
Abstract
Background: With improvements in biomaterials and design, implant arthroplasty is becoming a useful option for treatment of disorders of the hallux. Methods: Forty-eight patients (53 implants) who had Bio-Action great toe implants (Osteomed, Addison, TX) for symptomatic advanced degenerative changes in the first metatarsophalangeal (MTP) joint have been followed prospectively since August of 1998. We reviewed the functional results of 32 patients (36 implants) at a minimum followup of 36 (range 36 to 69, mean 47) months. The scoring system designed by Kitaoka et al. was used to assess the functional results. Patient satisfaction, length of hospital stay, time to return to routine activities, footwear problems, radiographic appearances, and complications also were studied. Results: With the numbers available, there was significant improvement in the range of motion achieved and hallux MTP scale after the operation. There was a positive correlation (r = 0.87) between patient satisfaction and the hallux MTP scale. However, there was no correlation between patient age and patient satisfaction or hallux MTP scale. Seventy-seven percent of patients considered the result of the operation to be good or excellent. Conclusion: Overall, the 5-year functional results of this total joint system appeared to be satisfactory.
INTRODUCTION
The first metatarsophalangeal (MTP) joint frequently is the site of pain and deformity in adults. There is no consensus about the treatment of painful, advanced degenerative arthrosis involving the first MTP joint. 7,14 Keller resection arthroplasty is associated with unpredictable results and a high incidence of transfer metatarsalgia especially in active adults. 17,19 Arthrodesis is best reserved for patients who have an active lifestyle and engage in daily activities of high demand, such as heavy manual labor and sports. There have been few reports of the results after arthrodesis of the first MTP joint for the treatment of isolated hallux rigidus. Although these reports are helpful because they provide an indication of patient satisfaction, their usefulness is limited because of the multiple operative techniques that have been used, the subjectiveness of the criteria for reporting results, and the lack of statistical analyses. Prolonged periods of immobilization, malunion, nonunion, degenerative changes in adjacent joints, and footwear restrictions are some of the limitations associated with arthrodesis. 7,14 Other operative techniques described for severe hallux rigidus include capsular interposition arthroplasty 4 and carbon fiber arthroplasty 9 of the proximal phalanx.
Implant arthroplasty in disorders of the hallux is a useful alternative option. 3,10 Recent improvements in the biomaterials and understanding of biomechanics of the first MTP joint have revived the concept of total joint replacement. With the success of cobalt-chrome alloy and polyethylene in hip and knee arthroplasties, some systems for great toe replacement have been introduced. In MTP joint arthroplasty, these are designed as two-component, semi-constrained or nonconstrained articulations. The Bio-Action great toe implant (OsteoMed, Addison, Texas) (Figures 1 and 2) is an example of a nonconstrained, two-component total joint replacement system with a phalangeal component. It is made of titanium and a medical grade high-density polyethylene bearing surface articulating with the metatarsal component made of cobalt-chrome alloy. Theoretically, the engineering of this implant allows and enhances both normal contact pronation and toe-off supination, thus reducing stress on the first ray and enhancing forward ambulation in a more efficient manner. 2 The implant materials, titanium, cobalt-chrome, and ultra-high molecular weight polyethylene, have been proven to be both inert as well as durable over long periods of time. This new system is expected to give a good functional outcome, with lasting pain relief, a better cosmetic appearance than after arthrodesis or resection arthroplasty, and preservation of length and motion of the joint, and use of normal footwear.

Bio-Action great toe implant 24 months postoperatively.

Lateral radiograph 24 months postoperatively.
The available reports on early and intermediate results (up to 5 years) of the two-piece, nonconstrained total joint replacement systems of the hallux MTP joint are encouraging; 6,11 however, there are no prospective studies to our knowledge.
MATERIALS AND METHODS
Between August, 1998, and May, 2004, 53 total joint replacements were done in 48 patients. Those patients with severe degenerative changes in the first MTP joint who were otherwise candidates for either resection arthroplasty or arthrodesis were included in the study. The main indications included symptomatic hallux rigidus (Hattrup and Johnson grade III 14 ) refractory to conservative measures, symptomatic degeneration secondary to a long-standing hallux valgus, previous failed hallux surgery with painful degeneration and restriction of function and motion, and symptomatic degeneration of the first MTP joint after trauma or inflammatory or metabolic disorders. Patients with local or generalized sepsis, peripheral vascular disease, neurologic impairment, poor local skin condition, and poor medical conditions were excluded from the study. Patients who were unwilling to participate in the study also were excluded.
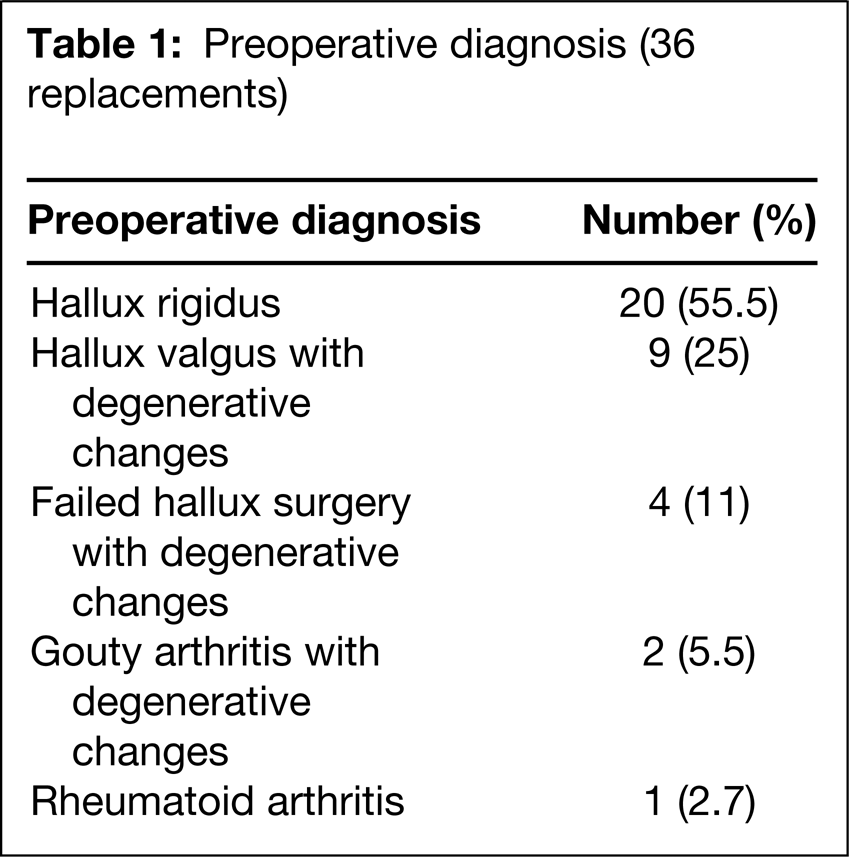
We reviewed the results of 32 patients (36 replacements including four bilateral) with a minimum followup of 36 months. Since the aim of this study was to evaluate the intermediate results, only patients with at least 36 months of followup were included in the analysis. The mean age was 57 (38 to 72) years and mean followup was 47 (36 to 69) months. There were 24 females and eight males. The preoperative diagnoses are shown in Table 1. Twenty-two of 32 patients (71.8%) were either housewives with activities of low demand or were in occupations such as clerical or managerial jobs.
Preoperative diagnosis (36 replacements)
The condition and all the treatment options available for this condition were discussed with the patients. Those patients who opted to have the total joint replacement using the Bio-Action great toe implant and were willing to participate in the study were informed about the limitations and possible complications of the procedure. All the patients who agreed to participate in the study were carefully assessed preoperatively and at regular intervals postoperatively. The principal symptoms, disabilities, range of movement, footwear problems, and any associated deformities were assessed preoperatively and postoperatively at each followup visit. Subjective assessment was done by using grades of satisfaction as excellent, good, fair, or poor. Assessment also was done by using the hallux MTP scale as described by Kitaoka et al. 5,13 Patients were evaluated at 2 weeks, 6 weeks, 3 months, 12 months, and annually thereafter unless otherwise indicated.
Operative Technique
A dorsomedial approach was used in all patients. The metatarsal cut was performed with a 10-degree dorsal slant to allow improved dorsiflexion. The phalangeal cut was made perpendicular to the long axis of the proximal phalanx. The correctly sized implants as determined at surgery were then inserted with an interference fit.
One 69-year-old patient needed a cemented implant on the metatarsal side because of a cyst in the metatarsal head. Additional procedures included basal osteotomy of first metatarsal using single screw fixation for severe hallux valgus deformity and severe degenerative changes in MTP joint (six of 53 replacements) (Figure 3) and correction of lesser toe deformities in six patients.

Additional basal osteotomy of first metatarsal 39 months postoperatively.
Patients were allowed to walk with wooden soled shoes as soon as they were comfortable. Physiotherapy was started 48 hours postoperatively to maintain the passive range of motion achieved at surgery.
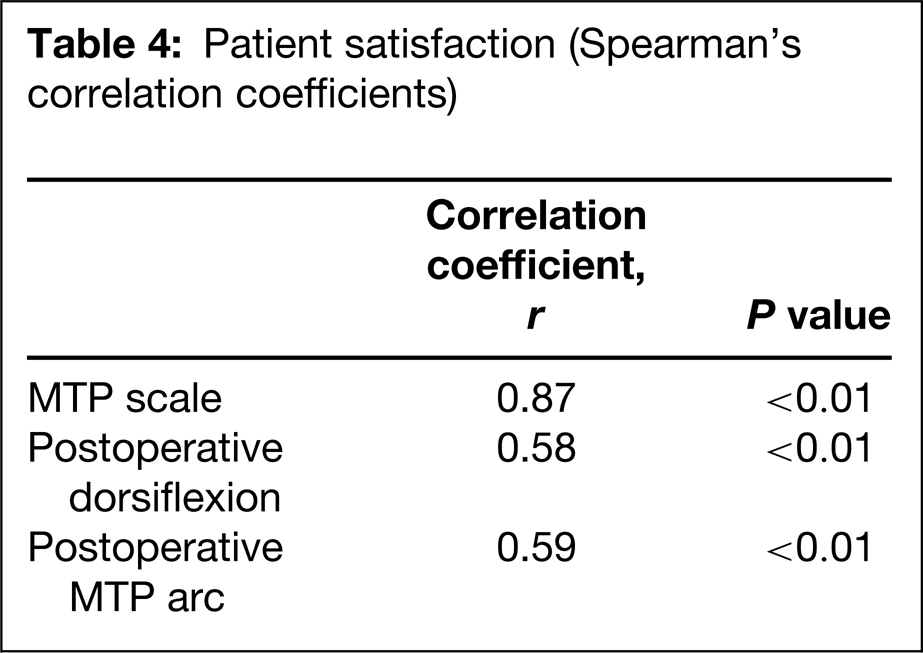
Statistical analyses are provided in Table 4.
RESULTS
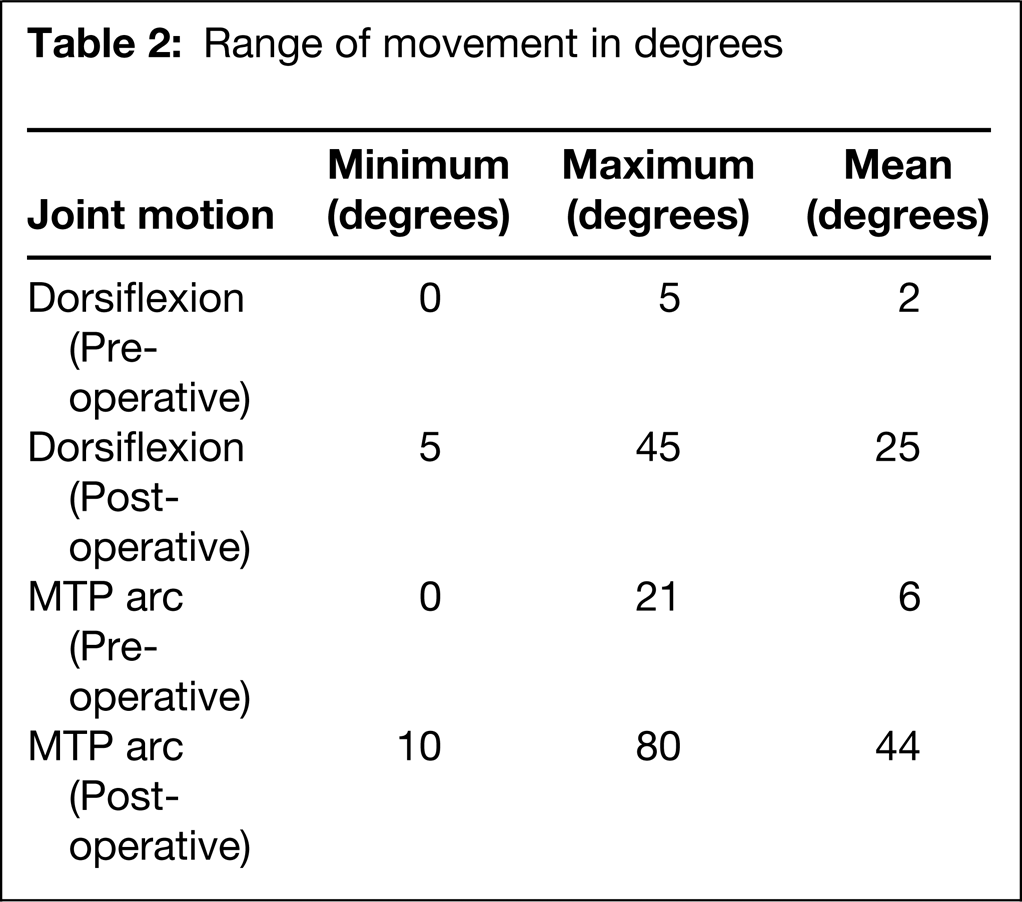
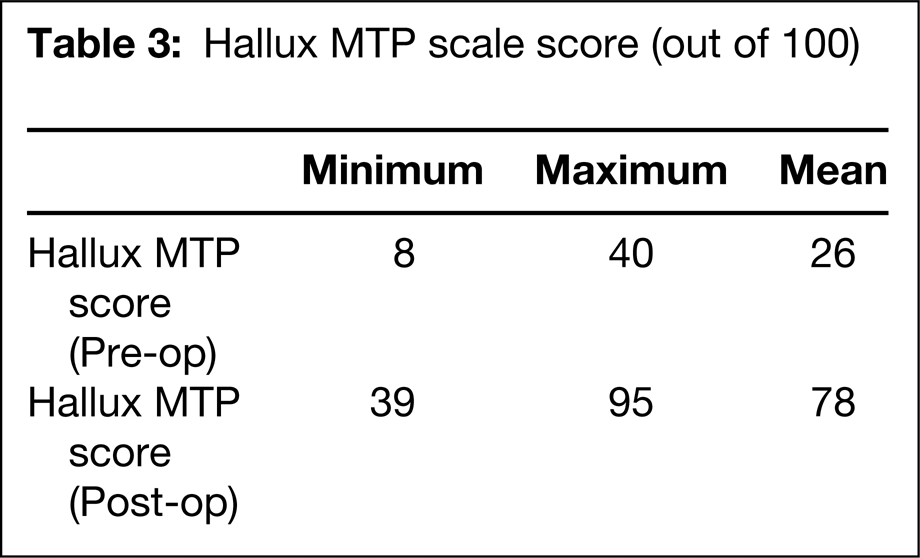
We reviewed the intermediate results of 32 patients (36 replacements) with a minimum followup of 36 months that included radiographic features. The mean length of stay in the hospital was 3 (1 to 5) days including the day before operation when the patients were admitted. The mean duration of followup was 47 (36 to 69) months. Twenty-two of 32 patients (69%) returned to normal daily activities or work between 4 and 6 weeks postoperatively. At the latest review, the average MTP joint arc of motion was 44 (10 to 80) degrees and the average hallux MTP scale was 78 (39 to 95) (Table 2 and 3). There was a significant improvement in dorsiflexion, MTP arc of motion and Hallux MTP scale after surgery (paired samples test p value <0.01).
Range of movement in degrees
Hallux MTP scale score (out of 100)
At the latest followup, there was significant improvement in the degree of pain, functional abilities, and footwear requirements as compared to preoperative status. Twenty-five of 32 patients (79%) returned to normal or an occasionally affected lifestyle after the operation. Twenty-six of 32 of patients (81%) wore conventional footwear, and three of 32 patients (9%) wore footwear with inserts.
Patient satisfaction (Spearman's correlation coefficients)
No patient had significant transfer metatarsalgia. Twenty-eight of 32 patients (88%) had improvement in function. Three patients who continued to have pain after the operation rated the result as poor. Two of the three patients who had poor outcome had revision surgery. One patient had removal of the implant and excision arthroplasty, and the other patient had arthrodesis of the joint 30 months after the primary replacement. There was no obvious cause to explain the poor results in all the three cases. Our overall revision rate of the procedure to date is 5.5% with a minimal followup of 36 months (two of the total 36 replacements). The radiographic studies to date have revealed no evidence of dislocation, osseous encroachment around the implant, changes at the hallux interphalangeal joint, implant break down, or stress fracture of the metatarsals (Figures 1 and 2). Periprosthetic lucent lines predominantly in the metatarsal component probably were caused by loosening and change of implant position, and subsidence of the implant were observed in 12 of 36 implants at a minimum of 36 months followup. But this did not compromise the functional outcome, and subjective satisfaction of patients remained high (Figure 3). With the numbers available, no significant difference could be detected in the functional outcome between males and females. Similarly, patients with activities of low demand did as well as patients with activities of high demand. However, the numbers are too low to make any significant comparisons.
We had one intraoperative complication of fracture of the first metatarsal while inserting the implant. This was treated by cerclage wiring. No patient had any significant infections of the implant.
The subjective satisfaction in 32 patients (36 replacements) at a minimum followup of 36 months was excellent in 36% (13 of 36), good in 41.6% (15 of 36), fair in 13.9% (five of 36), and poor in 8.3% (three of 36). The objective assessment of improved functional abilities and joint range of motion correlated (r = 0.52) to the subjective satisfaction expressed by the patients.
DISCUSSION
Papagelopoulos et al 12 reported their experience with 93 primary implants (79 patients) of the first MTP joint using cemented metal and polyethylene components and silicone implants. The mean age of their patients was 56 (19 to 75) years. The average duration of followup evaluation in 75 patients who were alive and without reoperation was 12 (2 to 17) years. At 10 years, implant survival was 82% in patients 57 years of age or younger, and 90% in patients older than 57 years. The authors concluded that the overall probability that an implant would be in situ was 82% at 15 years after arthroplasty. Survivorship was higher in patients who were older than 58 years. They also reported that the implant survival was not significantly affected by preoperative diagnosis, gender, relative weight, previous operation, or type of implant.
Townley and Taranow 16 reported 279 arthritic hallux MTP joints treated with metallic resurfacing hemiarthroplasty over a 40-year period. The implant was designed to replace only the articular surface of the proximal phalanx, with minimal resection of bone stock. Ninety-five percent of patients had a good or excellent result at a followup of 8 months to 33 years.
Koenig and Horwitz 6 reported a 5-year study of 61 total joint arthroplasties using the Biomet total toe system. Of the 61 cases, 49 had a diagnosis of hallux rigidus and 12 had a diagnosis of hallux valgus. Ten involved revision of failed silastic elastomer implant arthroplasty. The patients' age ranged from 29 to 72 (mean of 54.5) years. All patients had end-stage arthroses. They reported overall excellent results (51 of 61) with 10 having various levels of compromised results.
Olms and Dietze 11 reported 21 patients who had arthroplasty using the Bio-Action toe implant with a 2-year followup. Seventeen of the 21 patients recorded less pain or no pain after the operation and increased range of dorsiflexion. An equal number of the patients recorded increased activity levels after the operation. A good cosmetic result was reported in all patients, and there were no revisions or infections.
The main problems associated with implant arthroplasty of the MTP joint today is a lack of standard outcome measures, incremental design changes, and limited reports on long-term followup. There are currently at least five different two-component implant systems for replacement of the first MTP joint. 1 The Acumed Great Toe System, (Acumed, Beaverton, OR) the Biomet total toe system, (Biomet Inc, Warsaw, IN) Bio-Action great toe implant (Osteomed Corp, Addison, Texas), the Kinetik great toe implant (Kinetikos Medical, Inc. San Diego, CA), the Reflexion first metatarsophalangeal joint implant (Osteomed Corp, Addison, Texas).
Our study is probably one of the largest prospective case series with a minimum 3-year followup using a two-component, nonconstrained metal and polyethylene total joint replacement for hallux MTP joint arthritis. Although Townley and Taranow 16 reported 96% excellent or good results using hemiarthroplasty in degenerative joints with problems on both sides of the joint, it is more logical to replace the total joint with a two-component, nonconstrained system.
The subjective satisfaction in our series of 32 patients (36 replacements) with a minimum followup of 36 months was excellent in 36% (13 of 36) and good in 41.6% (15 of 36). Improvement was noted in the arc of motion and dorsiflexion of the MTP joint (paired samples test significant at 5% level) and in the degree of pain, functional abilities, and footwear requirements after the operation. The objective assessment of improved functional abilities and joint range of motion correlated to the subjective satisfaction expressed by the patients. We found no correlation between the age of patient and patient satisfaction or hallux MTP scale.
The intermediate (3 to 5 years with average followup of 4 years) functional results of this two-component, nonconstrained total joint replacement system using the Bio-Action great toe implant for painful, advanced degenerative arthritis were satisfactory. Careful preoperative assessment, meticulous operative technique, and regular followup are mandatory for successful outcome. The study is ongoing and we are still recruiting patients and will look at 10-year results. Because of the high biomechanical demands placed on the first MTP joint and the complex interactions between the joints of the foot, routine use of joint replacement arthroplasty cannot be recommended until good results have been achieved consistently over time from large multicenter trials. Careful explanation to the patients of all other options of treatment including arthrodesis and resection arthroplasty is very important. There are many centers in Europe and North America, using some form of total joint replacement systems for the hallux MTP joint replacement with different outcome measures. We emphasize a need for a universal scoring system in assessing these patients and a large, multicenter prospective trial to further prove the usefulness of a total joint system of this kind.