
Abstract

INTRODUCTION
Brachydactyly is an acromelic osteochondrodys-plasia due to either abnormal positional information or disturbed function of certain growth factors responsible for the expression of inborn growth potential. During growth, the hallmark is a “cone epiphysis,” the apex of which protrudes into the adjacent metaphysis. Epiphyses close prematurely leading to short, broad tubular bones. The single most commonly hypoplastic bony segment is the middle phalanx (brachyphalangia or brachymesophalangia).
Brachymetacarpia and brachymetapody (short metacarpal /metatarsal) are also included with the hypoplastic deformities, but this is extremely rare and is not usually noted until after the adolescent growth spurt, and is often included under the broad definition of brachydactyly (small digits). Simultaneous hand and feet hypoplastic anomalies are rare. 5 We describe a case of a new genetic mutation of simultaneous hand and feet brachydactyly, not previously described, with two treatment options. Finally, we provide a short clinical review of the types of brachydactyly.
CASE HISTORY
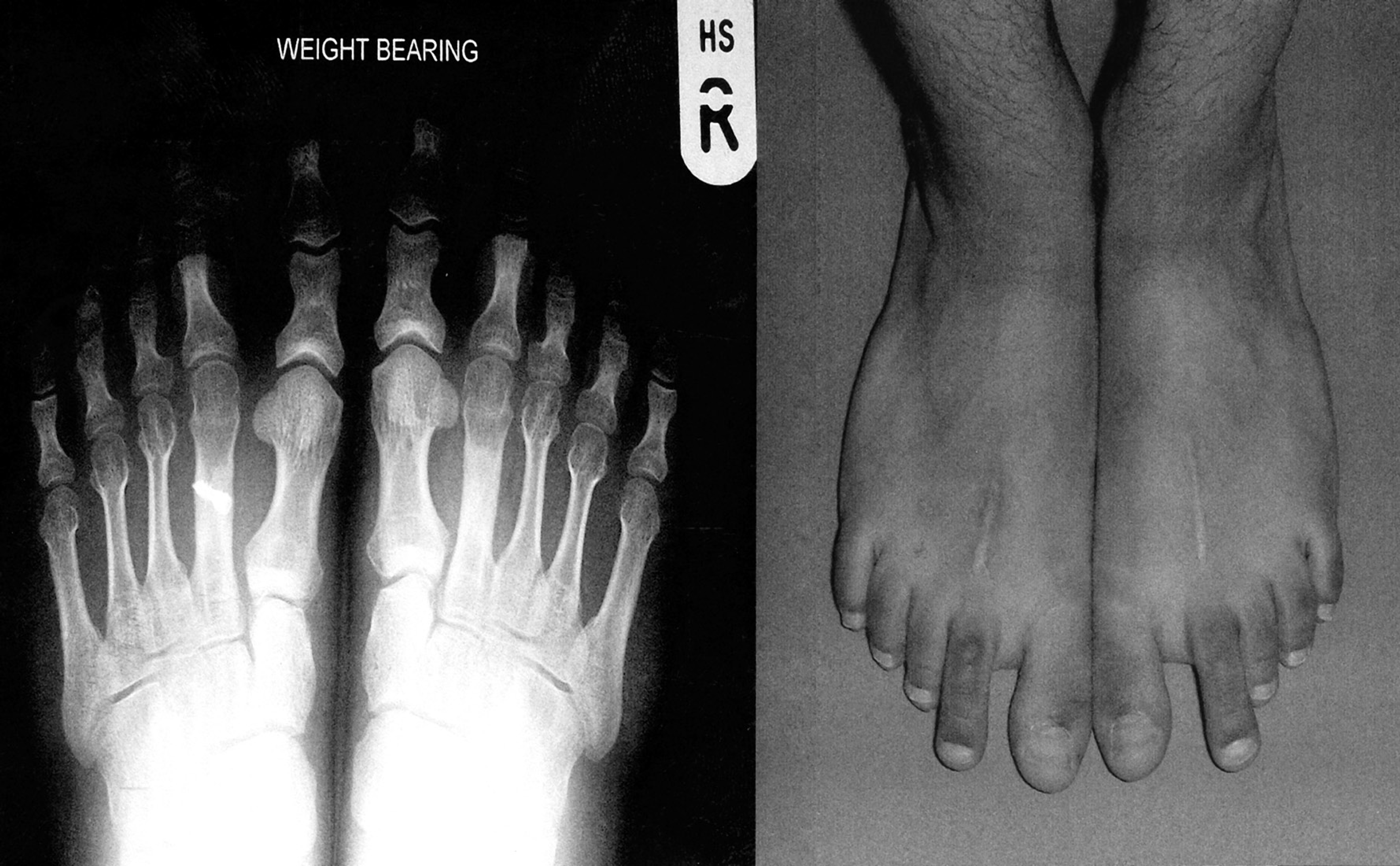
A 12-year-old girl of Indian ancestry presented with increasing pain in the soles of both feet and difficulty wearing shoes for 1 year. Examination revealed normal growth and development with bilateral asymptomatic symmetrical brachydactyly of her hands (Fig. 1) with normal length index fingers bilaterally. She walked with an antalgic gait. She had bilateral symmetrical brachydactyly affecting the first, third, fourth, and fifth digits of both feet (Fig. 2). The second digits appeared normal; however, they were protruding almost half the length of the second digit past the big toes bilaterally. The bases of the second toes were swollen and tender. Pedobarograph studies revealed this area to be the pressure points when weightbearing. Radiographic studies identified normal second digits; fusion of the epiphyses with coning and metatarsophalangeal hypoplasia of the first, third, fourth, and fifth digits; and broad proximal phalanges of the first digits and normal tarsal bones (Fig. 3). Radiographs of the hands showed the same pattern of abnormality.
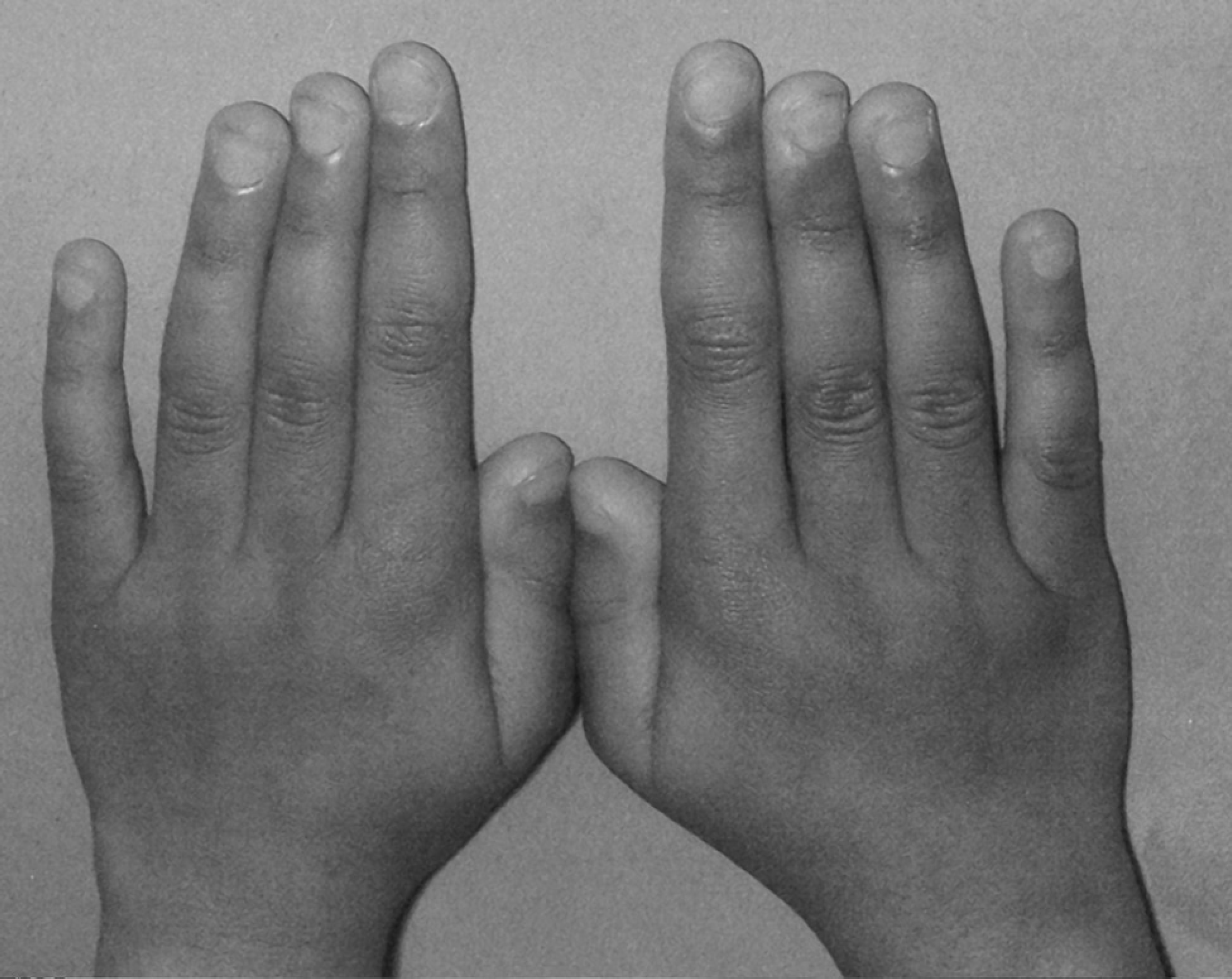
Photograph of both hands with normal index fingers and brachydactyly of the remaining fingers.
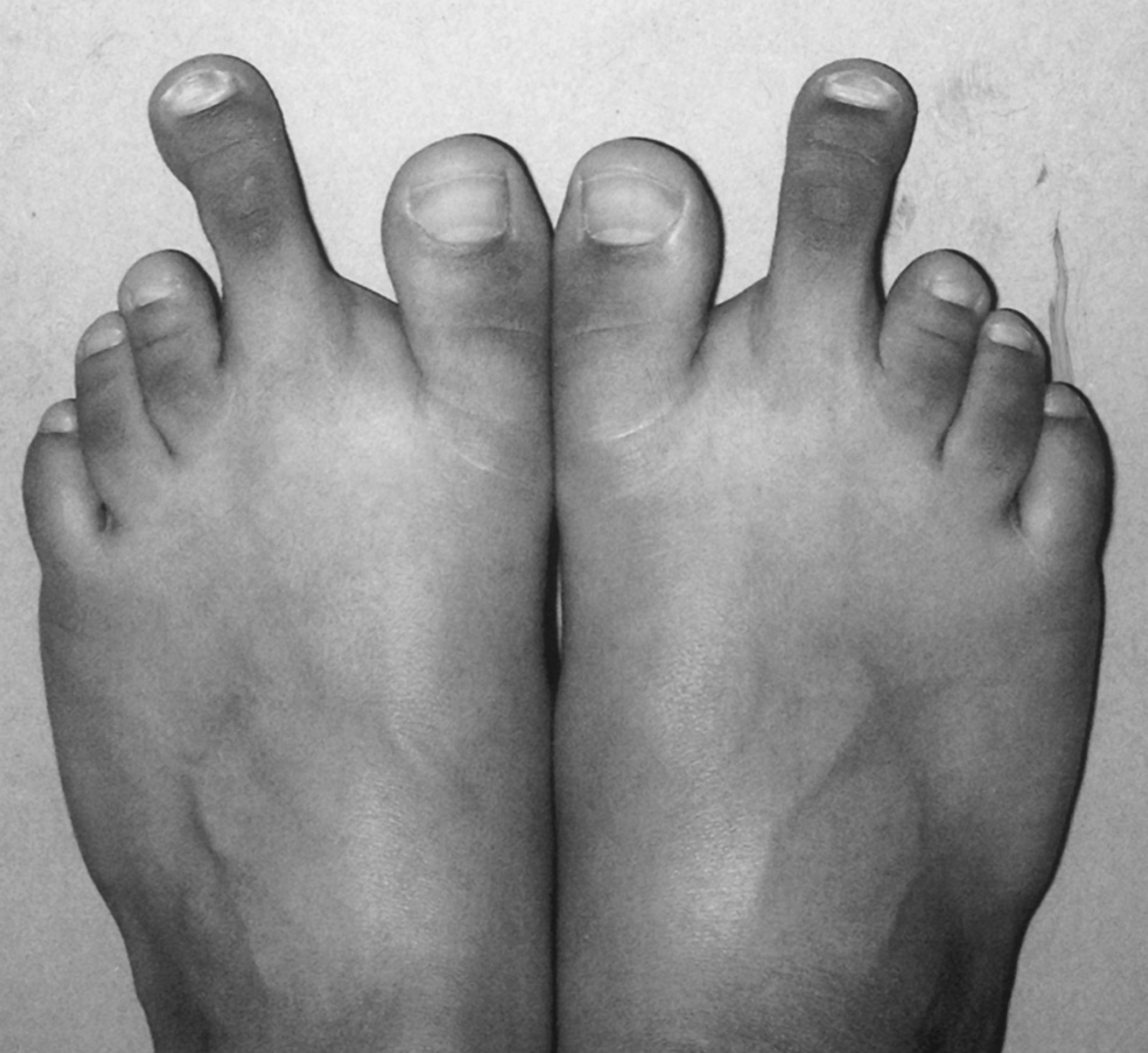
Photograph of both feet showing the protruding normal second toes with brachydactyly of the remaining toes.

AP radiographs of both feet showing elements of both brachydactyly type D (bilateral short and broad hallux terminal phalanges) and type E (short bilateral first metatarsals with short second to fifth phalanges).
She was diagnosed by genetic, radiological, and pediatric consultants as having an isolated symmetrical brachydactyly disorder of her hands and feet (all syndromic systemic associated disorders were excluded). Both parents were free of the condition and the geneticists diagnosed a new mutation of brachydactyly D/E. She had failed conservative management and was in constant pain, and her lifestyle was dramatically affected. Bilateral shortening metatarsal osteotomies with a soft tissue release of the second digits were performed. The osteotomy was internally fixed with a single cannulated screw. A check radiograph revealed the right second metatarsal had fractured at the site of the internal fixation. The patient was taken back to surgery where the screw was removed and two Kirschner wires were inserted to maintain the reduction (Fig. 4). Plaster cast boots were used postoperatively.

Postoperative radiographs showing the shortening osteotomies with New Deal screw fixation of the left second metatarsal and the revised Kirschner wires of the right second metatarsal.
The patient walked with full weightbearing as pain permitted. The plaster boots and Kirschner wires were removed 6 weeks after the procedure. Three months after the procedure, the wounds had healed. At 6 months, the patient walked normally, pain free, wearing normal shoes, and the swelling and capsulitis had settled completely. The cosmetic deformity and slightly longer second toe did not concern the patient or her parents and patient satisfaction was extremely high (Fig. 5). At the final 2-year follow-up, the scars and toe length had improved; the patient remained asymptomatic and radiographs revealed union at the osteotomy sites (Fig. 6).

Photographs of both feet showing the reduction of size of the second metatarsals and the healed wounds (6-month follow-up).
Radiograph on the left and photograph on the right of the same patient at the 2-year follow-up showing satisfactory clinical outcome and union at the osteotomy sites.
DISCUSSION
Brachydactyly is a group of rare conditions in which various subtypes have been defined based on the specific characteristic pattern of digital bones involved and the frequent association of various systemic disorders. All display an autosomal dominant pattern of inheretance of genes acting with variable expressivities and penetrance, and occasional new mutations (sporadic cases) do occur, but no specific etiological factor has been identified. Presentation is type specific, with associated syndromic clinical features usually present from birth. Hypoplasia of the digits may range from simple shortening (most common) to a small hand or foot with nothing more than nubbins for digits. There usually is some degree of hypoplasia of all tissues, not just the bones. Except for the nubbin-like digits, function usually is near normal. Brachymetacarpia alone usually presents during the teenage growth spurt as a depression of one or more metacarpal heads with the fist clenched. The ulnar two fingers are most commonly affected.
Brachydactyly type A has six different subtypes as described by Bell (1951) 2 :
Type A1 is associated with short stature, hypoplastic middle phalanges of the fingers and toes and proximal phalanges of the thumbs and big toes, with occasional terminal symphalangism.
Type A2 is characterized by hypoplastic, rhomboid, or triangular shaped middle phalanges of the index finger and second toe, leading to radial or hallux deviation.
Type A3 is similar to type A2, with fifth digit involvement.
Type A4 results in brachymesophalangy affecting mainly the second and fifth digits with absent middle phalanges of the lateral four toes. There is often associated congenital talipes calcaneovalgus.
Type A5 is associated with absence of the middle phalanges, nail dysplasia, and duplication of the terminal phalanx of the thumb.
Type A6 may display hypoplastic or absent middle phalanges of the hands and feet, mesomelic shortening of the limbs, and a short stature. The terminal phalanges of the index fingers deviated radially. In the wrist, the hamate and capitate bones are joined and there may be an associated delayed coalescence of bipartite calcanei.
Brachydactyly type B is characterized by hypoplasia of the middle phalanges or absence of the terminal phalanges of the index to little fingers, usually with absence of the nails. The thumbs may be of normal length, are often flattened and broad, and occasionally bifid. There is also mild syndactyly between the digits. This type of hand malformation presents the severest deformity in the brachydactyly group. Syndactyly in the feet usually involves the second and third toes. The feet are similarly but less severely affected.
Brachydactyly type C ranges from shortening of the middle phalanges and first metacarpal to shortening of all the metacarpals; brachymesophalangy; shortening of the proximal phalanges of the index and middle fingers and hypersegmentation (extra phalanx) of the index and middle fingers. Elongation of the radial side of the base of the second proximal phalanx results in ulnar deviation at the second and third metacarpophalangeal joints.
Brachydactyly type D is characterized by short and broad terminal phalanges of the thumbs and big toes. Three-quarters of individuals will have bilateral first distal phalangeal hypoplasia. There may be generalized involvement of the apical skeleton.
Brachydactyly type E characteristically causes an asymmetrical shortening of one or more metacarpals or metatarsals or both, with or without variable involvement of the phalanges. Hertzog suggested that there are at least three subtypes: E1, in which shortening is limited to fourth metacarpals and/or metatarsals; E2, in which variable combinations of metacarpals and metatarsals are involved, with shortening also of the first and third distal and the second and fifth middle phalanges; and E3, a category which may have a variable combination of short metacarpals without phalangeal involvement. 8 Previous reports of orthopaedic management are rare and the majority involve digit-lengthening procedures mainly of the hands. 1,3,4,9
We found clinical and radiological features of type D and type E brachydactyly as described above. Operative procedures were aimed at a reduction in length of the protruding toe to a functional size while maintaining an acceptable cosmetic appearance. Possibilities included soft tissue debulking combined with an osteotomy or epiphysiodesis, reduction syndactyly, and toe amputation of the protruding normal digit. Grogan et al. have reported the success of ray amputation; however, we use this method as a last resort or salvage procedure in pediatric patients. 7 Epiphysiodesis would not have provided any meaningful shortening due to late age of presentation. Bilateral shortening osteotomies of the second metatarsals were performed as described by Fournet-Fayard et al. 6 The cannulated screw and Kirschner wires proved to be alternative forms of successful fixation. Shortening of the toe to lengths the same as, or less than, the other toes may not be possible, nor is it necessary for a satisfactory outcome.
Our patient and her family were fully investigated by the pediatricians, geneticists, radiologists, and the orthopaedic team, and as her parents were found be normal clinically and radiographically, a diagnosis of a new mutation (sporadic case) of an isolated combined type D and E brachydactyly was made. The parents were counseled and advised that there was a one in two chance of passing on the brachydactyly to future generations (autosomal dominant). There have been documented cases of a combination of types of brachydactyly but this particular pattern of involvement of the hands and feet as we have described has not been previously reported.