsened. We purposely set a very low threshold for foot involvement to determine whether very early/mild disease expression in the foot would be sufficient to affect health-related quality of life. In these benchmark data, these seemingly small changes show a dramatic difference in the individuals' functioning and their quality of life. These individuals demonstrated a severe negative impact on their mobility and functional capacity with even minimal foot involvement.
Very early foot involvement of the rheumatoid process even suggested a trend for less favorable scores in the Arm and Hand Function domain. The presentation of RA in the hands is much more frequent and common than foot involvement, and is, in fact, one of the diagnostic criteria for RA. Therefore, this trend may be a very important, and possibly early indicator of developing disability. We plan to follow this trend longitudinally during the ensuing period of the investigation. Mean scores of the Daily Activity, Emotional Status, and Bother Index domains fared worse than population norms, but there was no statistical difference between subjects using, or not using, adaptive footwear. We purposely excluded individuals with severe disease (stage 4), as it was intuitively obvious that their quality of life was severely affected. The lack of statistical difference between the two groups in the Emotion and Bother domains is not surprising, as their disease expression is reasonably early and similar in both the focus and control groups.
These results reveal that foot involvement, even at a low threshold definition, does suggest greater disease impact for the affected individual. The quality of life for subjects with foot involvement is lower. The individual's functioning is worse simply because he or she cannot wear a variety of shoes. These foot-involved subjects often present to the physician with a seemingly similar level of disease as the nonfoot-involved RA subjects. The results of this investigation suggest that foot involvement in RA portends a more severe expression of the disease process and a greater deleterious impact on the individual's health-related quality of life.