
Abstract
Background: Although vacuum-assisted closure (VAC) is a well-established technique in other surgical specialties, its use has not been established in the foot and ankle. The aims of this study were to determine if vacuum-assisted closure therapy (VAC) helps assist closure in diabetic foot ulcers and wounds secondary to peripheral vascular disease, if it helps debride wounds, and if it prevents the need for further surgery. Methods: We retrospectively reviewed 15 patients (18 wounds or ulcers) with primary diagnoses of diabetes (10 patients), chronic osteomyelitis (two patients), peripheral vascular disease (two patients), and spina bifida (one patient). Eleven of the 15 patients had serious comorbidities, such as peripheral neuropathy, renal failure, and wound dehiscence. All wounds were surgically debrided before VAC therapy was applied according to the manufacturer's instructions. The main outcome measures were time to satisfactory wound closure, changes in the wound surface area, and the need for further surgery. Results: Satisfactory healing was achieved in 13 of the 18 wounds or ulcers at an average of 2.5 months. VAC therapy failed in five patients (five class III ulcers), three of whom required below-knee amputations. Wound or ulcer size decreased from an average of 7.41 cm 2 before treatment to an average of 1.58 cm 2 after treatment. Conclusion: VAC therapy is a useful adjunct to the standard treatment of chronic wound or ulcers in patients with diabetes or peripheral vascular disease. Its use in foot and ankle surgery leads to a quicker wound closure and, in most patients, avoids the need for further surgery.
INTRODUCTION
The vacuum-assisted closure (VAC) negative-pressure technique has been used to assist wound closure after plastic and reconstructive, 1,7,8,16,18 cardiothoracic, 17 gynecologic, 2 and general surgical procedures, 5 but its use in foot and ankle surgery has been limited. In addition to isolated reports of the use of this technique in foot and ankle surgery, Clare et al, 6 in 2002, reported that in 17 patients with diabetes mellitus, peripheral vascular disease, and osteomyelitis the VAC technique resulted in marked improvement of wound healing. The technique is designed to remove chronic edema fluid to decrease the after-load to blood flow and increase localized blood perfusion. 1,16 The reduction of edema combined with the application of negative-pressure forces enhances the formation of granulation tissue, and the VAC technique has been shown to effectively stimulate healing by secondary intention. 1,16 The aims of our study were to determine if VAC therapy (1) resulted in quicker wound closure in patients with diabetes or ischemia, (2) helped to debride wounds, and (3) prevented the need for further surgery.
MATERIAL AND METHODS
After approval by our Institutional Review Board, retrospective review identified 15 patients with 18 chronic, nonhealing wounds or ulcers on the foot and ankle. The average age of the nine males and six females was 49.3 (22 to 80) years. These patients were followed for an average of 6.3 (1 to 18) months. Primary diagnoses were insulin-dependent diabetes mellitus (IDDM) in eight, noninsulin dependent diabetes mellitus (NIDDM) in two, chronic osteomyelitis in two, peripheral vascular disease (PVD) in two, and spina bifida in one. All but three of the 15 patients had serious comorbidities (Table 1). Five of the patients with diabetes mellitus also had PVD, one of whom had chronic osteomyelitis. Three of those with diabetes also had peripheral neuropathy. Of the 15 patients, seven had PVD with ankle brachial pressure indices of less than 0.6, confirmed on continuous-wave Doppler examination. Efforts at revascularization in these patients included bypass procedures and angio-plasties, all of which failed. Five patients had postoperative wound dehiscence before application of the VAC device.
Eight of the 18 wounds were located in the forefoot or midfoot, seven were in the ankle or hindfoot, and three were in the lower leg. Eleven were class III ulcers (Wagner-Meggitt classification 15,19 ) and seven were class II ulcers. In the 10 diabetic patients, there were seven class III ulcers down to exposed tendon and bone. Eleven patients had clinical evidence of active infection and were given broad-spectrum systemic antibiotics.
All wounds had failed to heal after treatment with wound dressing and debridement; two patients had amputations before VAC therapy, and one had application of an external fixator for an open tibial fracture.
Before application of the VAC device (Kinetic Concepts, Inc., San Antonio, Texas), surgical debridement removed all devitalized necrotic tissue, including bone in some patients, and the wound was packed with proflavin. Twenty-four to 48 hours later, the VAC negative-pressure device was applied according to the manufacturer's instructions.
All patients were followed until satisfactory wound healing occurred or failure of healing was evident. At each follow-up examination, wound dimensions (length × breadth in centimeters) were recorded and clinical photographs were obtained to objectively evaluate wound shrinkage and formation of granulation tissue.
Application of the VAC device
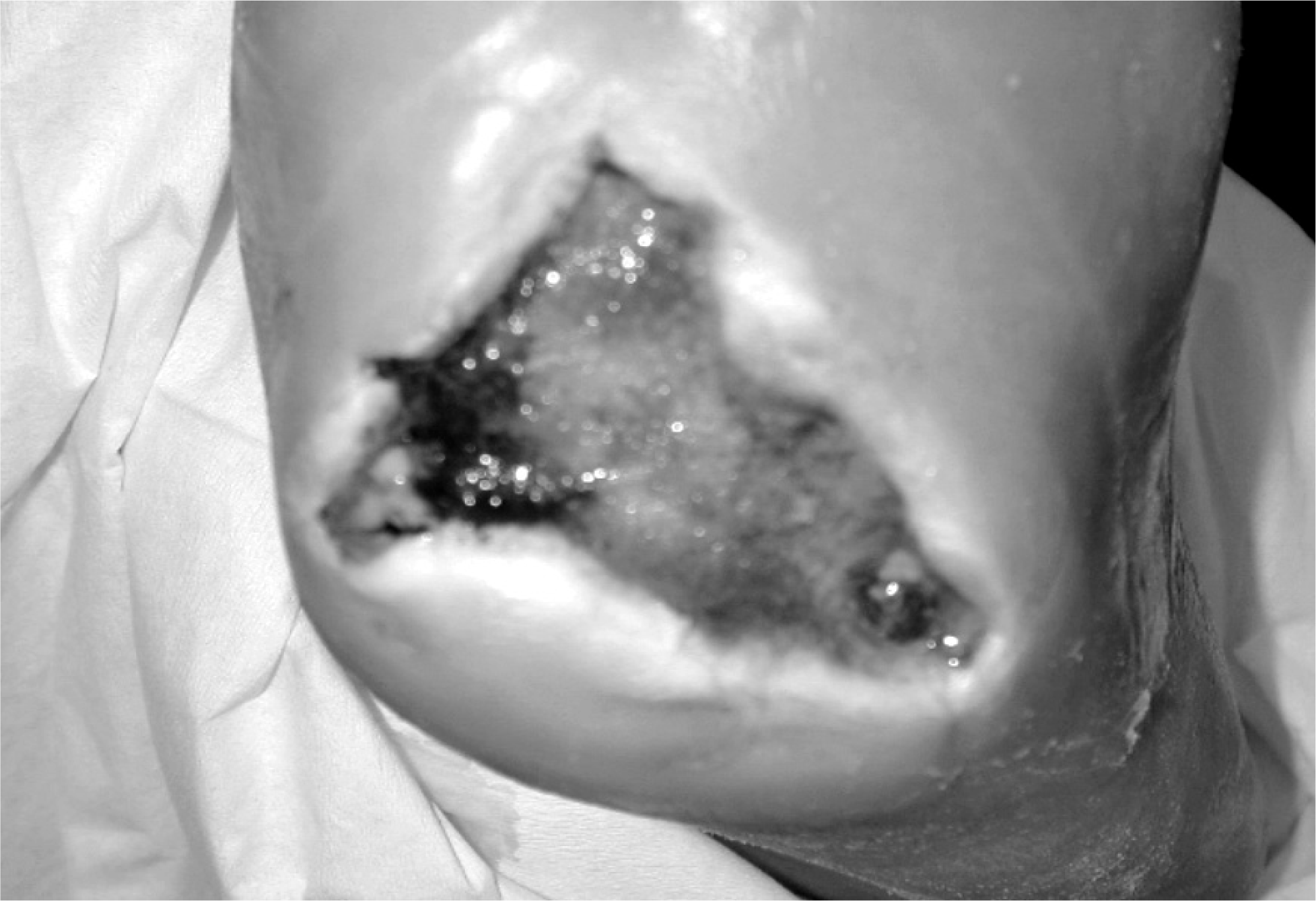
The VAC device contains an open-cell foam dressing into which is embedded an evacuation tube, which exits parallel to the skin surface. The tube is connected to a collection container, and the effluent from the wound is drawn into the collection container when negative pressure is applied. The container is connected to an adjustable vacuum pump that regulates the negative pressure. The foam dressing was trimmed and fitted according to the dimensions of the wound and was placed in direct contact with the base of the wounds. Adhesive tape was applied around the dressing, extending 3 to 5 cm beyond the margins of the wound to create an airtight seal (Figure 1). For the first 48 hours, 125 mm Hg of continuous negative pressure was applied. Then the dressing was changed and intermittent pressure cycles of 5 minutes on and 2 minutes off were applied. The open wound was thus converted to a controlled closed wound environment. 1 Those who were treated as outpatients were given mini-VAC portable devices. The VAC device was used until the wound was either completely healed or had progressed to a stage where skin grafting or simple wound dressings could achieve satisfactory wound closure.
RESULTS
Satisfactory healing was obtained in 13 of the 18 wounds or ulcers in an average of 2.5 (1 to 6) months, thus avoiding further treatment such as re-debridement or amputation. VAC therapy failed in five patients (five class III ulcers), three of whom required below-knee amputations. Wound or ulcer size decreased from an average of 7.41 cm 2 (2 to 10 cm 2 ) before treatment to an average of 1.58 cm 2 (0 to 2 cm 2 ) after treatment. Of the 13 ulcers in the 10 diabetic patients, 11 in nine patients healed completely. The other two were in patients who were noncompliant with treatment and followup protocols; one eventually required a forefoot amputation and the other a first ray amputation.
DISCUSSION
Argenta et al. 1 reported the use of the VAC technique in 300 patients with nonhealing ulcers, 99% of which healed. They concluded that the VAC negative-pressure technique significantly increased rates of granulation tissue formation and local blood supply and was a useful adjunct to wound care. While not as good as the results of Argenta et al., our results were comparable to those of Clare et al. 6 and confirm the effectiveness of this technique in the treatment of chronic nonhealing wounds or ulcers of the foot and ankle. They reported severe PVD as the most common reason for failure of VAC in their series and suggested that patients with severe PVD should be treated by other methods. In our seven patients with PVD, five of whom had diabetes, VAC therapy failed in three. Ford et al. 10 reported improved results in patients with chronic osteomyelitis after VAC treatment. They postulated that the negative pressure created by the vacuum device facilitates antibiotic absorption from surrounding capillaries into the bone, thus reducing infection. VAC therapy failed in all three of our patients who had chronic osteomyelitis, all of whom also had PVD and one had IDDM.
Demographics and Treatment
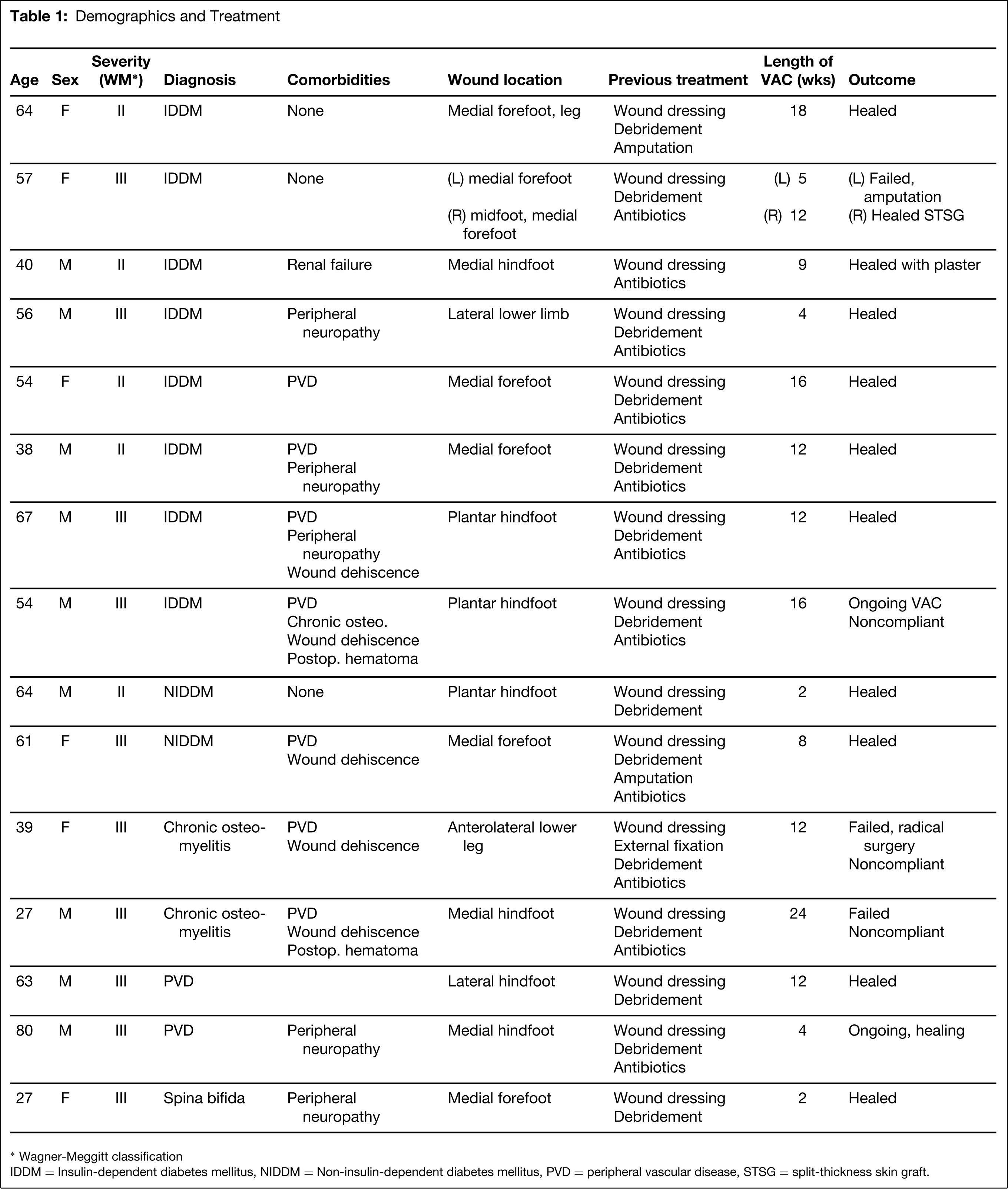
Wagner-Meggitt classification
IDDM = Insulin-dependent diabetes mellitus, NIDDM = Non-insulin-dependent diabetes mellitus, PVD = peripheral vascular disease, STSG = split-thickness skin graft.

Vacuum-assisted closure (VAC) device applied on an ulcer on the heel of a diabetic patient.
After VAC application, epithelial closure of the wound is complete.
The precise mechanism by which the VAC negative-pressure technique effects wound closure is unknown. Morykwas et al. 16 showed in a pig model that peak blood flow levels were four times higher than base line values with continuous pressures of 125 mmHg. They also found a significantly higher rate of granulation tissue formation and a significant decrease in bacterial flora after 4 to 5 days of treatment. Clinical and experimental studies have shown that removal of third-space fluid resulted in a decrease in tissue turgor and a decrease in capillary after-load, which promoted capillary circulation and inflow. In addition, the removal of excess exudates from the wound is believed to remove inhibitory factors which inhibit vascularity. These fluids contain high levels of matrix metalloproteinases and their degradation products, and these have been shown to suppress the proliferation of keratinocytes, fibroblasts, and vascular endothelial cells in vitro. 20 Bacterial counts in human wound tissues treated with the VAC technique have demonstrated significant decreases after 3 to 4 days, paralleling the results of animal studies. Because the negative pressure applies uniform, controlled tension to every point on the inner surface of the wound, the sum of the applied forces becomes large and tends to draw the edges of the wound inward. Prospective, randomized trials have showed a decrease in the ulcer volume and in the mean number of polymorphous neutrophils and lymphocytes in wounds treated with VAC. 9,19
Clare et al. 6 described some practical problems in the use of VAC for treatment of wounds located over a small area, especially the midfoot and forefoot area. We encountered few problems with this and were able to apply the VAC technique to eight forefoot and midfoot ulcers, seven of which healed. Other reported complications of the VAC technique include localized infection, bleeding, increased pain, bad odor, and toxic shock syndrome. 1,7,14 None of these complications occurred in our patients, except for a bad odor when dressings were changed. Three of the five patients in whom VAC was unsuccessful were noncompliant with treatment and followup protocols. The development of the mini-VAC portable device may promote better compliance because treatment can be done on an outpatient basis.
Our results add to the growing evidence that VAC is a useful adjunct to the standard treatment of chronic wounds or ulcers of the foot and ankle in patients with diabetes or peripheral vascular disease. Its use may avoid the need for further debridement or amputation. More long-term, randomized, controlled trials are needed to clearly establish its benefits.