
Abstract
Background:
In the anterior ankle impingement syndrome, recurrent traction to the anterior joint capsule is stated to be the cause of formation of talotibial osteophytes. This hypothesis involves the assumption that the osteophytes originate at the site where a capsular attachment is located. A soft tissue component that can get squeezed between the distal tibia and talus is thought to be responsible for impingement complaints during dorsiflexion movements.
Methods:
In eight ankle specimens, the width of the nonweightbearing tibial cartilage rim and the distance of the tibial and talar cartilage to the capsular attachment were measured. The relationship of the soft tissue components to the anterior joint was studied. The average tibial cartilage rim width was 2.4 mm (1.5–3.0 mm). Tibial and talar cartilage-capsule distances were 4.3 mm (0.5–9.0 mm) and 2.4 mm (1.8–3.3 mm), respectively. In all specimens, the anterior joint space contained a triangular soft tissue component, overlying the joint capsule. The component consisted of a synovial membrane and subsynovial located fat and collagen tissue. It was observed that in 15° dorsiflexion the soft tissue component was squeezed between the tibia and talus.
Conclusions:
The anterior ankle joint capsule attaches proximal to the site where the anterior talotibial spurs originate. The hypothesis of formation of talotibial spurs due to repetitive capsule traction therefore does not seem plausible. The anatomic findings do support the hypothesis that an anteriorly located soft tissue component is present that can give impingement symptoms.
INTRODUCTION
Osteophytosis is the process of formation of new bony spurs at the joint margin and is associated with osteoarthritis. These osteophytes are neoplastic, cartilaginous, and osseous protrusions around the joint space. They consist of typically five types of tissues: 1) superficial layer mesenchymal fibrous connective tissue, 2) fibrocartilage, 3) hyaline cartilage, 4) deeper layers of hypertrophic cartilage and 5) deeper layers of bone. The deeper layers become hypertrophic, vascularize, and undergo endochondral ossification. 1 In osteoarthritis this process is thought to stimulate cells at the chondrosynovial junction by polysaccharides derived from degradation of articular cartilage. 22
Bony spurs can also develop due to repetitive (micro) trauma. 3,6 When a bony spur forms at a ligament, tendon, or capsule insertion, it grows in the direction of the natural traction pull of these soft tissue structures. The spurs form at the site where the stiff collagen tissue attaches to the bone. Recurrent microtrauma due to traction will lead to tendoperiostosis and subsequently enchondral calcification. This process is defined as enthesophytosis. 13 The enthesophytes are seen at several sites, especially at the calcaneum, patella, radius, and lesser and greater trochanter. 13
In the ankle, the presence of anteriorly located tibial and talar ankle spurs has been reported in up to 60% of professional soccer players. 10 The etiology of the formation of these impinging talotibial spurs is not fully understood. McMurray 11 thought that the development of the talotibial osteophytes was caused by repeated capsule traction of the anterior ankle joint from repetitive kicking with the foot in full equinus (i.e., traction spurs). Since then, the “traction spurs” theory has been cited widely. 3,4,7,12
Since bony spurs originate from anterior surfaces of the ankle joint at the level of the joint space, the traction spurs hypothesis involves the assumption that the capsular attachment is located at the level of cartilage rim near the joint space. The literature fails to provide descriptions of the exact capsular attachment and its topographical relation to the cartilage rim. From arthroscopic studies, it is known that anterior osteophytes are found to be situated well within the capsular attachment at the joint margin, and not at the capsular origin. 7 The traction spurs theory is therefore not supported by anatomic, morphologic, and clinical data.
Talotibial spurs can result in the anterior bony ankle impingement syndrome. 3,14,20,21 Bony spurs are, however, not automatically associated with impingement complaints. Asymptomatic ankle osteophytes are reported in 45% of soccer players and 59% of dancers. 10,15 The pain is probably caused by impingement of synovial or posttraumatic scar tissue between the bony surface of the distal tibia and/or malleoli and the bony contours of the talus. 20
The aim of the present study was to investigate whether the capsular attachment was located on the anterior cartilage rim at the joint. This could support the traction spurs theory. We also wanted to study whether an anteriorly located soft tissue component was present that could induce impingement. An anatomic study was performed to describe the exact anatomic anterior cartilage rim, capsular attachment, anteriorly located soft tissue component, and their relations to the anterior ankle joint.
MATERIALS AND METHODS
A total of nine cadaver lower limb specimens were obtained. They were sealed in plastic bags and deep-frozen to −30°C. The average age of the specimens was 69 years (range, 58–77); five were males and four were females. No information was available about individual case histories.
The frozen specimens were sawed in sagittal sections of 4 mm in diameter. The sections were thawed at room temperature. During direct observation, specimens with signs of severe ankle osteoarthritis were eliminated from the study. In the sagittal sections, special attention was given to the details of the anterior joint space, soft tissue components, and capsular attachment.
The width of the nonweightbearing distal tibial cartilage rim was measured. The dimensions of the proximal tibial cartilage rim projecting in the frontal plane to the joint line were measured at the medial and lateral capsular attachment. The measurements were performed at a point one-fourth, one-half, and three-fourths between these two medial and lateral landmarks. (Fig. 1) The cartilage-capsule distance, distance of the tibial and talar cartilage border to the capsular attachment, was measured at the same five landmarks (Fig. 1).
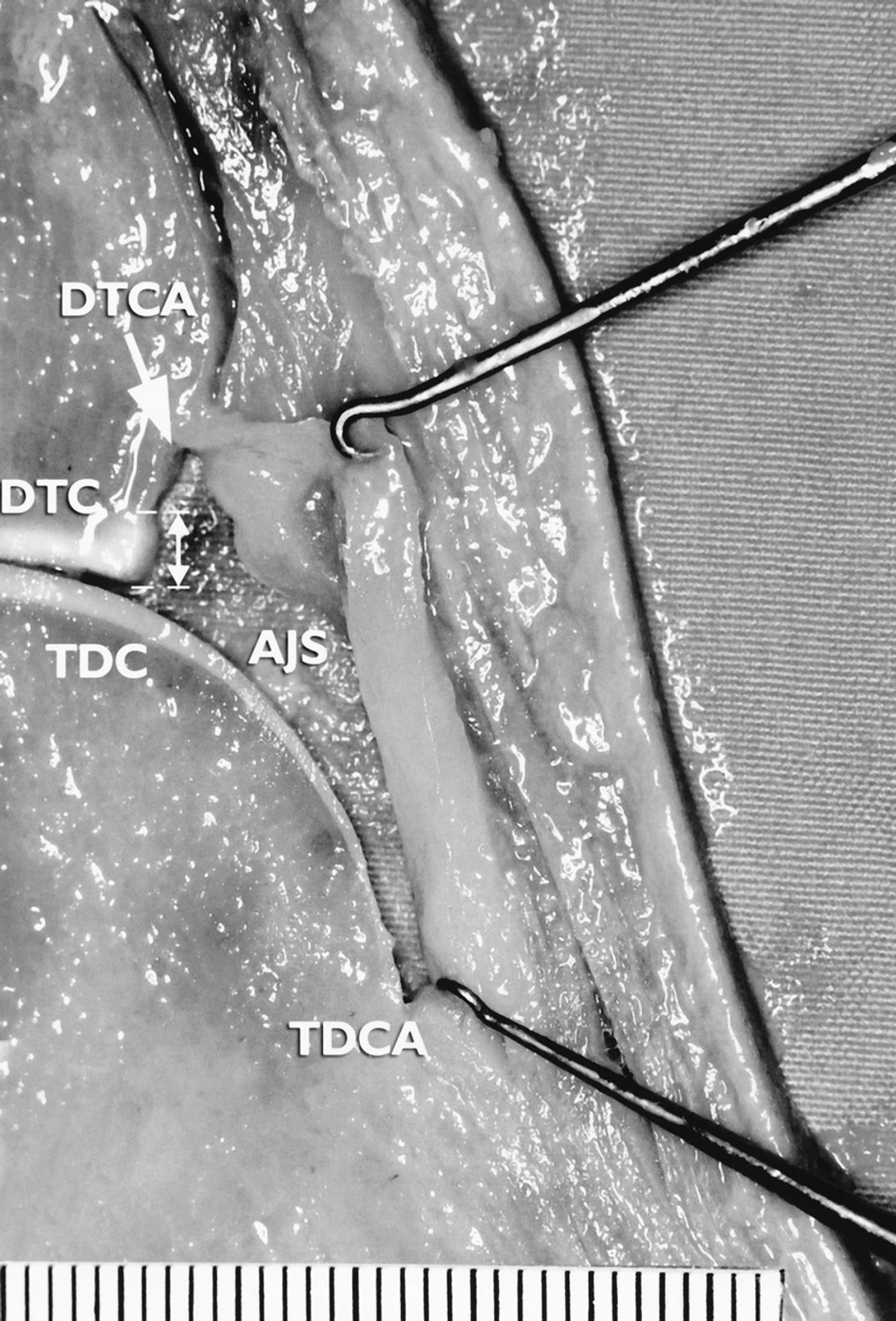
Sagittal section of an ankle specimen showing the width of the nonweightbearing distal tibial cartilage rim (double arrow) and distance of the distal tibial and talar dome cartilage to the capsule attachment. The triangular soft tissue component of the anterior joint space is smoothly pulled with two hooks to show the tibial (arrow) and talar capsule attachments. Note that the capsular attachment is situated proximal to the joint line and cartilage rim. The measuring rod is in millimeters. DTCA, distal tibia capsule attachment; DTC, distal tibia cartilage; AJS, anterior joint space; TDC, talar dome cartilage; TDCA, talar dome capsule attachment.
The sections were manually manipulated in 15° dorsiflexion position to study the relation of the soft tissue components and the anterior joint space. A histopathologic analysis was performed of the soft tissue component, bone and cartilage. The slides were hematoxylin-eosin stained.
RESULTS
One specimen showed severe signs of osteoarthritis and was excluded from the study. Eight ankle specimens were studied.
Anterior Cartilage Rim and Capsule Attachment
The average nonweightbearing tibial cartilage rim width and cartilage-capsule distance at five anatomical landmarks are given in Table 1. The overall average tibial cartilage rim width and tibial cartilage-capsule distance were 2.4 mm (1.5–3.0 mm) and 4.3 mm (0.5–9.0 mm), respectively.
Average nonweightbearing cartilage width (mm) of the distal tibia, and tibial and talar cartilage-capsule (mm) distance in eight sagittal sawed ankle specimens
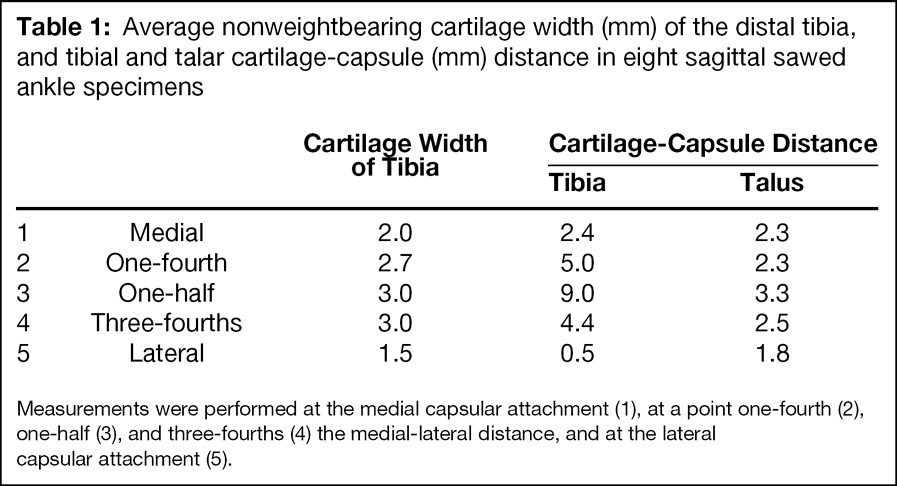
Measurements were performed at the medial capsular attachment (1), at a point one-fourth (2), one-half (3), and three-fourths (4) the medial-lateral distance, and at the lateral capsular attachment (5).
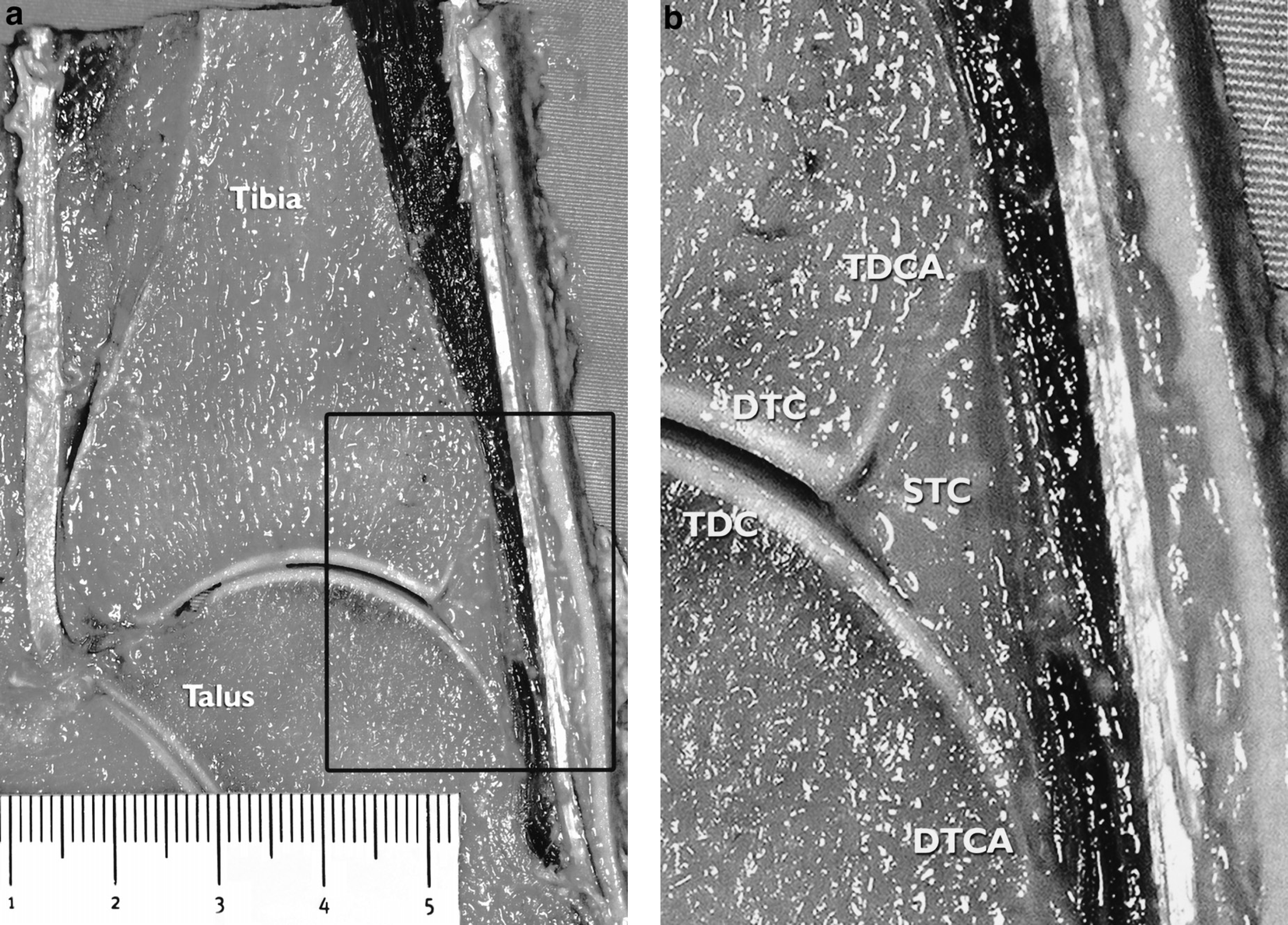
On the talar site there was a gradual decrease of cartilage thickness in distal direction (Fig. 2). The overall average cartilage-capsular distance was 2.4 mm (1.8–3.3 mm).
Anterior Joint Space and Soft Tissue Components
In the sagittal sections, the anterior joint space was found to be bordered by the distal tibia, talar dome, and anterior joint capsule (Fig. 2). In all specimens, the anterior joint space contained a triangular shaped soft tissue component that extended into the tibiotalar joint. When the joint was forced into a 15° dorsiflexed position, the anterior joint capsule moved into an anterior direction. In this position, there was a diminished anterior joint space, while the triangular soft tissue component was squeezed between the anterior distal tibial rim and talus in all specimens.
Histopathologic Analysis
Histopathologic analysis revealed that at the site of the joint space the soft tissue component was bordered by a layer of synovial cells, which forms the synovial membrane. The triangular subsynovial soft tissue component consisted of fat tissue and small parts of collagen tissue and blood vessels (Fig. 3).
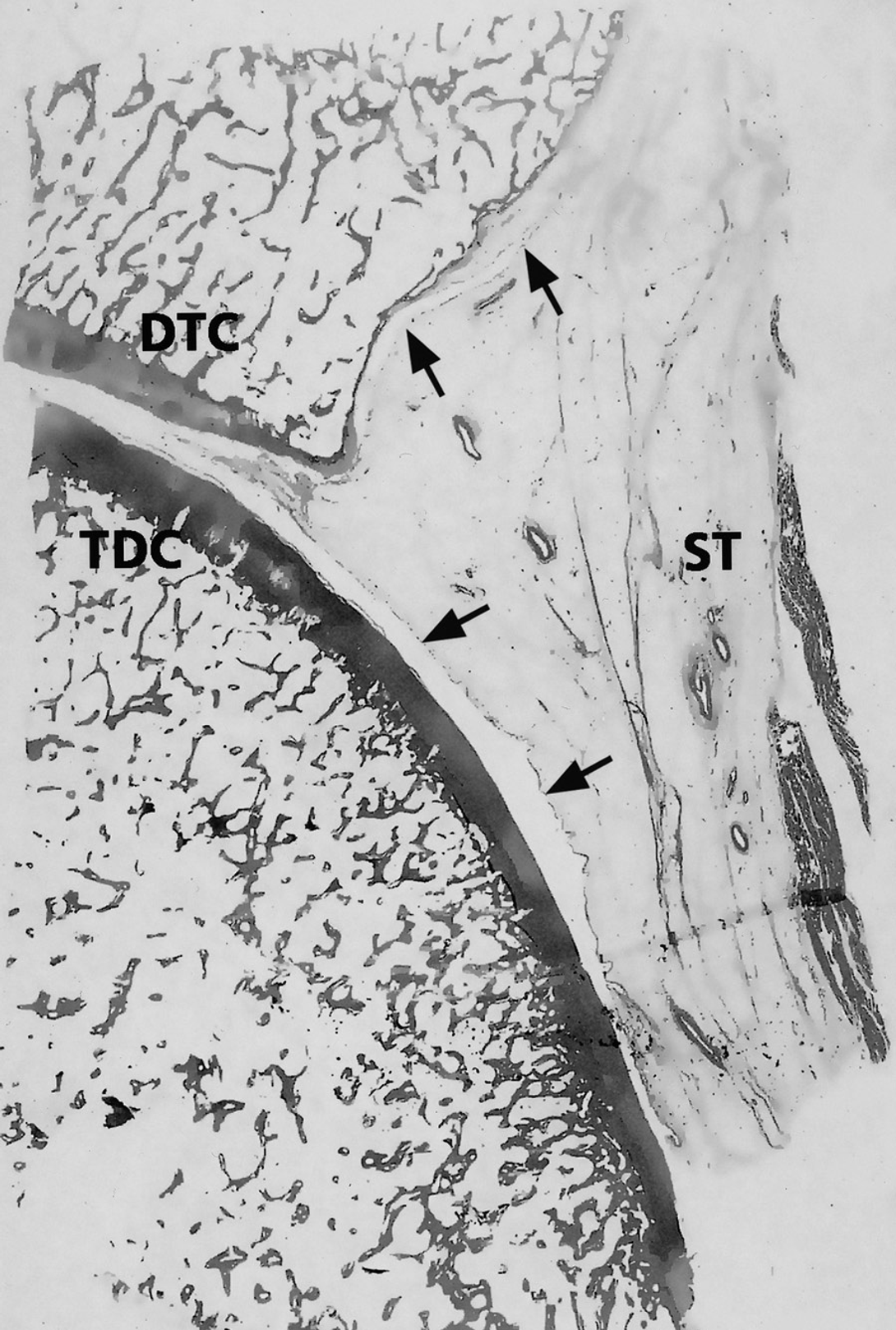
Histopathologic analysis (hematoxylin-eosin stained). It shows that at the site of the joint space the triangular soft tissue component is bordered by the synovial membrane (arrows) and subsynovial located collagen, blood vessels, and fat tissue. Note that a small part of the soft tissue component is projecting into the joint space. DTC, distal tibia cartilage; TDC, talar dome cartilage; ST, subsynovial tissue.
DISCUSSION
Traction to the anterior ankle capsule during plantarflexion movements is stated to be an etiologic factor of the formation of anterior tibiotalar osteophytes in the anterior ankle impingement syndrome (i.e., traction spurs). 3,4,7,11,12 This hypothesis is supported by the fact that these spurs are frequently found in athletes, who repetitively force their ankle in hyperplantarflexion actions, resulting in repetitive traction to the anterior joint capsule. 8 It assumes that the capsular attachment is located at the anterior cartilage rim, where the spurs originate.
This study, however, shows that in cadaver specimens the anterior joint capsule attaches onto the tibia on average 6 mm proximal to the anterior cartilage rim. On the talar site, the capsule attaches approximately 3 mm from the distal cartilage border. The distance of capsule attachment to the site where bony spurs originate is thus relatively large. Based on these anatomic observations, the hypothesis of formation of talotibial spurs due to recurrent traction to the joint capsule (traction spurs) does not seem plausible. This is supported by observations during arthroscopic surgery. 20 In patients with bony impingement, the location of tibial spurs is reported to be at the joint level and within the confines of the joint capsule. 17,20 On the talar side, the typical osteophytes are found proximal to the talar neck notch. Both tibial and talar osteophytes can easily be detected during an arthroscopic procedure with the ankle in forced dorsiflexion. The capsule does not have to be detached to locate these osteophytes. By arthroscopically shaving away the osteophyte at the joint level, a bare area is created within the confines of the joint capsule. Long-term results of arthroscopic resection of these spurs have shown that recurrence of these osteophytes located at the joint level occurs in 67% of the patients. 20 It is very unlikely that this recurrence is caused by traction to the joint capsule. The spurs, therefore, must be considered as osteophytes, and not enthesophytes.
It was shown that along the distal tibia, the width of the nonweightbearing cartilage rim extends up to 3 mm proximal to the joint line. It is this nonweightbearing anterior cartilage rim that undergoes the osteophytic transformation. 5 Damage to this anterior cartilage rim is known to occur in the majority of supination traumas. 18,19 It has been postulated that depending on the degree of damage, chondral and bone cell stimuli will initiate a repair reaction with cartilage proliferation, scar tissue formation, and calcification. Additional damage by ankle sprains due to recurrent instability or forced dorsiflexion movements will further enhance this process. 3 Recent studies showed that ankle instability is significantly correlated with osteophytic formation, especially in the medial ankle compartment. 9,19 Repetitive direct (micro) trauma to this anteriorly located cartilage rim, as seen in the kicking action in soccer, is another important factor. 16
In the anterior ankle impingement syndrome, the cause of pain is thought to be not the osteophyte itself, but the inflamed soft tissue impingement that occurs between the osteophytes. 17 Tibial and talar spurs typically do not overlap each other. 2 Histopathologic analysis of arthroscopic resected soft tissue reveals synovial changes with evidence of chronic inflammation. 6 In all our specimens, a triangular soft tissue synovial fold, subsynovial fat, and collagen tissue were found along the entire anterior tibiotalar joint line. During forced dorsiflexion movements, this soft tissue component is squeezed between the anterior distal tibia and the opposite talus. Recurrent trauma to this soft tissue component may lead to hypertrophy of the synovial layer, subsynovial fibrotic tissue formation, and infiltration of inflammatory cells. In theory, arthroscopic excision of the soft tissue could relieve pain. Talar and tibial osteophytes, however, decrease the anterior space, and compression of this soft tissue component is more likely to occur. In a bony anterior impingement lesion, we believe that it is important to remove these osteophytes in order, to restore the anterior space and reduce the chance of symptoms recurring.
In conclusion, it was shown that the anterior capsule does not attach at the site where the anterior talotibial spurs originate. The anatomic findings support the hypothesis that an anteriorly located soft tissue component is present that causes pain from impingement during dorsiflexion.