
Abstract
Background: The purpose of the study was to evaluate the effect of three different types of hallux valgus surgeries on patient function using validated questionnaires and to correlate the results with radiographic and physical examinations. This study presents the 2-year followup data of a previous prospective outcome study. Methods: One hundred and ninety-six patients were enrolled in this study and completed a baseline AAOS Lower Limb Outcomes Data Collection Questionnaire. They completed the same form at 6, 12, and 24 months after having one of three types of hallux valgus surgeries (106 chevron osteotomies, 72 modified McBride procedures, and 18 modified Lapidus procedures). This questionnaire included the Short Form-36 Health Survey (SF-36) as well as questions relating to lower extremity function. Additionally, physicians were asked to complete preoperative and postoperative questionnaires on each patient that included radiographic and physical examination data and the type of surgery done. Completed outcome surveys and radiographic data were available on 196 patients, and physical examination scores were available to assign an AOFAS score in 111 patients at 24-month followup. A one-way comparison was done after stratifying the results for the type of surgery, preoperative hallux valgus angle and 1-2 intermetatarsal angle, postoperative hallux valgus angle and 1-2 intermetatarsal angle, and the change in the angles. Results: Four of the 10 SF-36 scores (physical function, role-physical, bodily pain, and role-emotional) for the combined data improved by more than five points. For the AAOS lower extremity function scores, physical health and pain (68.5 to 81.6), satisfaction with symptoms (1.8 to 3.6), global foot and ankle (77.6 to 93.4), and shoe comfort (29.0 to 58.7) scores all increased significantly. The AOFAS score increased from 52.6 to 85.5 (p < 0.001). Surprisingly, when comparing mild-to-moderate to severe deformities preoperatively and postoperatively using the absolute magnitude of the angular change in the hallux valgus or intermetatarsal angles, similar improvement was noted in AOFAS, SF-36, and AAOS lower extremity scores. The magnitude of preoperative deformity, postoperative residual deformity, and magnitude of correction also did not significantly change the amount of improvement in any of these scores. No significant differences were noted in the outcome scores among the three different surgeries. Conclusion: Patients who had hallux valgus surgery had significant improvements in four of their SF-36 scores, four of five of AAOS lower extremity scores, and AOFAS scores. The degree of deformity, amount of correction, or type of operation did not influence outcome.
Keywords
Introduction
Most clinical studies in orthopaedic surgery evaluate physicians' perceptions of outcome, with a few questions regarding the patients' perceptions. The evaluation of patient perception frequently is limited to whether the patient was satisfied, satisfied with reservations, or dissatisfied. The focus of outcome research is to determine the patient's perception of outcome independent of the physician's perception. This study presents the 2-year followup data of a previous prospective outcome study that demonstrated significant improvement in patients' physical function and bodily pain and the AAOS global foot and ankle and shoe comfort sub-scores at 6- and 12-month followup. 6 The results are correlated with the type of operation, radiographic outcome, and physical examination findings using the validated AAOS Lower Limb Outcomes Data Collection Questionnaire. 3
Materials and Methods
One hundred and ninety-six patients completed the AAOS Lower Limb Outcomes Data Collection Questionnaire 24 months after one of three types of hallux valgus surgeries. This questionnaire includes the Short Form-36 Health Survey (SF-36) as well as questions relating to lower extremity function. 7 There were 180 women and 16 men with an average age of 49 (range 18 to 81) years. Sixty-seven orthopaedic surgeons, 12 in academic practice and 55 in private practice, who were active or candidate members of the American Orthopaedic Foot and Ankle Society participated in this study and completed physician data sheets.
The inclusion criteria for patients were a hallux valgus angle of more than 20 degrees, an age of 17 years or older, no inflammatory arthritis, and pain unresponsive to shoewear modification. Additionally, the surgery had to be one of three types: distal metatarsal osteotomy (chevron) (106 patients), proximal metatarsal osteotomy with distal soft tissue realignment (modified McBride) (72 patients), or metatarsocuneiform fusion with distal soft tissue realignment (modified Lapidus) (18 patients). Before surgery the patients completed a baseline AAOS Lower Limb Outcomes Data Collection Questionnaire which was given to them by their physician and then mailed to the principal investigator. Patients subsequently received a questionnaire at 6, 12, and 24-month followup from the principal investigator's office, which was then returned to the principal investigator. The six-month and 12-month data have been reported previously. 6 Institutional Review Board approval was received by the principal investigator's institution.
The data were analyzed using the Passport software developed by the American Academy of Orthopaedic Surgeons, with all of the responses manually entered into the database. The Passport software allows for automatic calculation of each of the AAOS Questionnaire sub-scales. Scores include all 10 of the SF-36 scales (physical function, role-physical, bodily pain, general health, vitality, social function, role-emotional, mental health, physical composite score, and mental composite score). Additionally there were three lower extremity scores (physical health and pain, treatment expectations, and satisfaction with symptoms) and two specific foot and ankle scores (global foot and ankle and shoe comfort).
For each participant in the study, a questionnaire was sent to the physician asking for preoperative and postoperative data on type of surgery, physical examination, and radiographic data. The five questions regarding physical examination were asked with a check-box response to allow for calculation of AOFAS hallux metatarsophalangeal-interphalangeal scores (Figure 1). Pain, function, and footwear requirement scores were obtained from the questions on the outcome survey instrument to calculate an AOFAS score (Figure 2). 4
The average and standard deviation for each score were calculated. Aggregate preoperative and postoperative scores were compared for the 10 SF-36 scores and five lower extremity scores for the AAOS instrument and AOFAS scores (Table 1 and 2). Multiple other comparisons were done by using a one-way ANOVA test to compare the type of operation, preoperative and postoperative radiographic angles, change in angles, amount of initial deformity, and the amount of residual deformity with eventual outcome. To perform the statistical evaluation, angular measurements were grouped as follows:
Preoperative hallux valgus angles: < 30°, 30° to 40°, and >40°
Postoperative hallux valgus angles: 0° to 10°, 10° to 20°, > 20°
(Two patients had a postoperative hallux valgus angle of <0° and were not included in this comparison)
Preoperative 1-2 intermetatarsal angles: <13°, 13° to 17°, >17°
Postoperative 1-2 intermetatarsal angles: 0° to 5°, 5° to 10°, >10°
Change in hallux valgus angle: 0° to 10°, 10° to 20°, >20°
Change in 1-2 intermetatarsal angle: 0° to 5°, 5° to 10°, >10°
Two-year followup questionnaires and radiographic data from the physician questionnaires were available for 196 patients. Two-year outcome questionnaires, radiographic data, and AOFAS hallux metatarsophalangeal-interphalangeal scores were available for 111 patients because only radiographic data was completed on some of the physician questionnaires.
Results
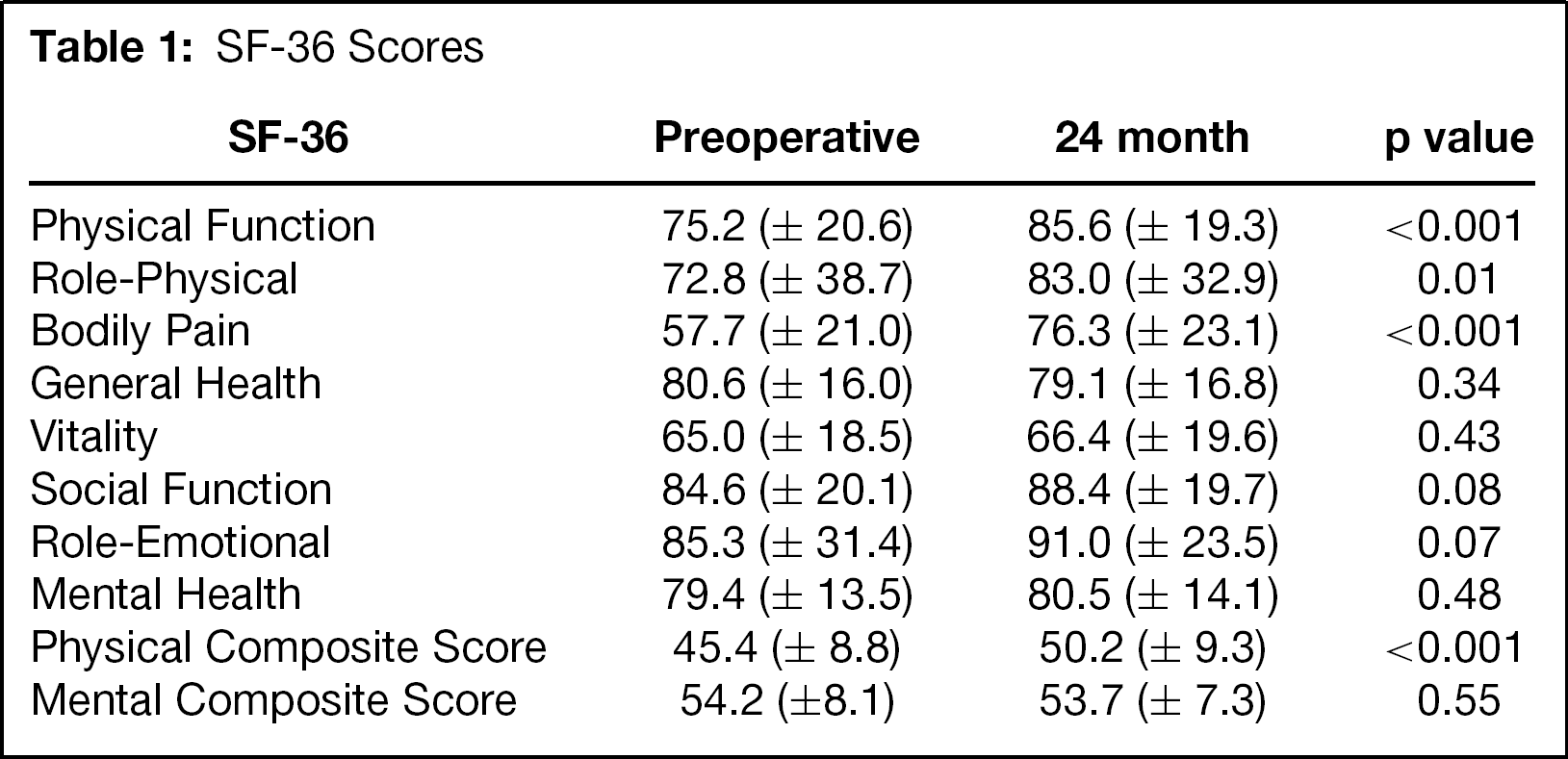
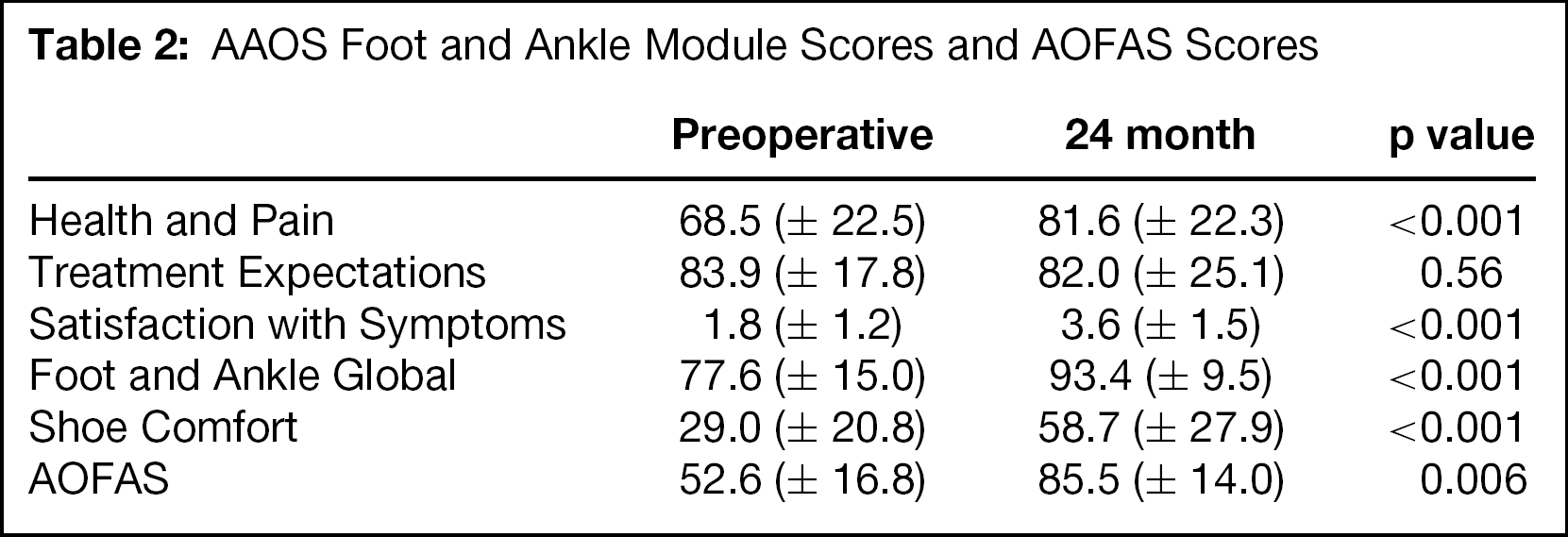
The aggregate scores at 24 months revealed that four of the 10 SF-36 scales changed by more than five points (Table 1). The lower extremity scores of physical health and pain improved from 68.5 to 81.6 (p < 0.001), satisfaction with symptoms improved from 1.8 to 3.6 (5-point scale; p < 0.001), global foot and ankle scores improved from 77.6 to 93.4 (p < 0.001), and shoe comfort improved from 29.0 to 58.7 (p < 0.001). The AOFAS score also increased significantly from 52.6 to 85.5 (p = 0.006) (Table 2).
Of the other multiple analyses performed, few showed statistically significant changes. No difference was found in any outcome score between patients who had only hallux valgus surgery (114 patients) and those who had associated procedures (82 patients). When comparing the three operations, the postoperative intermetatarsal angle was less after the chevron osteotomy (6.6 degrees) than after either the modified McBride procedure (9.7 degrees; p < 0.05) or the modified Lapidus procedure (14.3 degrees; p = 0.002). Less correction in the hallux valgus angle was noted for the chevron procedure (9.9 degrees) than for the McBride procedure (17.6 degrees; p < 0.001) and the modified Lapidus procedure (16.3 degrees; p = 0.05). The only other statistically significant difference between the types of operations was in the improvement in the bodily pain score which was 7.1 points for the modified Lapidus procedure and 23.7 points for the modified McBride procedure (p = 0.03). Surprisingly, the amount of preoperative hallux valgus and the intermetatarsal deformity had no effect on the change of any of the 15 outcome scores or the AOFAS score. Assessment of the magnitudes of change in the hallux valgus and intermetatarsal angles revealed no significant differences between mild-to-moderate and severe deformities in the most improved angular changes for any of the 15 outcome scores or AOFAS scores.
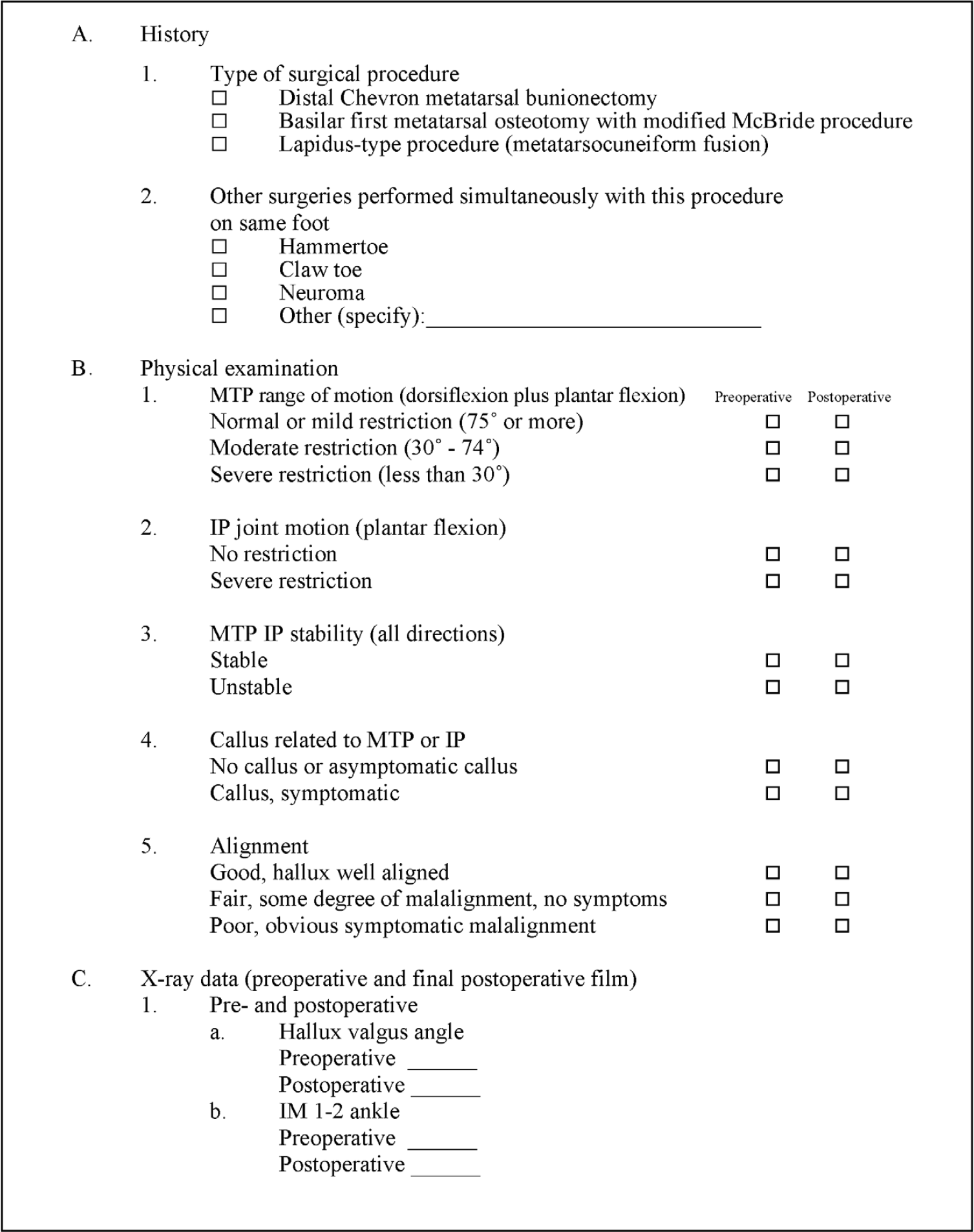
Physician Data Sheet for Outcome Study on Bunions.
Discussion
Most previous studies of hallux valgus surgery have predominantly reflected the physician's perception of outcome and have almost uniformly demonstrated successful results. The 6-month and 12-month outcome results from this patient cohort have been published previously and demonstrated statistically significant improvement in SF-36 physical function, role-physical, and bodily pain scores at 6- and 12-month follow-up. 6 The scores for the physical health and pain, satisfaction with symptoms, global foot and ankle, and shoe comfort scores also increased significantly. The 24-month data presented in this study were consistent with the improvement found at 6 months and 12 months. The current study also included calculation of the AOFAS hallux metatarsophalangeal-interphalangeal score which also showed a significant improvement from 52.6 preoperatively to 85.5 points at 2-year followup (p < 0.001).
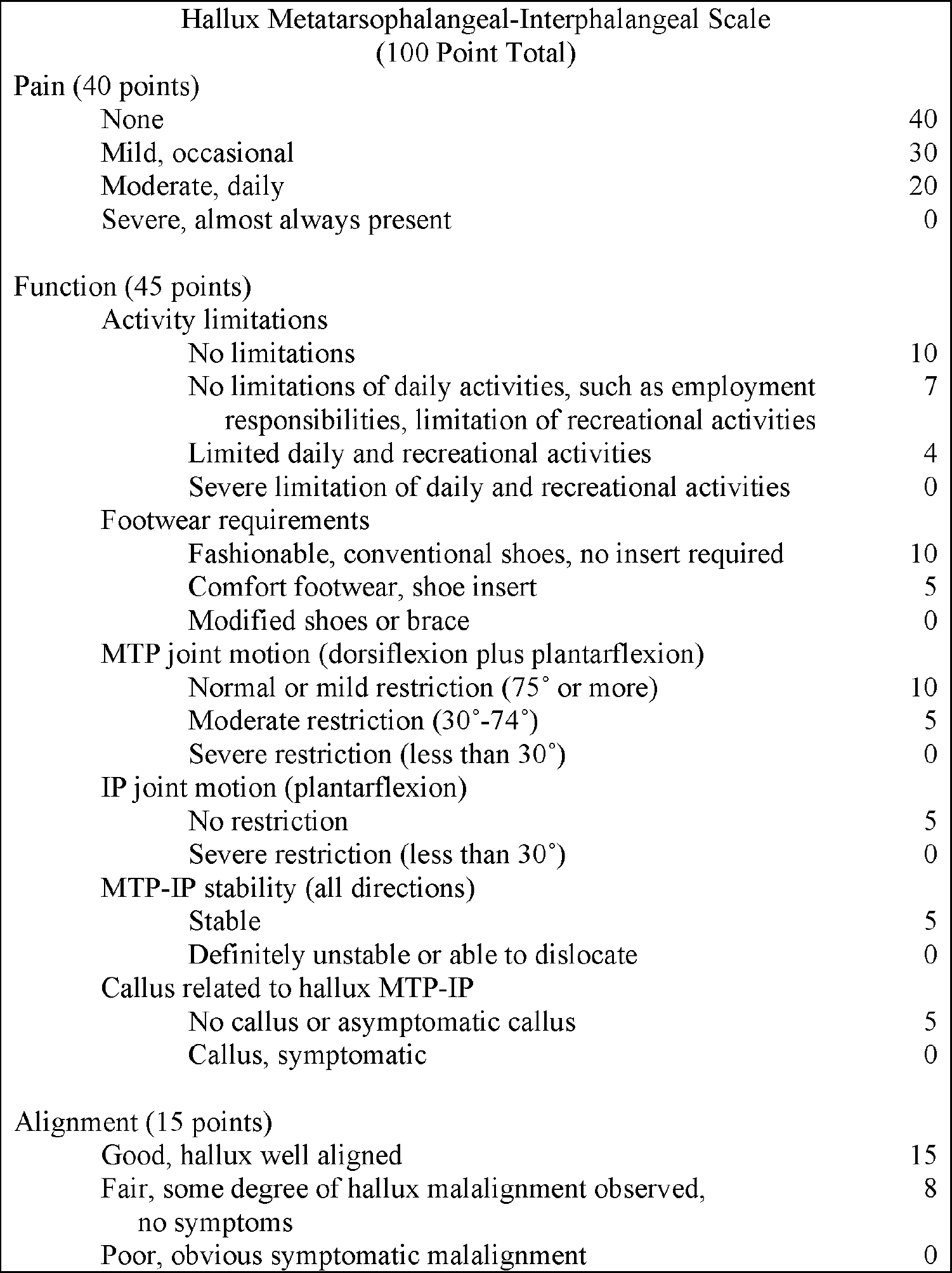
The Hallux Metatarsophalangeal-Interphalangeal Scale (100 Point Total).
Physician data on type of operation, physical examination, and radiographic measurements preoperatively and postoperatively allowed multiple additional comparisons. As expected, a smaller overall magnitude of improvement in the hallux valgus angle was noted in patients who had a chevron osteotomy than in those who had a modified McBride procedure or modified Lapidus procedure since the chevron osteotomy is indicated in patients with less severe deformities. However, most of the remaining comparisons of the outcome scores, AOFAS scores, and angular changes among the different types of operations did not show statistically significant changes. A greater postoperative intermetatarsal angle was noted for the modified Lapidus procedure (14.2 degrees) than for the chevron osteotomy and modified McBride procedure. No specific conclusions can be drawn regarding the effectiveness of the modified Lapidus procedure, because the surgical indication for the modified Lapidus, whether first metatarsocuneiform instability or the surgeon's preference of operation, was not known for the 18 patients who had the procedure.
SF-36 Scores
AAOS Foot and Ankle Module Scores and AOFAS Scores
Surprisingly, the magnitude of the deformity preoperatively reflected by the severity of the hallux valgus or 1-2 intermetatarsal angle, postoperative residual hallux valgus or 1-2 intermetatarsal angular deformity, or overall magnitude of change in the hallux valgus or intermetatarsal angle did not have a consistent effect on the 15 outcome scores or AOFAS score. Hypothetically, a more severe deformity preoperatively would have a greater overall benefit from surgical correction, or an overall greater magnitude of angular correction from surgery would lead to a greater overall improvement in outcome, or less residual deformity after surgery would lead to a better overall outcome. We found none of these three scenarios to be true. Occasional minor differences between the scores that barely reached statistical significance were noted on very few of the multiple comparisons, but no consistent change was found when any of the above parameters were assessed. It should be remembered that consistent improvements were noted between the preoperative and postoperative scores for all of the above groupings, but the magnitude of correction was essentially the same for each of the 15 outcome scores and the AOFAS score regardless of how the data were compared.
The AAOS Lower Limb Outcomes Data Collection Questionnaire includes the 36 questions which comprise the 10 subscale scores for the SF-36. 2,3 The SF-36 instrument was designed as a general health outcome instrument, which has been used to assess the outcome of orthopaedic procedures, such as total hip replacements, total knee replacements, or spine surgery, but also for many medical conditions, such as congestive heart failure, myocardial infarction, or diabetes. 6 Despite being a nonspecific instrument, physical function, role-physical, and bodily pain scores showed statistically significant improvement in patients who had hallux valgus surgery when comparing their preoperative and postoperative scores.
The foot and ankle subscale for the AAOS Lower Limb Outcomes Data Collection Questionnaire includes five additional questions from which the treatment expectation scores are derived, one additional question from which the satisfaction with symptoms score is derived, 20 questions from which the global foot and ankle scales are derived, and five questions from which the shoe comfort scales are derived. 3 The physical health and pain scale of this instrument is a simple mean of the three physical health scales (physical function, role-physical, and bodily pain) from the SF-36 portion of the questionnaire. The physical health and pain scale, derived from the SF-36, was shown to track well with physician-assessed patient function during the validity and reliability testing of the AAOS questionnaire. 1 Coincidentally, it is these three scales of the SF-36 that were noted to have a statistically significant improvement of more than five points in this study.
One potential future goal from this study, which used an outcome survey instrument with 66 individual questions, would be to derive an abbreviated questionnaire that would still yield validated outcome data for a given patient population. Although the questions are more specific for the foot region on the global foot and ankle and shoe comfort scales, only 15.5 and 25.7 point differences were noted postoperatively, respectively. This compares to an 8.6 point difference for the physical function, 10.4 point difference for the role-physical, and 18.4 point difference for the bodily pain scales of the SF-36. Thus, it did not appear that the specific subscales for the foot and ankle region were more sensitive to change than the SF-36 physical function, role-physical, or bodily pain scores. More abbreviated outcome questionnaires, such as the Foot Function Index have been developed and validated and would take less time to complete. 5
The hallux metatarsophalangeal-interphalangeal scale assigns 40 points to pain, 45 points to function, and 15 points to alignment. 4 This study demonstrated a significant improvement in AOFAS scores from 52.6 preoperatively to 85.5 postoperatively. Although it correlates well with the change in outcome scores, the correlation is somewhat artificial. Fifteen points of the AOFAS hallux metatarsophalangeal-interphalangeal scale are assigned for alignment. With a good surgical result, a patient will receive the maximum 15 points for the alignment scale, and presumably preoperatively they would receive 0 points for “obvious, symptomatic malalignment.” Thus, 15 points of the improvement reported would be from the radiographic improvement, which does not necessarily correlate with patient outcome. Pain would be expected to improve 10 to 20 points on this scale, as the patients frequently reported “moderate daily pain preoperatively which correlates to a score of 20. Most patients reported “mild and occasional pain” postoperatively with some reporting “no pain whatsoever” leading to a 30 or 40 point score, or a 10 to 20 point improvement. Most patients had no activity limitations and only lost five points out of a total of 10 for footwear requirements, as they were able to wear comfortable shoes preoperatively. Postoperatively, most patients resumed fashionable or conventional shoes without an insert for a full 10-point score. Very few physicians reported a change in metatarsophalangeal joint motion, interphalangeal joint motion, metatarsophalangeal-interphalangeal joint stability, or a callus related to the hallux metatarsophalangeal or interphalangeal joints preoperatively or postoperatively. Thus, most patients would be expected to gain 30 points in the AOFAS score for a good result and 40 points for an excellent result based on this scoring system, which correlated well with our change of 32.9 points. While the AOFAS score improved, we believe the SF-36 bodily pain, role-physical, physical function scales, and the global foot and ankle shoe comfort scores to be most responsive, because the scoring systems are based on continuous variables generated from the patients' perspectives of their outcomes.
In summary, this study has demonstrated that patients had significant improvements in physical function, role-physical, and bodily pain SF-36 scores after hallux valgus surgery. Additionally, physical health and pain, satisfaction with symptoms, global foot and ankle, shoe comfort and AOFAS hallux metatarsophalangeal-interphalangeal scores also significantly improved. The degree of improvement was not noted to be influenced by the preoperative or postoperative hallux valgus or 1-2 intermetatarsal angles, the magnitude of change of these angles, the residual deformity, or the type of surgery.
Corresponding author will provide additional descriptive data tables upon request.