
Abstract

INTRODUCTION
Syndesmotic instability of the tibiofibular ligaments can be difficult to diagnose clinically. This clinical tip reports a diagnostic sign of late medial ankle pain as a possible indicator of syndesmotic laxity. The pain is caused by tenderness of the deltoid ligament as it attenuates because of lack of other syndesmotic restraints in the ankle. This clinical sign suggests an incremental, slowly progressive shift of the talus and subtle widening of the ankle mortise. Awareness of this possibility may help to diagnose a complex ankle injury. Although biomechanical studies have implicated the deltoid ligament as an important stabilizer of the ankle and a restraint to syndesmotic widening, recognizing an initially intact deltoid ligament that may progressively stretch and allow gradual clear space widening is not documented. 1 , 2 Duration of symptoms should be considered when diagnosing ankle pain because damage to restraining structures can lead to further injury.
The temporal element in ankle instability helps to explain the later clinical findings. A lax or incompetent syndesmotic ligament complex will allow progressive widening of the ankle mortise with a lateral shift of the fibula. The primary resisting force of this widening is the deltoid ligament. In the early phase of medial clear space widening, the deltoid begins to be stretched. This stretching process is often painful and can be observed by the physician on clinical examination both as tenderness along the deltoid ligament itself and as tenderness with external rotation of the ankle. The process may be prolonged and may take place over months or even years as the restraining ligaments of the foot are strained. Ultimately the deltoid becomes incompetent, and the sequelae of an ankle joint unevenly aligned in the mortise become clinically obvious with ankle joint synovitis and pain. 3 Thus, an occult syndesmotic ligament injury may lead to persistent medial ankle pain.
A recent biomechanical study 1 of stress in the syndesmotic ligaments with provocative stretch testing of the syndesmosis revealed little displacement in the actual ligaments and recommended elicited pain as the best outcome measure of such tests. The current clinical tip suggests that the clinical finding of medial ankle pain represents the transition to syndesmotic instability and supports the biomechanical findings. 1 The clinician should be aware that medial ankle pain might be a manifestation of syndesmotic dysfunction and subsequent straining of the deltoid. Earlier recognition of this problem may decrease the morbidity of the injury and may help minimize the risk of arthritis.
CLINICAL TIP
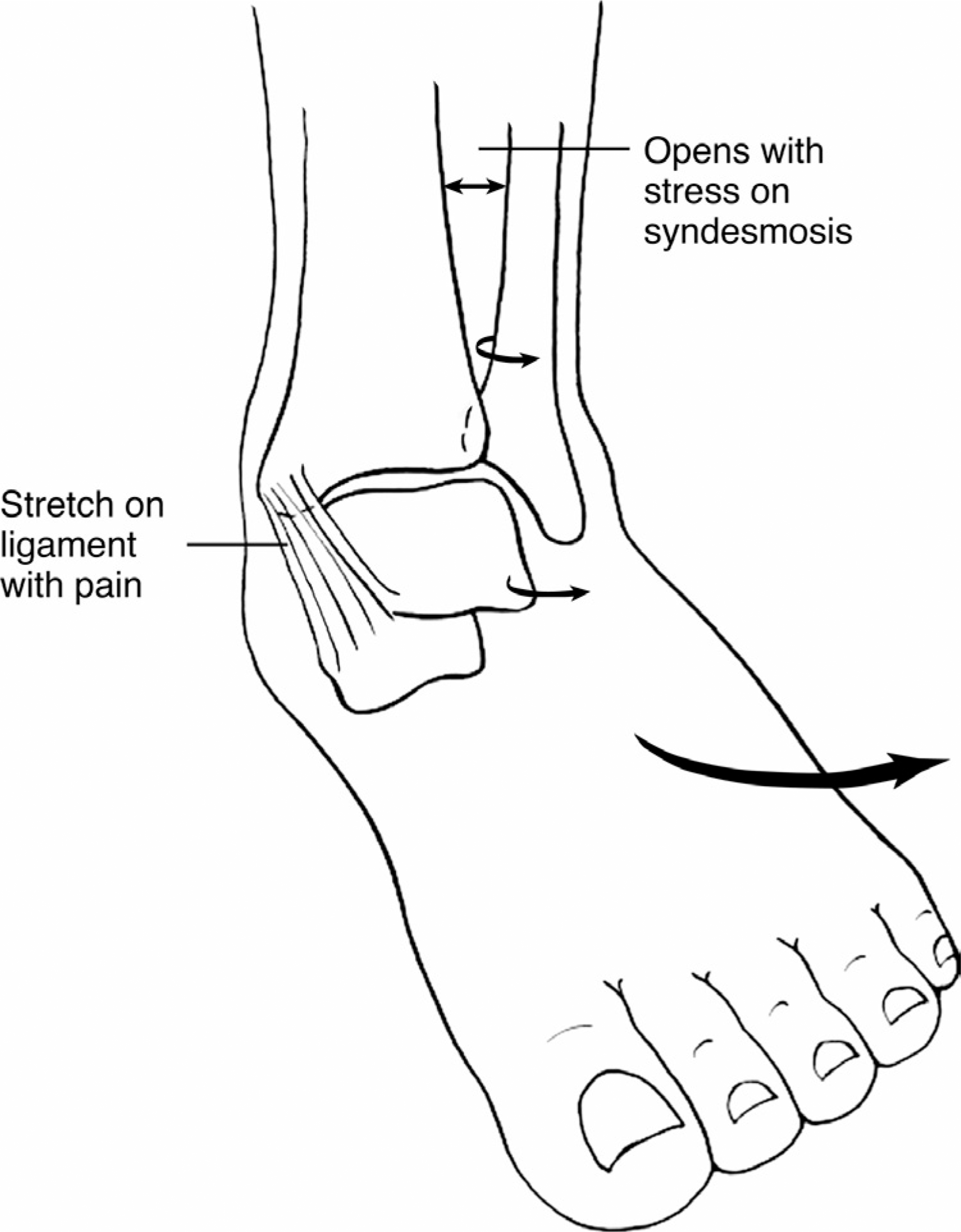
Clinical examination for ankle mortise instability after rotational injury may reveal tenderness at the distal tibio-fibular syndesmosis with strain of the syndesmotic ligaments, especially with external rotation of the foot against the leg with the knee bent (Figure 1). Pain in the medial aspect of the ankle is one manifestation of syndesmotic injury. Initially, the structural integrity of the various components of the deltoid ligament is maintained and there is no medial joint space widening that would indicate instability (Figure 2). Later, the medial pain decreases as the deltoid is attenuated or ruptured and the only remaining pain is in the ankle joint and the syndesmosis. The patient history also may include a vague deep leg pain that worsens with activity.
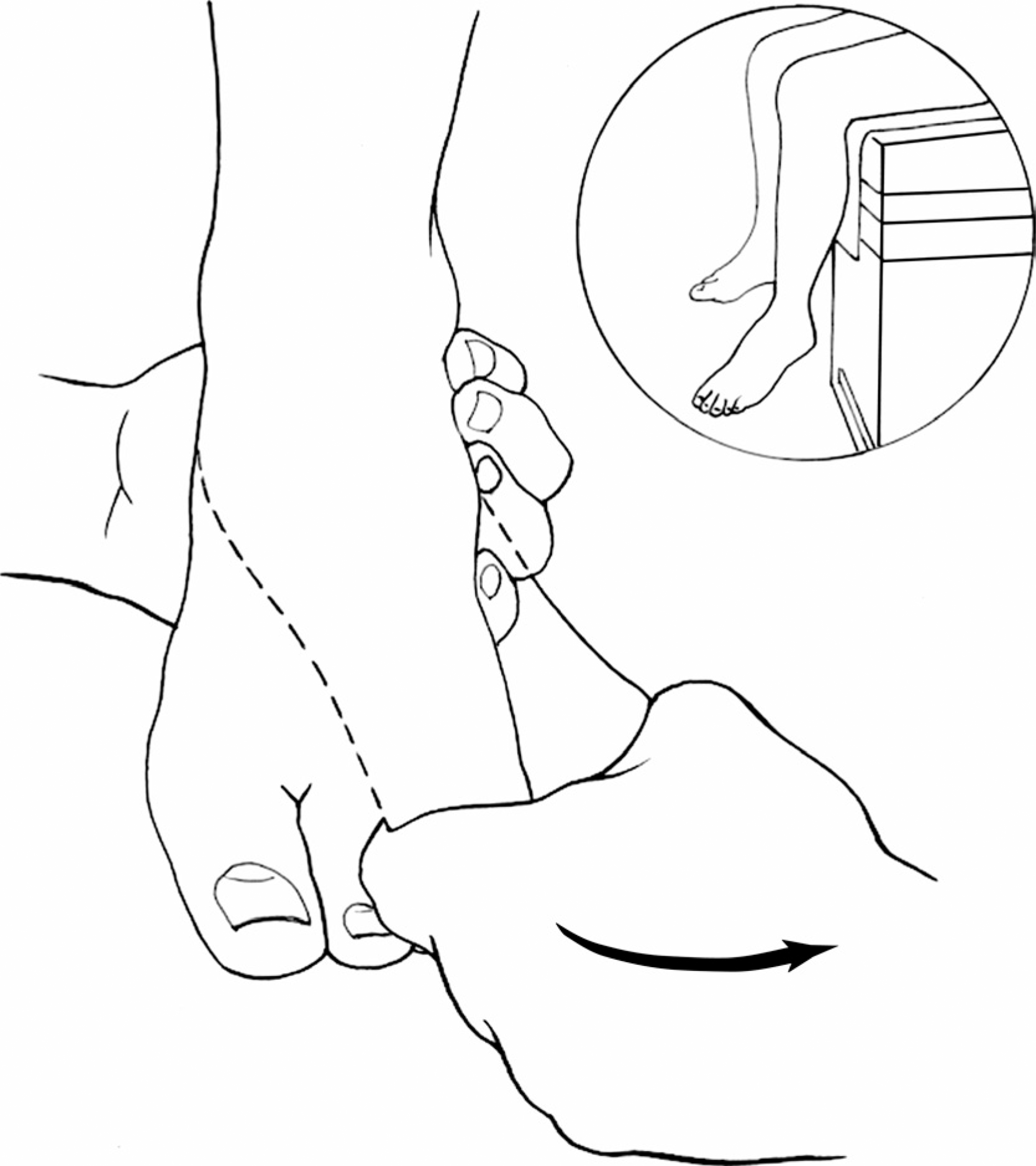
External rotation of the ankle with the knee bent. The examiner rotates the foot while holding the forefoot and the heel. The leg is externally rotated through the ankle joint.
External rotation places strain on the deltoid ligament, which is painful before stretching out or rupturing. This pain is medial and is a clue to subtle ligamentous instability at the syndesmosis.