
Abstract
Background: The Agility (DePuy, Warsaw, Indiana) total ankle replacement has been in use since 1984. One of the most common complications continues to be delayed union or nonunions of the distal tibiofibular syndesmosis. In the reported studies on the Agility ankle the delayed union and nonunion rate can be as high as 38%. Methods: Since 1999, 114 Agility total ankle replacements were done at two centers in the United States without the use of autologous concentrated growth factors. Since July of 2001, 66 Agility ankles were implanted with Symphony (DePuy, Warsaw, Indiana) augmented bone grafting. The standard operative technique was followed in all the patients. Prospective data was collected on all patients. The standard ankle radiographs were taken preoperatively and postoperative at 8 weeks, 12 weeks, 16 weeks, 6 months, and yearly. CT scans were obtained at 6 months if fusion at the syndesmosis was questionable. The Graphpad Instat software (Graphpad Software Inc., San Diego, CA) was used for statistical analysis. The two-tailed unpaired t-test was used, and the value <0.05 was considered significant.Results: There was no statistical difference in the demographic data for the two groups. In 114 ankle replacements without autologous concentrated growth factors 70 fused at 8 weeks (61%), 14 fused at 12 weeks (12%), 13 fused at 6 months (12%). There were 17 nonunions (15%); delayed unions (3 to 6 months) and nonunions, therefore, equaled 27%. The syndesmosis fused in 50 of the 66 ankle replacements (76%) that had autologous concentrated growth fractures at 8 weeks (76%); 12 fused at 3 months (18%), 2 fused at 6 months (3%), 2 had nonunions (3%). Delayed unions (3 to 6 months) and nonunions equaled 6%. There was a statistically significant improvement in the 8- and 12-week fusion rates, and a statistically significant reduction in delayed unions and nonunions. Conclusion: Autologous concentrated growth factors appear to make a significant positive difference in the syndesmosis union rate in total ankle replacements.
INTRODUCTION
Total ankle arthroplasty has regained some interest in the past decade. Early in the evolution of ankle replacements problems with component design, prosthesis fixation, operative technique, and patient selection led to early failures. 29,14 For a while there was a strong appeal to abandon total ankle replacement in favor of ankle arthrodesis. 6,16,19,30
During the mid to late 1980s, second generation systems attempted to correct some of the flaws associated with their predecessors. These ankle replacements systems are still undergoing modifications as new technologies and research data are evaluated. 31,20 Also, advancements in biological agents, 34 with a history of application in other areas of orthopaedic surgery, are now finding applications in ankle replacement surgery. With improved operative techniques and new component materials, total ankle arthroplasty is possibly returning as a viable option in the treatment of patients with debilitating ankle arthritis for whom conservative treatment has failed to alleviate symptoms.
The Agility ankle (DePuy, Warsaw, Indiana) was first used in 1984, and the system has undergone five phases of development since. 31,33 These modifications have improved function and ease of application.
The unique design of the Agility ankle incorporates the distal tibiofibular syndesmosis to support the tibial component, allowing for a much larger bone surface, with the theoretical advantage that it will limit the prevalence of tibial component subsidence. Distal tibiofibular syndesmosis fusion is therefore essential for the success of this ankle arthroplasty.
In a review of the first 100 Agility ankle arthroplasties, the nonunion rate of the syndesmosis was found to be 9% and the delayed union rate (defined as longer than 6 months) was 29%. 31 Migration of the tibial component was related to nonunion and delayed union of the syndesmosis. Improving the rate of distal tibiofibular syndesmosis fusion is expected to decrease the migration rates of the tibial component and, consequently, improve the function and long-term survival of the prosthesis.
In 1965, Urist demonstrated that demineralized bone matrix could induce de novo bone formation. 40 Growth factors in this matrix include transforming growth factor beta (TGF-β), platelet-derived growth factor (PDGF), insulin-like growth factors (IGFs), and fibroblast growth factor (FGF). 12 Bone morphogenic protein (BMP) is a member of the TGF-β super-family. 32 In vitro assays have shown that these same growth factors are carried by platelets. 34 As the healing cascade of bone occurs, the initial phase is characterized by inflammation and hematoma formation at the site of injury. Many growth factors found in platelets are released during platelet degranulation in this initial phase after tissue injury. 34 The signals for cellular chemotaxis, differentiation, and osteoblastic proliferation are controlled by these growth factors. 5,37,38 Proliferation of marrow stromal cells and recruitment of undifferentiated mesenchymal cells then occur forming woven bone, which is remodeled to lamellar bone. 11 Growth factors from an autologous platelet concentrate have been successful in inducing bone formation in both animal and human studies, 7,24,25,26 and this effect probably is attributable to the growth factors contained in platelet concentrate.
Symphony PCS (DePuy, Warsaw, Indiana) is a system in which a platelet concentrate is prepared from a 55 cc volume of autologous blood. The volume is centrifuged, and the platelet rich layer is combined with thrombin to produce a concentrate gel with four to six times the normal concentration of platelets. The gel is then sprayed directly onto the prepared bone surfaces and mixed with the autologous bone graft.
The purpose of this study was to determine whether the use of an autologous platelet concentrate would improve the rate of distal tibiofibular joint fusion after total ankle arthroplasty.
MATERIALS AND METHODS
Since 1999, 114 Agility total ankle replacements were done at two centers in the United States without the use of autologous concentrated growth factors. Since July of 2001, 66 Agility ankle replacements were done at the same two centers, by the same two surgeons, (JCC and GCP) using autologous platelet concentrate (Symphony PCS: DePuy, Warsaw, Indiana).
The Agility ankle prosthesis was used in both group A and group B. In group A, standard syndesmotic fusion group, the average age was 63 (range 40 to 83) years. There were 53 women and 61 men. The average weight was 188 lbs. Four patients had rheumatoid arthritis and 100 had primary or post-traumatic arthritis. Twenty-two patients were smokers (19%).
In group B, syndesmosis fusion with autologous concentrated growth factors group, the average age was 64 (range 41 to 79) years. There were 29 women and 37 men. The average weight was 192 pounds. Two patients had rheumatoid arthritis, and 64 had primary or post-traumatic arthritis. There were 15 smokers in this group (23%).
During that time there were no major changes in the actual components or operative technique that could have influenced the outcome.
Prospective data were collected on all patients and included the AOFAS ankle and hindfoot scale, demographic information, patient satisfaction, and a visual analog pain scale. This information was gathered preoperatively, at 6 months, and yearly thereafter.
The standard ankle radiographs were taken preoperatively and postoperatively at 8 weeks, 12 weeks, 16 weeks, 6 months, and yearly. The radiographs were evaluated by an independent qualified radiologist. CT scans were obtained at 6 months if fusion of the syndesmosis was questionable. Complete syndesmotic fusion was defined as bony trabeculae spanning the distal tibiofibular joint seen in the mortise and anteroposterior views.
The Graphpad Instat Software (Graphpad Software, Inc., San Diego, CA) was used for statistical analysis. The two-tailed unpaired t-test was used, and the value <0.05 was considered statistically significant.
Operative Technique
The operative technique was as described by Alvine. 1 An external fixator was placed medially with pins in the neck of the talus and the calcaneus distal to the ankle joint and in the medial tibial shaft proximally. The joint was distracted approximately 5 mm. Subperiosteal dissection over the distal tibia was done to expose an area approximately 5 to 6 cm proximal to the ankle joint for placement of the cutting jig. A lateral incision was made to expose and prepare the distal tibiofibular syndesmosis for arthrodesis. Soft tissue was removed from the distal tibiofibular syndesmosis, and then a 2mm drill was used to prepare the lateral surface of the tibia and the medial surface of the fibula for fusion. Multiple holes were drilled into the opposing surfaces to promote fusion. An alternative was to use a small osteotome to decorticate the surfaces. An alignment guide was positioned along the tibial spine from the tibial tubercle to the anterior distal tibia. Biplanar adjustment was done to match the anatomy of the tibia and ankle. Equal bone cuts were removed from the tibia and talus with an appropriate cutting jig. The positions of the cuts were verified using fluoroscopy. The resected bone that was saved for autograft was morselized and prepared.
In the second group the bone was mixed with the Symphony PCS autologous platelet concentrate. With the Symphony PCS, 55 ml autologous blood was centrifuged, and the platelet rich layer was combined with thrombin to produce a concentrated gel with four to six times the normal concentration of platelets. The gel was then sprayed directly onto the prepared bone surfaces and mixed with the autologous bone graft. There usually was about 5 ml of the concentrate, and most of it was mixed into the bone graft. Trial components were tested first followed by the implants. Bone graft was placed in the syndesmosis and over the anterior fins of the tibial and talar components. Two 4.5-mm cortical screws were used to compress the fibula against the tibia for fusion.
The wound was closed in layers, and a sterile dressing and a posterior bulky splint holding the ankle in neutral dorsiflexion were applied. Dressings were removed at 2 weeks, and a short leg nonweightbearing cast was applied. Patients were kept nonweightbearing with the ankle held in neutral dorsiflexion for a total of 8 weeks. At the 5-week postoperative visit patients who had less than 10 degrees of dorsiflexion were enrolled in physical therapy for ankle range-of-motion exercises and were splinted in a removable cast. Full weightbearing was begun at 8 weeks if the syndesmosis appeared to have fused and the components were stable in the ankle (Figure 1).
If the syndesmosis was not completely fused at 8 weeks, patients wore a cast walker boot to begin weightbearing (Figures 2 through 4).
RESULTS
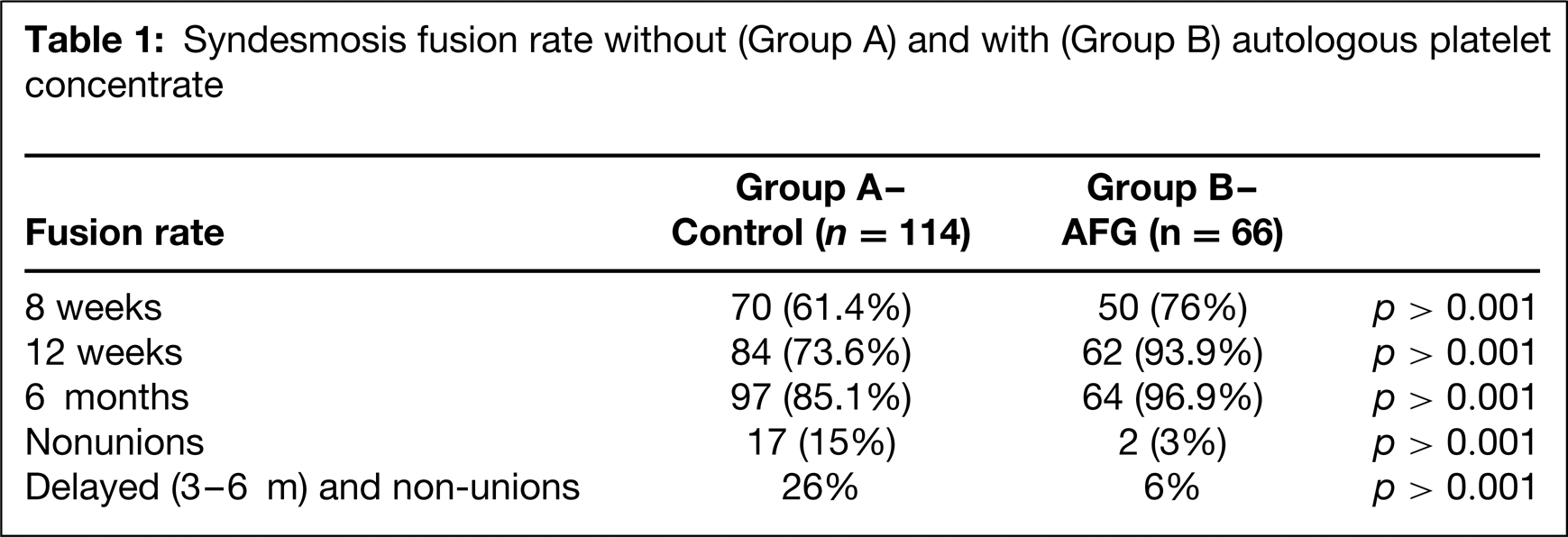
There was no statistical difference in the demographic data between the two groups. The results of a standard syndesmosis fusion and the fusions with autologous platelet treatment are summarized in Figure 5 and Table 1.
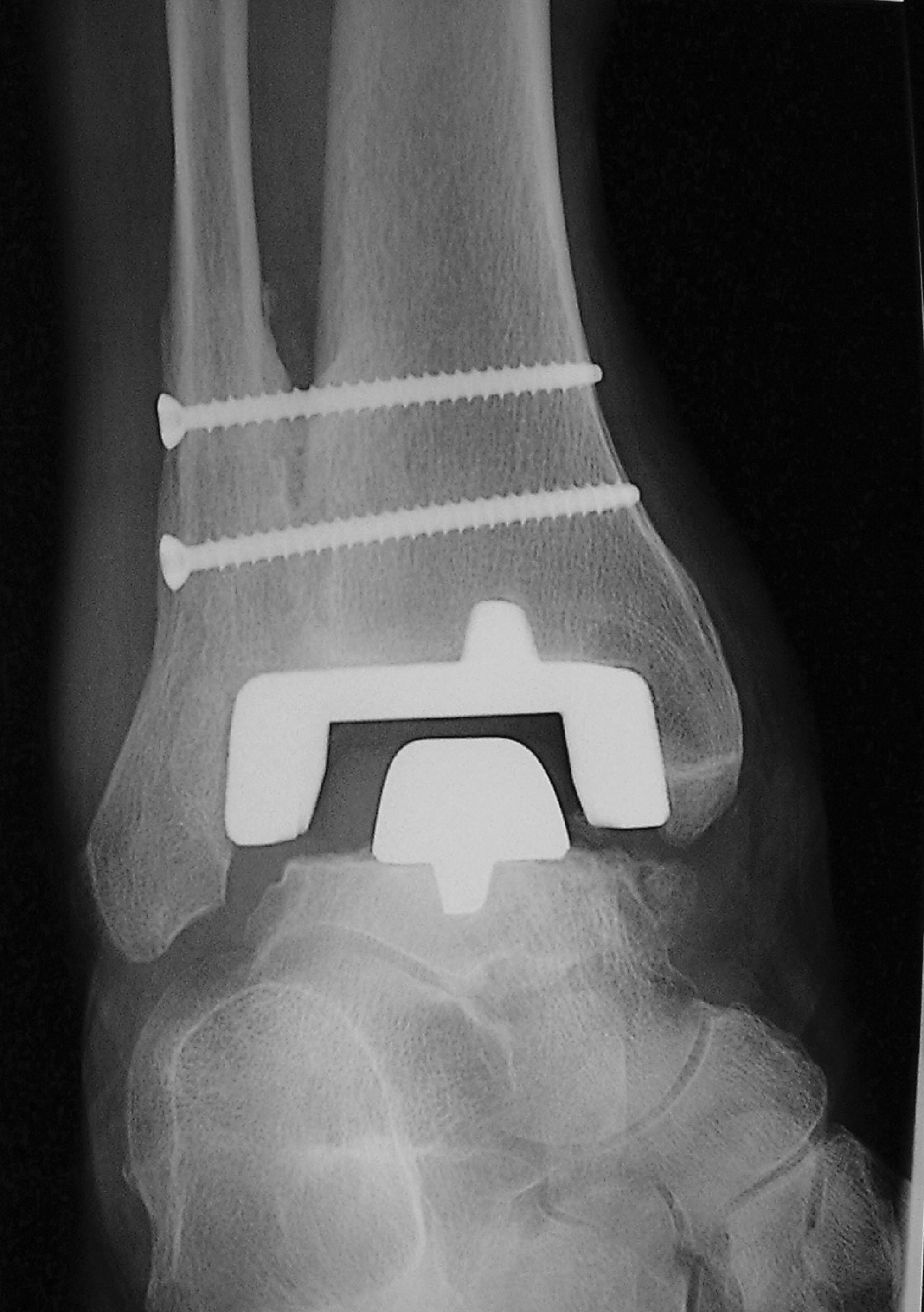
Solid syndesmosis fusion.
There was a statistically significant improvement in the 8- and 12-week fusion rates, and a statistically significant reduction in delayed unions and nonunions at 6 months. Of the 66 prosthetic ankles that were implanted using the standard technique augmented with autologous platelet concentrate, 50 (76%) were judged to have a solid distal tibiofibular fusion at 8 weeks postoperatively compared to 70 (61.4%) in the control group (n = 114). At 12 weeks postoperatively, 62 patients (93.9%) in the autologous platelet augmented group achieved fusion compared with 84 patients (73.6%) using the standard technique without platelet concentrate. Sixty-four of 66 patients (96.9%) had fusion of the syndesmosis at 6 months in the autologous concentrate augmented group compared to 97 of 114 (85.1%) in the control group.
If the timeframe 3 to 6 months is considered a delayed union, the combined delayed unions and nonunions included four patients (6%) in the autologous concentrate augmented group compared with 31 (27%) in the control group. Of the smokers, 50% achieved fusion in the control group at 6 months compared to 20% in the autologous concentrate group.
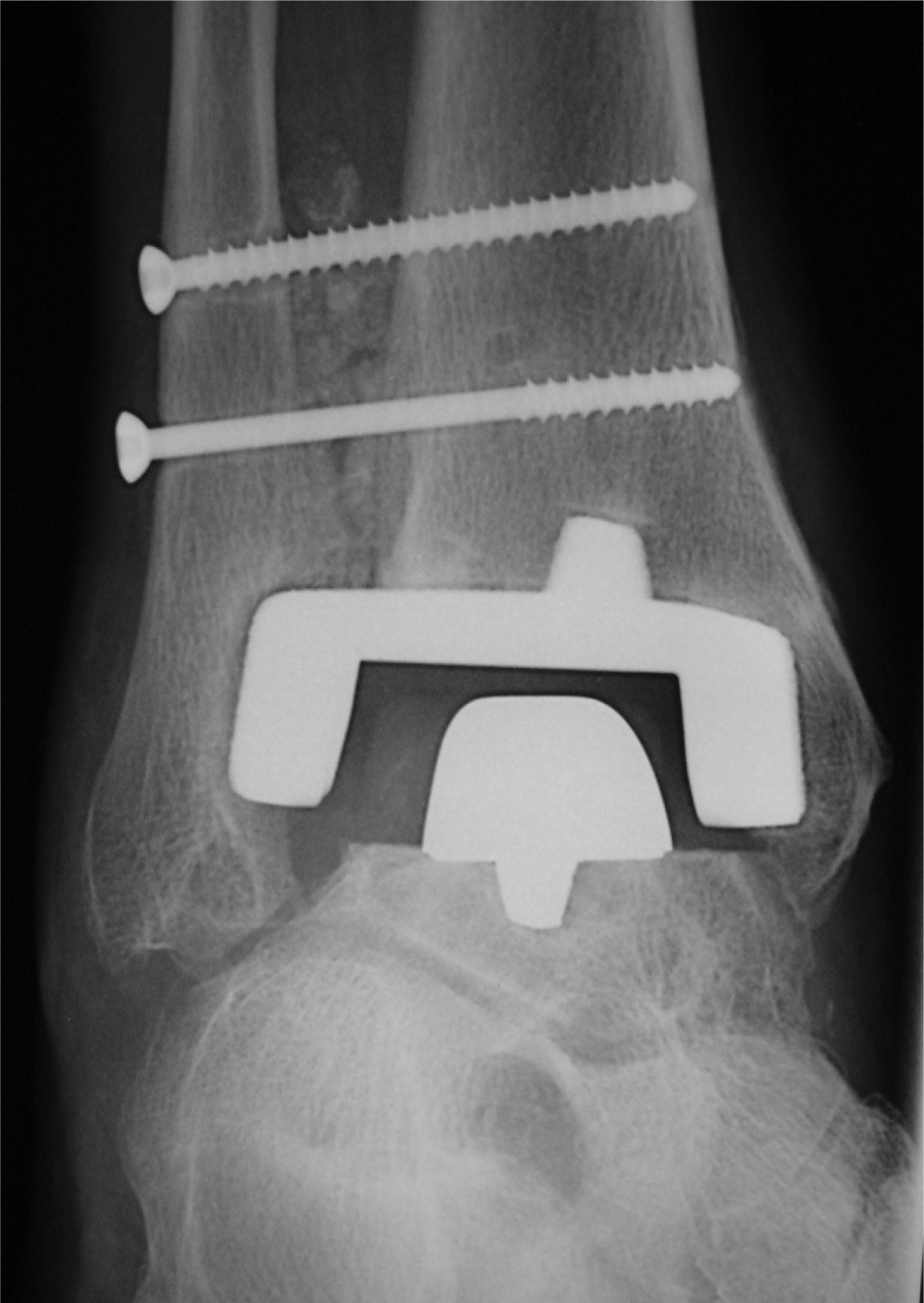
Probable nonunion.
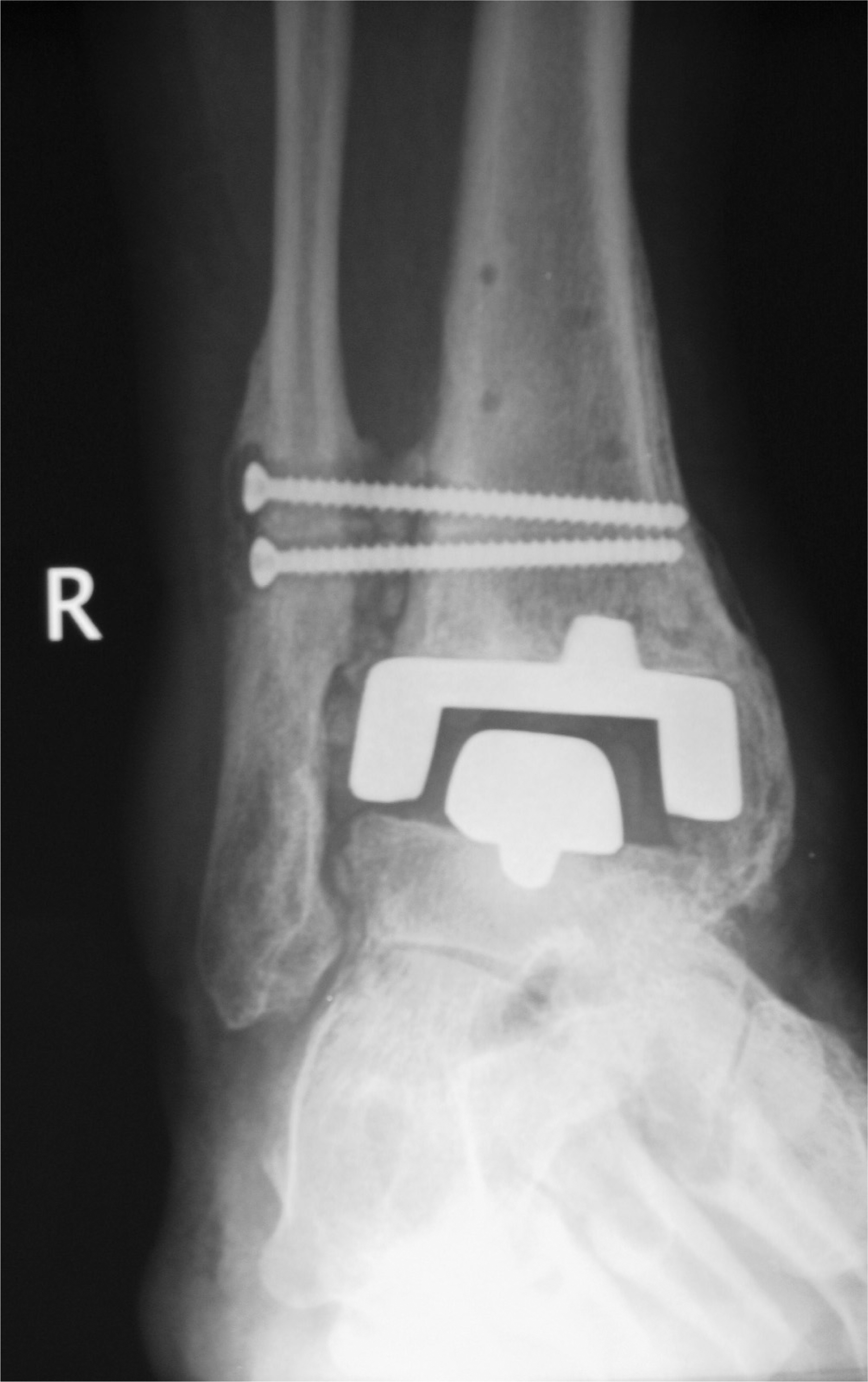
Syndesmosis nonunion.
DISCUSSION
The focus of this study was not to evaluate the outcome of ankle replacements but to evaluate the syndesmosis fusion rate with augmentation by autologous platelet concentrate.
Total ankle arthroplasty was first performed in the early 1970s, with overall discouraging results. These early procedures were aimed at avoiding the complications of ankle arthrodesis, such as nonunion, malunion, infection, soft-tissue slough, and nerve injury. 27,10 Because the loss of ankle motion is related to arthrosis throughout the foot, 19 and to an abnormal gait, 21 a successful total ankle arthroplasty would improve the function of the foot. Unfortunately, total ankle arthroplasty led to unacceptable long-term failure rates, and revision of the failed total ankle arthroplasty often ended in ankle arthrodesis, tibiotalocalcaneal arthrodesis, or below-knee amputation. 21,18 Therefore, many physicians abandoned total ankle arthroplasty as a viable treatment option. 4,6,16,19,30,39 From these early trials, however, valuable knowledge was obtained, which led to design improvements in second-generation ankle arthroplasty systems.
Syndesmosis fusion rate without (Group A) and with (Group B) autologous platele concentrate
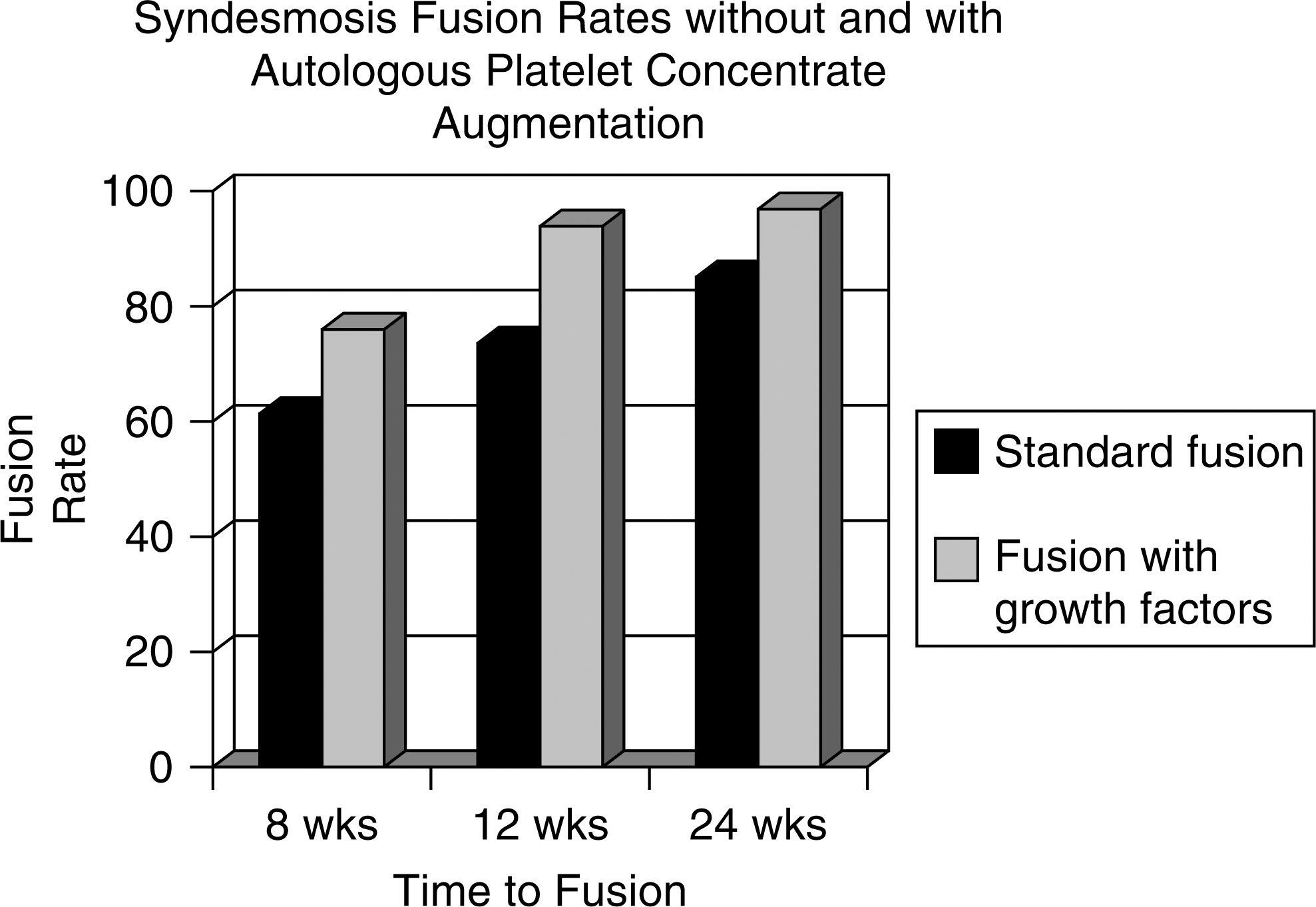
Syndesmosis fusion rates without and with autologous platelet concentrate.
During the mid to late 1980s, total ankle arthroplasty experienced a resurgence. Improved understanding of ankle biomechanics and the modes of total ankle arthroplasty failure led to developments in component design that are used today. 31,20 The ankle joint bears five to seven times body weight with each step over less surface area than in knee (three to four times) or hip (two to three times). 35,2,36 In addition to the increased amount of force at the ankle, the mechanism includes a shear force and a compressive force. 9 This creates problems with designing components that will fit into a smaller space and yet withstand greater forces than other prosthetic joints. Also, the area of greatest strength in the cancellous bone of the distal tibia is posteromedial. 15 Therefore, minimal bone resection and stable fixation must be assured to prevent the tibial component from migrating into the relatively weaker anterolateral tibial plafond.
One challenge with this system is the requirement for a solid syndesmotic fusion to prevent migration of the tibial component. To provide malleolar flanges that resurface the medial and lateral recesses, this prosthesis relies on distal tibiofibular arthrodesis. The tibial component has porous coating on three surfaces to increase the surface area for bone contact and to allow load sharing with the fibula. Successful fusion of the syndesmosis is important for the function of the prosthesis. 1 Two studies of the Agility total ankle arthroplasty include data regarding the delayed union or nonunion rates of the distal tibiofibular joint. 31,33 In the study by Pyevich et al. 31 delayed union occurred in 29% percent of total ankle arthroplasties and nonunion in 9%. They found a significant correlation between migration of the tibial component and delayed union or nonunion of the syndesmosis or syndesmotic arthrodesis. The reported risk ratio for migration of the tibial component in a patient with a distal tibiofibular joint nonunion compared to a solid fusion was 8.5. Also, the prevalence of ballooning lysis in ankles with delayed union or nonunion was significantly higher than with a solid fusion. In the study of Saltzman and Alvine, 33 the syndesmotic fusion nonunion rate for 180 patients with at least 6-month followup was 18%. 33 In this same study, the results from three different surgeon's first 10 Agility total ankle arthroplasties were reported. The delayed union rate of the syndesmosis was 38%. Therefore, in addition to other factors, surgeon experience appeared to be an important component of success. Finally, consistent with other results, survivorship of the implant was related to early solid fusion of the syndesmosis.
In a recent review of growth factor used to promote bone healing, Lieberman et al. 12 documented numerous preclinical and clinical studies supporting the use of these agents in treating orthopaedic injuries. 22 However, few studies document the clinical application of a combination of growth factors such as PDGF, TGF-β, IGFs, and FGF. The hallmark of the initial phase of bone healing involves inflammation. During this process a hematoma forms around the injured bone. Platelets in the hematoma degranulate, releasing growth factors, which act at different phases of bone healing. 3,4 At the site of bone injury, PDGF is present and is mitogenic for osteoblasts. 8 Transforming growth factor beta also is found early in fracture healing; however, there is evidence that it influences bone healing at all stages especially with respect to endochondral ossification. 15 Bone morphogenic protein is a member of the TGF-β super-family. 32 Insulin-like growth factor mediates the stimulatory effects of growth hormone on the skeleton, as well as working in concert with other growth factors to stimulate cell proliferation. 37 Osteoblast and chondroblast cellular processes such as mitogenesis and differentiation are regulated by FGF. 38
With regards to human clinical trials, Lowery et al. 25 reported no pseudarthosis on plain radiographs after augmenting posterior instrumented lumbar fusions with an autologous platelet concentrate, although this study was without controls. Of the smokers, 50% achieved fusion in the platelet rich concentrate group at 6 months compared to 20% in the group without platelet rich concentrate. In stark contrast to this, Weiner et al 41 reported the results of noninstrumented single-level posterior lumbar fusion augmented with autologous platelet concentrate. The fusion rate of the control group was 24 of 27, or 91%, compared to 18 of 32, or 62% in the autologous platelet concentrate group. They contributed the phenomenon to a possible antagonism between autologous growth factors and BMP. 28 Other possible mechanisms may include the concentration of platelets or techniques used to obtain the platelet concentrate. Other recent studies on spine fusion have failed to demonstrate either detrimental or beneficial effects from the use of autologous platelet concentrate. 13,23
Our present study demonstrated a statistically significant improvement in distal tibiofibular syndesmosis arthrodesis rate compared to our initial cohort. When a delayed union was defined as fusion after 6 months, our preliminary data showed a 94% arthrodesis rate in the autologous group compared to 73% in the control group. Some cite delayed union rates of 18% to 38% and nonunion rate of 9%. 33 This finding is noteworthy, because compelling evidence exists indicating that a distal tibiofibular syndesmosis nonunion is related to migration of the tibial component in the Agility total ankle arthroplasty. 31 The excellent short-term results in this series may be attributable to the use of autologous platelet concentrate.
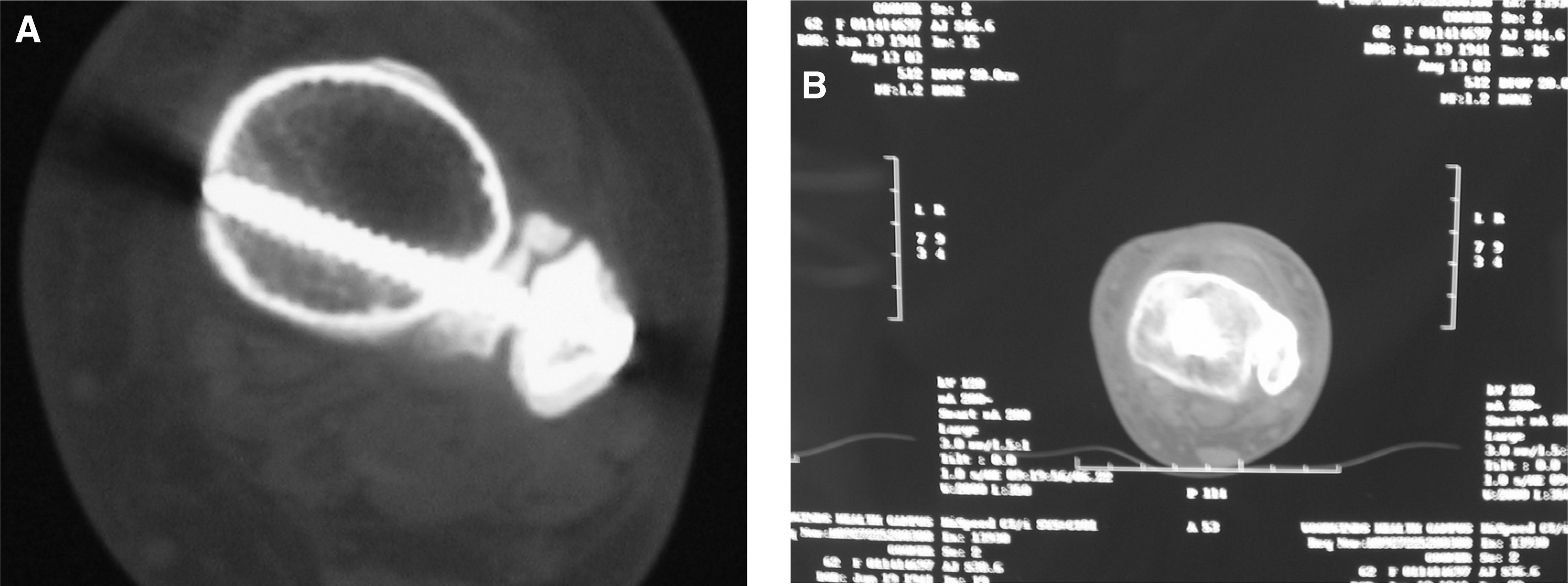
Several points of weakness of our study are the use of a nonrandomized historical control and the subjective use of radiographs as an endpoint for fusion. CT scans were obtained if union was questionable (Figure 3). Another confounding variable is the possible improvement in operative technique in the autologous concentrate group. However, a prognostic indicator of long-term success, syndesmosis union, has been improved. Long-term followup is needed to make a definitive determination concerning the effect of autologous platelet concentrate on the long-term function and survival of total ankle arthroplasty.