
Abstract
Background:
Pigmented villonodular synovitis (PVNS) is relatively uncommon. The disorder results in increased proliferation of synovium causing villous or nodular changes of synovial-lined joints, bursae and tendon sheaths. This study examines the occurrence of PVNS about the ankle and its association with trauma.
Methods:
Ten patients over a 10-year period were identified as having PVNS of the ankle. The average age was 40.2 (range 27 to 62) years. There were four women and six men. Average followup was 4.5 (range 1 to 11) years from the initial surgery. Four patients had bone involvement. All patients who were athletically active before symptoms arose complained of persistent pain and swelling in the lateral ankle. Their initial clinical symptoms were indistinguishable from commonly associated pathologies with persistent lateral ankle pain (i.e. tenosynovitis, osteochondral defects, os trigonum injury, and tendon tears). All patients had magnetic resonance imaging (MRI) revealing PVNS, which is represented by low-signal appearing masses on T1-and T2-weighted images. All patients' histopathology results revealed multinucleated giant cells and foam cells laden with hemosiderin deposits. All patients had synovectomy and tenosynovectomy.
Results:
Eight patients were able to return to some sports (range 4 to 12 months); two had continued pain, disability, and inability to return to sports because of recurrence.
Conclusions:
PVNS should be considered in athletically active patients with persistent lateral ankle pain and swelling, particularly if bone erosions are visible on plain radiographs.
INTRODUCTION
Pigmented villonodular synovitis (PVNS) is a relatively uncommon disorder that results in an increased proliferation of synovium, causing villous or nodular changes of synovial-lined joints, bursae, and tendon sheaths. 7 Aggressive bone and cartilage absorption, although not always found, are characteristics that distinguish PVNS from other inflammatory arthropathies. 13 The etiology of PVNS is controversial. Various mechanisms have been proposed, such as disturbances in fat metabolism, bleeding into the joint, and vascular neoplasm, but the two leading theories are an inflammatory response or neoplastic formation. 5,7,8,10,20
There are two forms of PVNS: diffuse and localized. 7 The diffuse form refers to involvement of the entire synovial membrane of a joint or bursa. The localized form refers to involvement of the tendon sheath or a portion of the joint lining. It was previously believed that the diffuse and localized types were two different pathologies. In 1941, Jaffe et al. recognized that they were merely two presentations of the same entity. 10 In both diffuse and localized forms, the synovium is highly proliferative and appears either nodular (localized) or villous (diffuse). The extraarticular form also may be referred to as a giant cell tumor of the tendon sheath (GCTTS). 2,7,15 The most common location of GCTTS is the sheaths of the fingers. 4 Tendon sheath PVNS and GCTTS, when found in the foot and ankle, are most often seen in the extensors and flexors of the digits and rarely along the tendons of the ankle. 4,24
The etiology of PVNS is not known but several theories have been proposed. The presence of lipidladen foam cells has led to the conclusion that PVNS is related to problems with fat metabolism. This theory is undermined by the findings that there are no consistent disturbances of serum triglycerides or cholesterol changes in patients with PVNS. 20 Hemosiderin deposits found in PVNS lesions have lead to the conclusion that bleeding into a joint or tendon sheath may cause PVNS. The perpetual bleeding into joints found in patients with hemophilia has demonstrated a tendency towards fibrosis similar to PVNS. 8 Further evidence was seen in animal studies. When blood was injected into joints changes similar to those in PVNS were found. 7,14 The fibrosis in the animal studies and in hemophiliac patients is not identical to that found in PVNS, missing the characteristic giant and foam cells. 7,14 To further dispute blood as the specific causative factor of PVNS, the animal studies found similar fibrosis whether it was blood or saline injected into the joint, indicating a more general reaction of synovium to a foreign body. 20 A neoplastic etiology has been proposed because of the proliferative nature of PVNS and its tendency to invade bone. 8
The purpose of this paper was to study the occurrence of PVNS about the ankle, assess the activity level of athletic patients undergoing treatment for PVNS, and to show that there may be an association with ankle trauma. We also wanted to discuss the diagnostic and therapeutic aids available.
MATERIALS AND METHODS
Ten patients with histologically verified PVNS about the ankle between 1993–2002 in a sports medicine clinic, were reviewed. PVNS was documented in six men and four women with an average age of 40.2 (range 27 to 62) years. The presenting symptoms and histories of previous injuries were obtained from patients' medical records. All but one patient (who had moved out of the area) could be evaluated at the time of this study.
Most of the patients were previously involved in lateral motion sports such as basketball, tennis, soccer, or aerobics. Two patients ran for exercise. The average followup from the index surgery was 4.5 years, with two patients having had surgery one year prior to the study. The longest followup in one patient was 11 years.
Eight patients previously had not been diagnosed with PVNS before presenting to the clinic. One patient was referred for a second opinion on management of recurrent PVNS. Nine patients underwent surgical intervention by the senior author (AS). Surgery involved synovectomy and tenosynovectomy, along with bone grafting of any bony defects. Hydrogen peroxide was used for irrigation to provide further destruction of abnormal synovial cells. Plain radiographic and magnetic resonance imaging (MRI) evaluations were obtained on all patients preoperatively, which were useful for incisional placement and surgical approach. Informed consent was obtained for all patients.
RESULTS
PVNS was found in multiple sites about the ankle including three ankle joints, three peroneal tendon sheaths, two subtalar joints, two flexor hallucis longus tendon sheaths, and one posterior tibial tendon sheath. Four patients had bony erosions, two with PVNS within the ankle and two within the subtalar joint. One patient had erosions of the tibial plafond, fibula, and talus. In this case, the PVNS also invaded the flexor tendons. Another patient with an ankle lesion had bony erosions on the lateral aspect of the talar neck. An additional patient had degenerative changes of the subtalar joint and bony involvement of the calcaneus. A summary of these findings is presented in Table 1.
Nine out of ten patients had a history of ankle sprains, with pain laterally. These patients presented with symptoms that were similar to more common pathologies such as peroneal tendon tears, os trigonum, flexor hallucis longus tenosynovitis, or osteochondral lesions of the talus. Patients consistently noted pain and swelling at the site of involvement. Plain radiographs showed bony changes about the talus and adjacent bones in four out of ten patients; MRI showed PVNS findings in all ten.
Three patients had recurrent PVNS. Two patients were unable to return to their desired activities including sports. Another patient (who was able to return to sports) was previously operated elsewhere and had recurrence in the posterior tibial tendon sheath. In this patient the initial mass histopathologically was diagnosed as a rheumatoid nodule, not PVNS. Recurrences in both of these patients were found at 1.5 years after the initial surgery. Another patient who had diffuse involvement of the ankle has had additional recurrences despite several treatments with radiation. This was the second patient in the series who was unable to return to sports. The eight remaining patients were able to return to some degree of athletic activity between 4 to 12 months postoperatively. Most of the patients wore a lace-up ankle brace during sports but not for daily activities. Table 1 includes a summary of the patients' history, limitations, and return to activity time frames.
DISCUSSION
Diagnosis of PVNS often is difficult because the condition has an insidious and non-specific onset, usually with subtle radiographic findings. PVNS most often is found in patients between the third and fourth decades of life occurring equally in men and women, 4,7,8 although some sources show higher female prevalence. 12,24 Most patients present with monoarticular swelling and a gradual increase in pain. 4,7,8 The knee is the most common location followed by the hip, ankle, and shoulder. 20,23 However, any area with synovial tissue may be affected. There is a large discrepancy in the reported percentage of PVNS in the foot and ankle, with a range between 2.5% and 21% of the total lesions. 25
Ten Patients with Pigmented Villonodular Synovitis about the Ankle
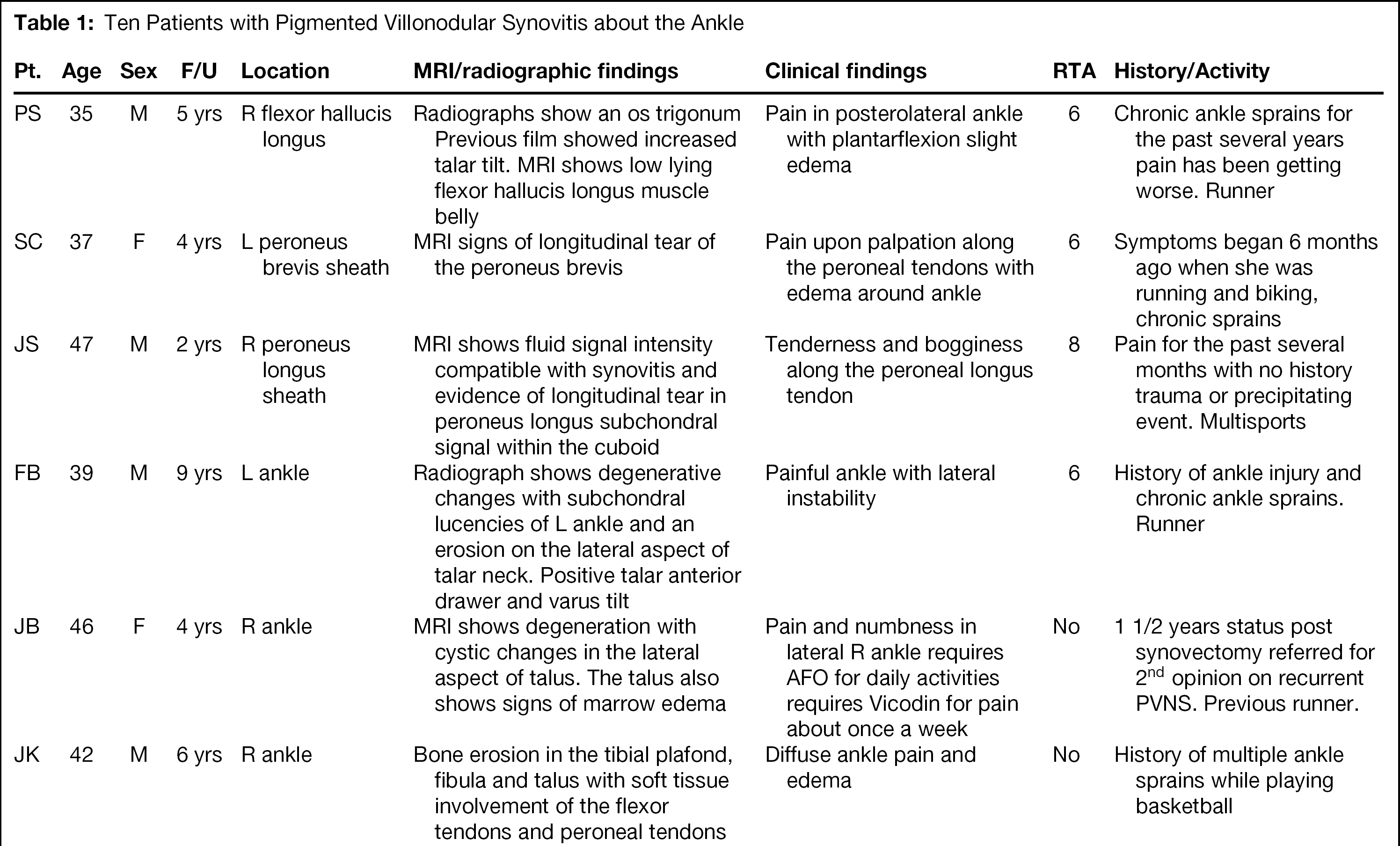
F/U = follow-up (years); RTA = return to activity (in months); No = did not return to activities.
Nine out of ten of the current patients in this series had a clear history of lateral ankle pain or recurring ankle sprains before the diagnosis of PVNS was made. Ankle sprains and anatomical variants such as os trigonum have been noted to cause chronic inflammation. This series seems to agree with the theory that PVNS is likely to develop in an area of preexisting inflammation. Unfortunately, we do not know the actual incidence of our patients seen with ankle sprains and occurrence of PVNS as compared to the incidence in the overall population. We postulate that ankle injury was the cause of chronic inflammation that served as the inciting event, leading to PVNS and therefore suggest that PVNS should be considered in the differential diagnosis of chronic ankle pain after trauma.
Chronic inflammation or history of trauma was not as evident in other reported cases of PVNS about the foot and ankle. 6,25 Ghert et al. 6 had six patients, none with a history of repetitive trauma and Rochwerger et al. 25 reported only two out of eight of patients with preexisting arthritis secondary to ankle fractures. It should be noted that the patients in our series are athletes who are more likely to have a history of trauma, such as ankle sprains, that can potentially inhibit activity. Perhaps a history of trauma was not as evident in the patients of the other series. A patient who is not an athlete might dismiss an event such as a mild ankle sprain and not report it to the treating physician.
The literature reports are in contrast with our current series in which ten lesions were found in the tendon sheaths about the ankle. The current series is too small to make conclusions on the incidence of the various anatomical locations. The occurrence of ten lesions along the ankle tendon sheaths in the athletic population does, however, suggest some common mechanism that is not present in previously described cases of PVNS in the foot or ankle. The potential for chronic inflammation after a sprain could also account for the lesions presenting in the tendons around the ankle versus the more commonly reported tendons in the toes.
The lesions often are difficult to differentiate from conditions such as rheumatoid arthritis, osteoarthritis, and other inflammatory or neoplastic processes of the synovial lining. 5 To further complicate the diagnosis, ankle PVNS often has presented as an asymptomatic mass. 6,20
Other sources have the incidence of PVNS in the foot and ankle closer to 12% and 13%. 20,24 Saxena stated in 1995, that since 1980, only eight cases in the ankle were reported. 27 The two latest series reporting PVNS in the foot and ankle showed that five out of 14 lesions were in the toes while the remaining lesions were in the joints. None of the PVNS lesions in those series were found in the tendon sheaths around the ankle. 6,25
Unmistakable bone involvement seen with plain radiograph has been noted in 15% of all cases of PVNS. 15,20 In the advanced stages, radiographic evaluation may appear similar to that of degenerative joint disease, including signs such as subchondral bone cysts and erosions of the periarticular bone with a sclerotic rim. 18 One characteristic distinguishing PVNS in a joint from degenerative joint disease is that PVNS is not associated with osteophyte formation. 28
Our current results in the ankle showed that four out of ten patients had bone erosions. Other foot and ankle PVNS series reported a much higher incidence of bone involvement. Ghert et al. 6 found that four out of six patients had bone erosions while Rochwerger et al. reported that seven out of eight had bone involvement for a combined 11 out of 14. 6,25 It stands to reason that since PVNS in a joint has direct contact with cartilage and bone erosion of bone would be common. The higher incidence of joint involvement in the previous series compared to this one could account for the apparent difference of bone involvement.
The mechanism of bone destruction by PVNS is not fully understood. It has been suggested that multinucleated cells demonstrating osteoclastic properties may arise from the synovium in PVNS. 2 The osseous and cartilaginous destruction may be mediated by matrix metalloproteinases (MMP), which also have been implicated as major contributors of cartilage destruction in inflammatory arthritidies, such as rheumatoid arthritis. 16 It has been proposed that cytokines such as TNFα, IL1, and IL6 stimulate MMP production. The cytokines released in PVNS also have been shown to have direct osteoclastic properties. 9 Because of this bone resorption, neoplastic lesions should be excluded from the diagnosis.
Partial or complete synovectomies have been considered the treatment of choice for PVNS. 8,20,24 It may be possible to locally excise nodular lesions while more diffuse lesions may require a total synovectomy. 8,20,24 PVNS is associated with a high recurrence rate, 8,12,20,24 and recurrence may be related to incomplete synovectomies. 1,20,22 When cartilage and bone are involved, bone graft or arthrodesis may be necessary. Irrigation with hydrogen peroxide or distilled water has been anecdotally reported to decrease synovial cell proliferation. Radiation treatment also has been advocated, especially in the diffuse form of PVNS or when complete synovectomy is not possible. 1,3,19
In this series, synovectomies were done on all lesions found in tendon sheaths. Two patients with cysts of the ankle required grafting with bone chips. Another patient is likely to undergo a subtalar arthrodesis for joint degeneration. The patient opted not to have an arthrodesis at the time of the resection in hopes that the excision of the lesions would alleviate the symptoms. Another patient with multiple recurrence about and within the ankle will likely need an ankle arthrodesis.
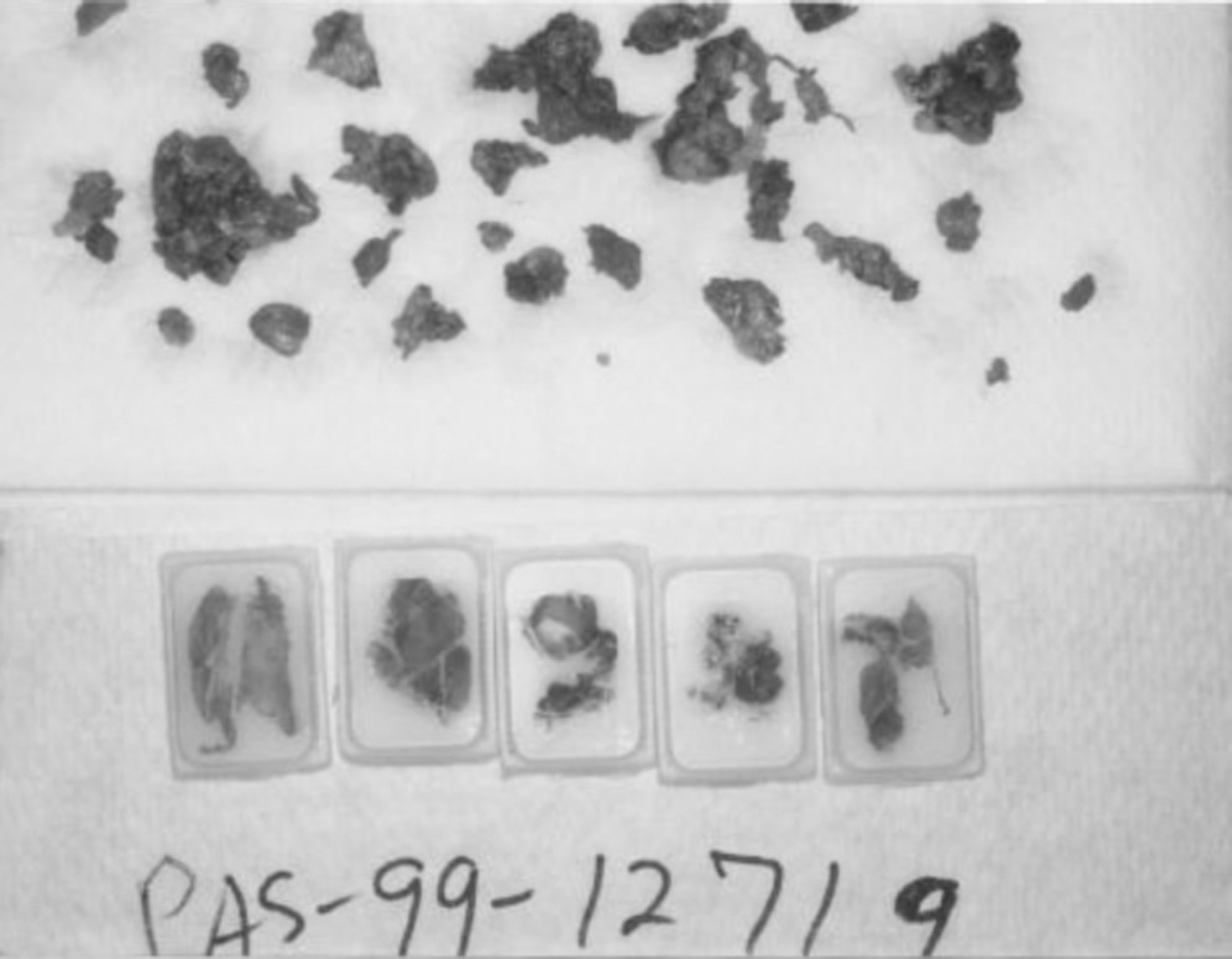
PVNS lesions may appear yellow, red, tan, or brown; the pigmentation within the lesion is due to fat and hemosiderin (Figure 1). 4,24 Histologically, PVNS may appear as a broad sheet of histiocytes with scattered lymphocytes, lipid and hemosiderin-laden foam cells, and multinucleated giant cells (Figure 2). 2,8,17 The multinucleated giant cells and the foam cells distinguish PVNS from other arthropathies (Figure 3). 8
Specimens extracted from a patient having PVNS of the ankle.
Histological slide of PVNS (50X).
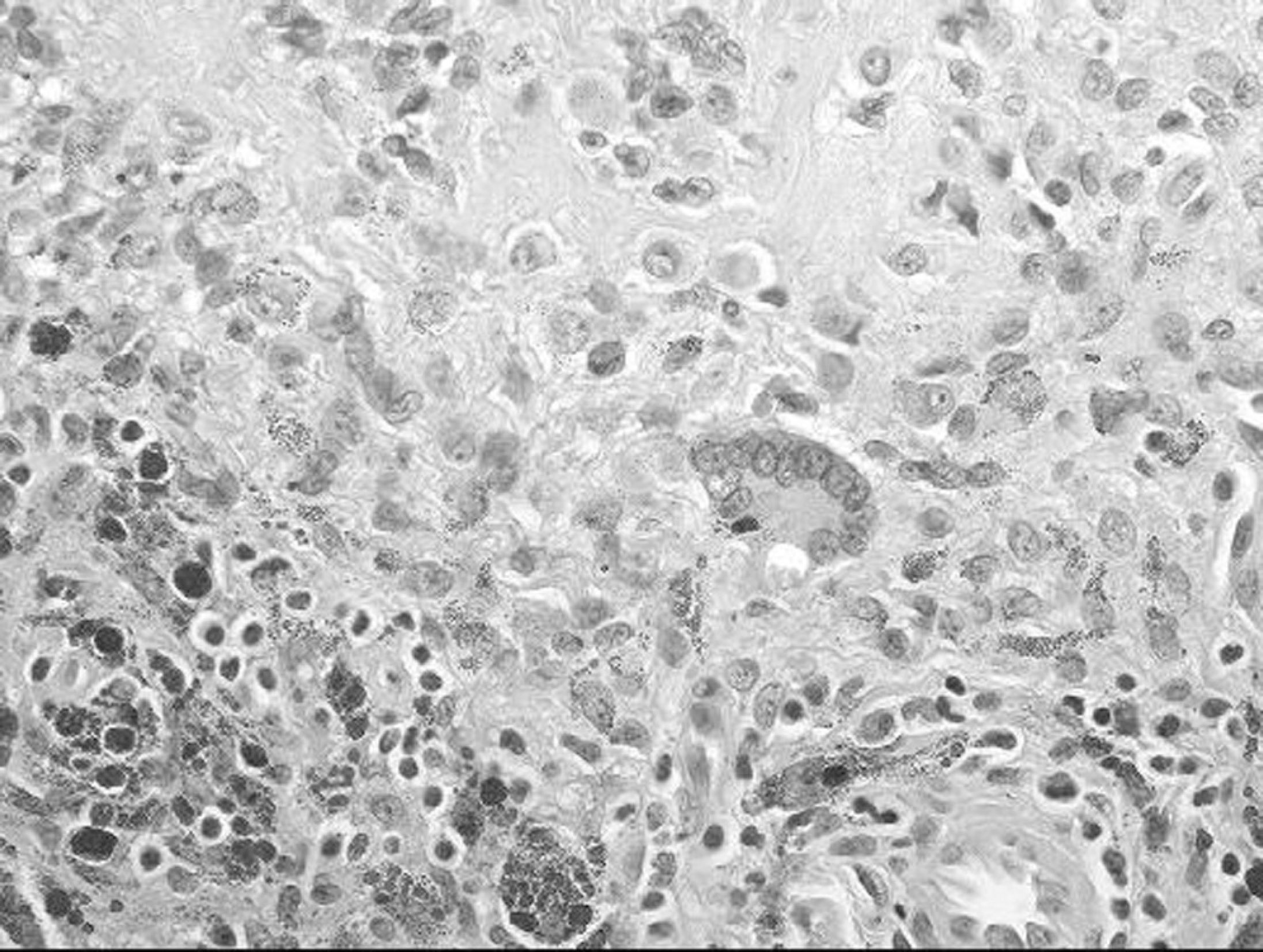
Further magnification showing giant cells, hemosiderin deposits and foam cells (100X).
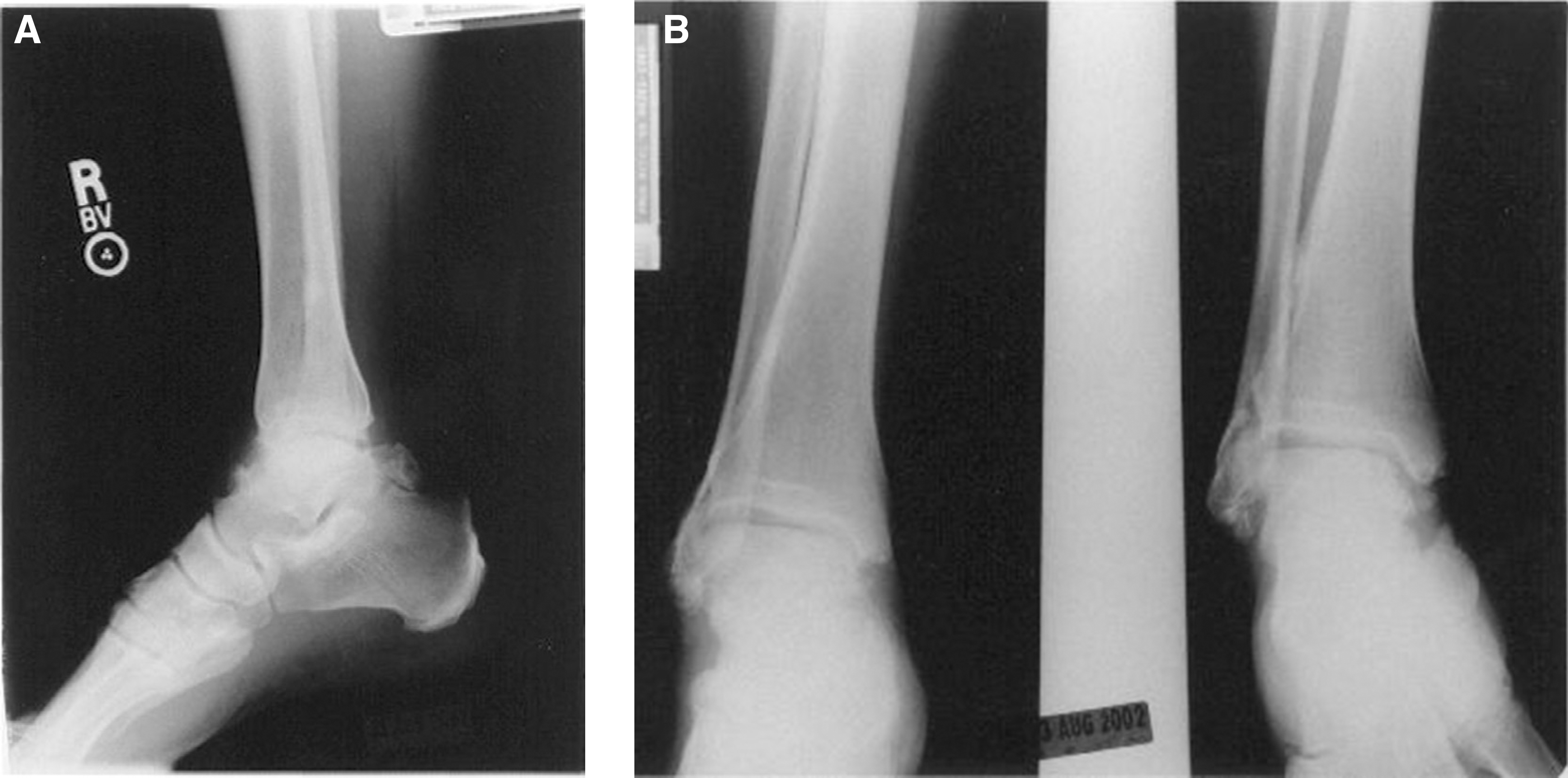
Radiographic evaluation of PVNS often depicts increased soft tissue density and can show bony erosions (Figure 4, A and 4, B). MRI reveals the hemosiderin deposits, lipids, and inflammatory tissue, making it very useful in diagnosing PVNS. 11 A low-signal intensity on both T1-and T2-weighted images is considered diagnostic for PVNS in most cases of clinically suspicious lesions. 18 Hemosiderin, with its paramagnetic effect, is what causes the decreased signal intensity. 18 If the tissue contains enough hemosiderin, it will have a low signal on all pulse sequences. 11,18 A high fat content in a lesion also helps determine the diagnosis of PVNS. 18,20 The synovial fluid surrounding the lesion may show a low or intermediate signal intensity on T1-weighted images with high-signal intensity on T2-weighted images. 11,18 MRI also is useful in determining the size, position, and invasion of cartilage or bone that may not be apparent on plain radiographs and thus helps in the preoperative planning (Figures, 5 A through D).
As early as 1941, Jaffe suggested that PVNS was caused by some reactive inflammatory response “to an unknown agent” rather than a true neoplasm. 10,26 Granowitz et al. agreed with Jaffe that PVNS has an underlying inflammatory etiology and urged for the discovery of the “inciting agent”. 8 Granowitz et al. listed infection, reactive synovitis, along with repeated trauma with hemorrhage as a possible inciting agent. 8 Synovial sarcoma also should be excluded from the diagnosis because of these findings.
Myers et al. presented 166 patients with PVNS along with a detailed analysis of the literature. 20 They reported that 53% of their patients had a history of trauma. 20 It was found that most of the literature on PVNS does not specifically report on trauma. Only 33% of 591 total cases that were reviewed from the literature specified taking a history for trauma. In those reports, 76% were positive for previous trauma. 20 More recently, based on histochemical results, researchers have postulated that chronic inflammation leads to synovial hyperplasia that predisposes synovial tissue to injury. 21 Microtrauma leads to bleeding which overwhelms the tissue's ability to dispose of the iron in the erythrocytes and thus causes pigmentation. Chronic inflammatory cell infiltrates also were found in all of their PVNS specimens studied. These findings lead to the conclusion that preexisting chronic inflammation plays an important pathogenic role in PVNS. 21 Because athletic patients may be subject to chronic repetitive inflammation, PVNS should be considered as a cause of their persistent pain and swelling.

The incidence of PVNS about the ankle have been reported to be relatively low. In athletes with a history of ankle sprains, a careful evaluation must be done. In a patient with unremitting pain, inflammation, or a palpable mass along the ankle, an MRI may be indicated. If the MRI findings show a low-intensity signal on both T1-and T2-weighted images PVNS should be suspected. Surgical management includes synovectomy and bone grafting of cystic areas, along with irrigation with hydrogen peroxide. The timely diagnosis of PVNS is advised because delay in diagnosis could lead to significant local bony and soft-tissue destruction. Long-term followup is imperative, because recurrence was the reason two out of ten patients in our series were unable to return to sports.