
Abstract
Background:
Biomechanical studies on retrograde intramedullary fixation for tibiotalocalcaneal fusion have been reported, but no studies have investigated dorsiflexion stiffness, load-to-failure, fatigue endurance, and plastic deformation using different distal screw orientations. Also, no studies have examined the effect of bone density on different distal screw orientations while using a fatigue loading mode.
Methods:
Eight matched pairs of cadaver legs were used. In one leg from each pair an intramedullary nail was inserted with lateral-to-medial distal screws and in the other with posterior-to-anterior screws. These samples underwent dorsiflexion fatigue testing with determination of initial and final stiffness, load-to-failure, and degree of plastic deformation at failure. DEXA scanning was done of each cadaver specimen to determine bone mineral density. Statistical analysis was performed using the Student t-test and a Pearson correlation. Significance level was set at p < 0.05.
Results:
The specimens with posterior-to-anterior screws had a significantly higher fatigue endurance load-to-failure (1130.0 ± 362.0 N compared to 801.0 ± 227 N, p = 0.01). They also had significantly higher final stiffness (203.1 ± 23.1 N/mm compared to 146.6 ± 46.2 N/mm, p = 0.05) and lower plastic deformation (2.4 ± 1.5 mm compared to 3.8 ± 2.3 mm, p = 0.04). There was a statistically significant correlation between bone mineral density and the difference in construct deformation with posterior-to-anterior and lateral-to-medial screw orientation (r = 0.76, p = 0.03).
Conclusions:
In this biomechanical investigation of tibiotalocalcaneal arthrodesis with intramedullary nail fixation, posterior-to-anterior distal screw orientation provided more stable fixation than lateral-to-medial screw orientation.
Keywords
INTRODUCTION
Tibiotalocalcaneal (TTC) arthrodeses are used in patients with both ankle and subtalar joint diseases such as posttraumatic arthritis, idiopathic osteoarthritis, rheumatoid arthritis, Charcot arthropathy, and talar osteonecrosis. 5,19,20,22 The procedure often is effective, but concerns remain about inadequate fixation or loss of fixation, implant failure, malunion, nonunion, delayed union, and infection. 5 Reported nonunion rates in TTC fusion have ranged from 11% to 40%. 6 In addition, patients who have this procedure may have osteopenia secondary to disuse or inflammatory arthropathy, which can further jeopardize fixation stability. 8,12,16 Patients who have TTC arthrodesis often are unable to be immobile or control weightbearing, and poor bone stock also may be an issue. Stability of fixation is important in this patient group for these reasons.
Several techniques have been used to achieve stable fixation of tibiotalocalcaneal arthrodesis, including blade-plate, 2 screw, 3 bone grafting, 8 and intramedullary rod fixation. 10,21 Intramedullary (IM) rod fixation is a reproducible technique that provides the benefit of a load-sharing device and the potential for less soft-tissue damage. Several methods of IM rod fixation have been investigated. 7,13 A recent study of retrograde IM nailing for TTC fusion and posterior-to-anterior distal screw alignment achieved a 100% union rate, with a single malunion healing after corrective osteotomy. 11 Some surgeons also have suggested empirically 6,11,20 that posterior-to-anterior placement of the distal interlocking screws may be especially useful in patients with osteopenic bone, where achieving stable internal fixation is especially difficult. 6 In a biomechanical study, testing monotonic static load-to-failure with external rotation, posterior-to-anterior distal screw orientation for IM rod fixation was significantly stiffer than transverse distal screw placement. 13
Our hypothesis was that posterior-to-anterior placement of the distal screws with IM fixation provides better initial fixation and fatigue endurance than the more traditionally placed transverse lateral-to-medial screws. The objectives were to compare these two screw orientations under dorsiflexion loading in terms of initial and final stiffness, strength, and fatigue endurance in dorsiflexion with cadaver models. We also examined the effect of bone mineral density as determined by DEXA scan on the fixation achieved with the two different distal screw placements in cadaver specimens.
MATERIALS AND METHODS
Eight matched pairs of fresh-frozen cadaver legs (both legs from eight donors) were used for the fatigue evaluation. The specimens had no evidence of previous surgery or musculoskeletal disease. The average age was 70.5 years (range 62 to 77 years). Five pairs were from female donors and three were from males. The specimens were frozen no more than 4 weeks.
The cadaver samples were disarticulated at the knee and stored at —20°C. At the time of preparation, each specimen was rapidly thawed in a warm water bath and stripped of soft tissues. Amputation was carried out distally through the transverse tarsal joint and proximally through the tibial shaft 10 cm distal to the tibial tubercle. The entire fibula was removed from the specimen. The major ligamentous and soft-tissue supports about the medial and posterior ankle and the subtalar joints were initially left intact to aid in instrumentation but were removed after instrumentation. The articular surfaces were left intact.
The cadaver models were prepared with the following alignment: 1) tibiotalar joint in neutral dorsiflexion, 2) subtalar joint in 4 degrees of tibiotalocalcaneal valgus, and 3) calcaneus centered below the talus and tibia. This position was held temporarily with smooth 2.0-mm Kirschner wires driven from the medial calcaneus into the medial talus and medial malleolus of the tibia and placed to avoid interfering with subsequent fixation and screw placement. The reaming guide wire was then inserted from the plantar surface of the calcaneus into the talus and into the tibial shaft. The starting point of the rod was just lateral to the plantar medial ridge that extends from the medial tubercle to the anterior tubercle of the plantar calcaneus in the frontal plane and in line with the sustentaculum in the sagittal plane.
From the starting point on the plantar calcaneus, the guide wire was directed toward the intramedullary canal of the tibial shaft in both the anteroposterior and lateral planes. Flexible reamers were then used to ream the calcaneus, talus, and tibia in 0.5 mm increments to a 12.5-mm diameter canal to prepare for insertion of the IM rod (12 × 150 mm; DePuy/Ace, Warsaw, IN) (Figure 1). The rod was inserted using the alignment guide provided by the manufacturer, which facilitates the proper alignment of the distal and proximal locking screws. Care was taken to ensure that the rod position was not excessively prominent plantarly so that it would not interfere with the weightbearing surface of the calcaneus. Also, appropriate rod positioning provided for good distal screw location such that lateral-to-medial screws could be placed along the transverse axis of the sustentaculum tali and posterior-to-anterior screws could be placed along the long axis of the talus.
One side of each matched pair was randomly assigned to receive instrumentation with three distal interlocking 5.5-mm cortical screws placed in a lateral-to-medial direction in the talus and calcaneus. One screw was placed in the talar body and two were placed in the calcaneal body. The proximal calcaneal screw was directed toward the sustentaculum tali. The contralateral specimen was then instrumented with the distal 5.5-mm screws in a posterior-to-anterior orientation. One screw was placed in the talar body, and two screws were placed in the calcaneus. The long axis of the posterior-to-anterior distal screw placement was aligned with the long axis of the talus with the screw directed toward the center of the talar head. This screw position is approximately 15 degrees medially off the longitudinal axis of the foot, in the transverse plane, in accordance with manufacturer's guidelines. Once the talar screw position was determined, the placement of the two calcaneal screws was determined as directed by the alignment guide toward the anteromedial calcaneus. The proximal calcaneal screw was directed towards the dense bone just anterior to the sustentaculum tali. After distal screw fixation, axial compression was applied with an external axial compression device (DePuy, Warsaw, IN), and standard proximal medial-to-lateral tibial shaft screw fixation was carried out with two 4.5-mm cortical screws.
The calcaneus of each specimen was secured in a wooden box using four 2.0-mm Kirschner wires. The specimens were aligned within the box to ensure that impingement would not occur between the specimen and the wooden box during load testing. A polyester resin was then poured into the wooden box to surround and fix the calcaneus within the box. Care was taken to avoid any bridging of resin between the talus and calcaneus or between the talus and box apparatus.
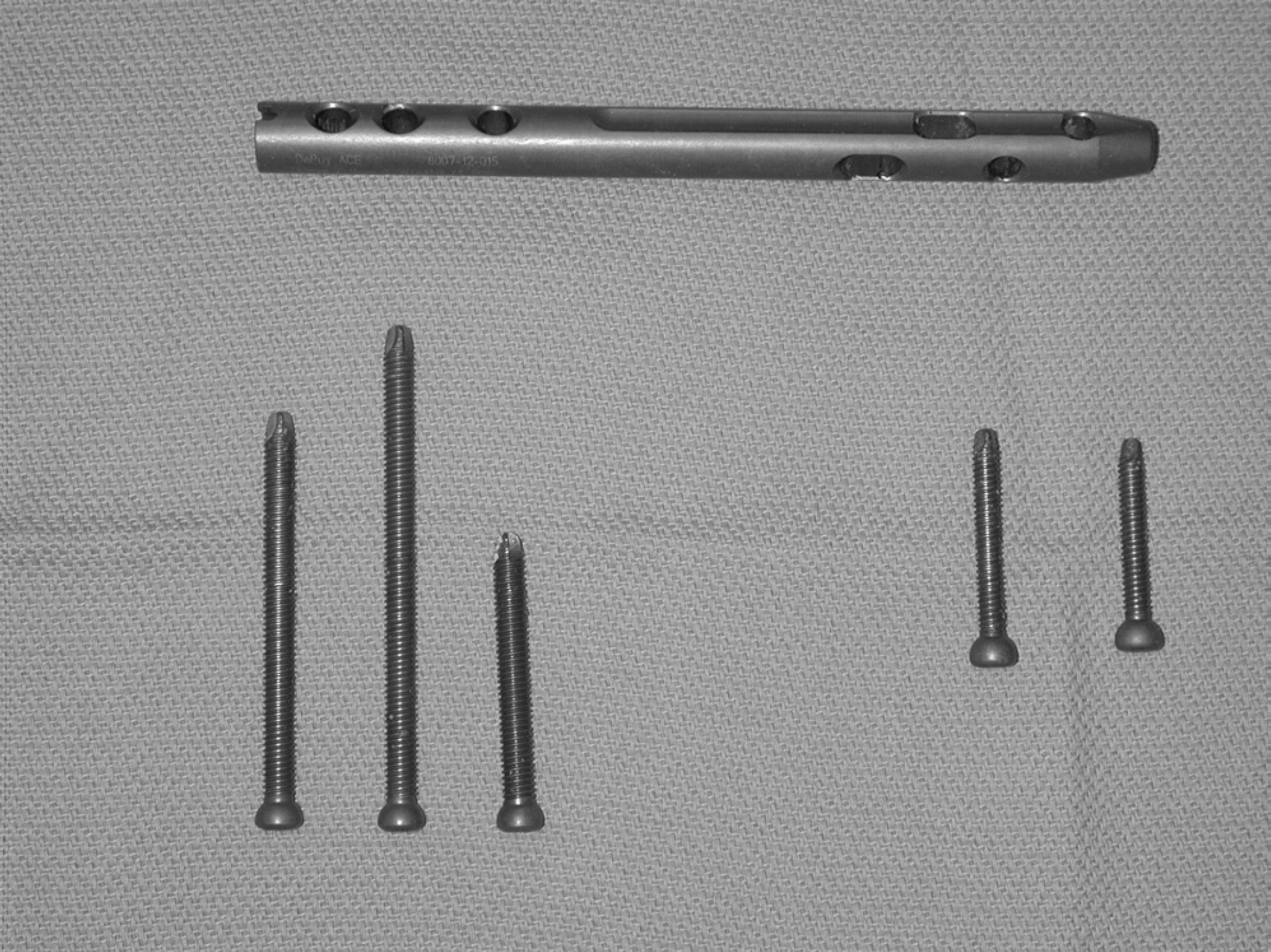
Intramedullary nails and interlocking screws used (DePuy/Ace, Warsaw, IN). Two pairs of proximal holes allow placement of the proximal screws in a medial-to-lateral direction, and the distal holes allow either lateral-to-medial or posterior-to-anterior screw placement. The proximal end of the nail and the proximal screws are shown at right.
Each specimen was mounted separately in the servohy-draulic load frame for dorsiflexion loading (MTS Systems, Eden Prairie, MN) (Figures 2 and 3). The load cell capacity of the MTS was 2500 N. The resolution of the test frame is 0.1% of the full scale value, and thus accurate measurement was possible to 2.5 N. Dorsiflexion loading was restricted to rotation about a pivot point 82.5 mm distal to the midline of the tibia in the anteroposterior direction to simulate a toe-off position, such as in normal postoperative partial weightbearing gait. Peak moment of 21.5 Nm was due to peak force of 260 N. We limited the fatigue motion to only dorsiflexion because we believe this is a worst-case loading configuration due to the relatively large moment arms of the forefoot. A previous study suggested most malunions or nonunions in TTC fusion occur in the sagittal plane, 19 a further reason for performing the fatigue tests with dorsiflexion loading. We chose only one direction of the dorsiflexion-plantarflexion movements in accordance with previous data indicating that there is no large difference between dorsiflexion and plan-tarflexion failure loads after tibiotalocalcaneal arthrodesis. 3 Further, in postoperative partial weightbearing heel-to-toe gait, the dorsiflexion stresses were believed to be most relevant contributor to failure. Although muscle forces may apply additional stresses through the fusion site, the authors believed this was not a major contributor to postoperative failure because the muscles in the limb are mostly inactive during the recovery period. The moment arm was calculated as the distance between a midline in the distal tibia in the anteroposterior direction and a perpendicular dropped to a bearing that was positioned in a medial-lateral direction (Figure 3).
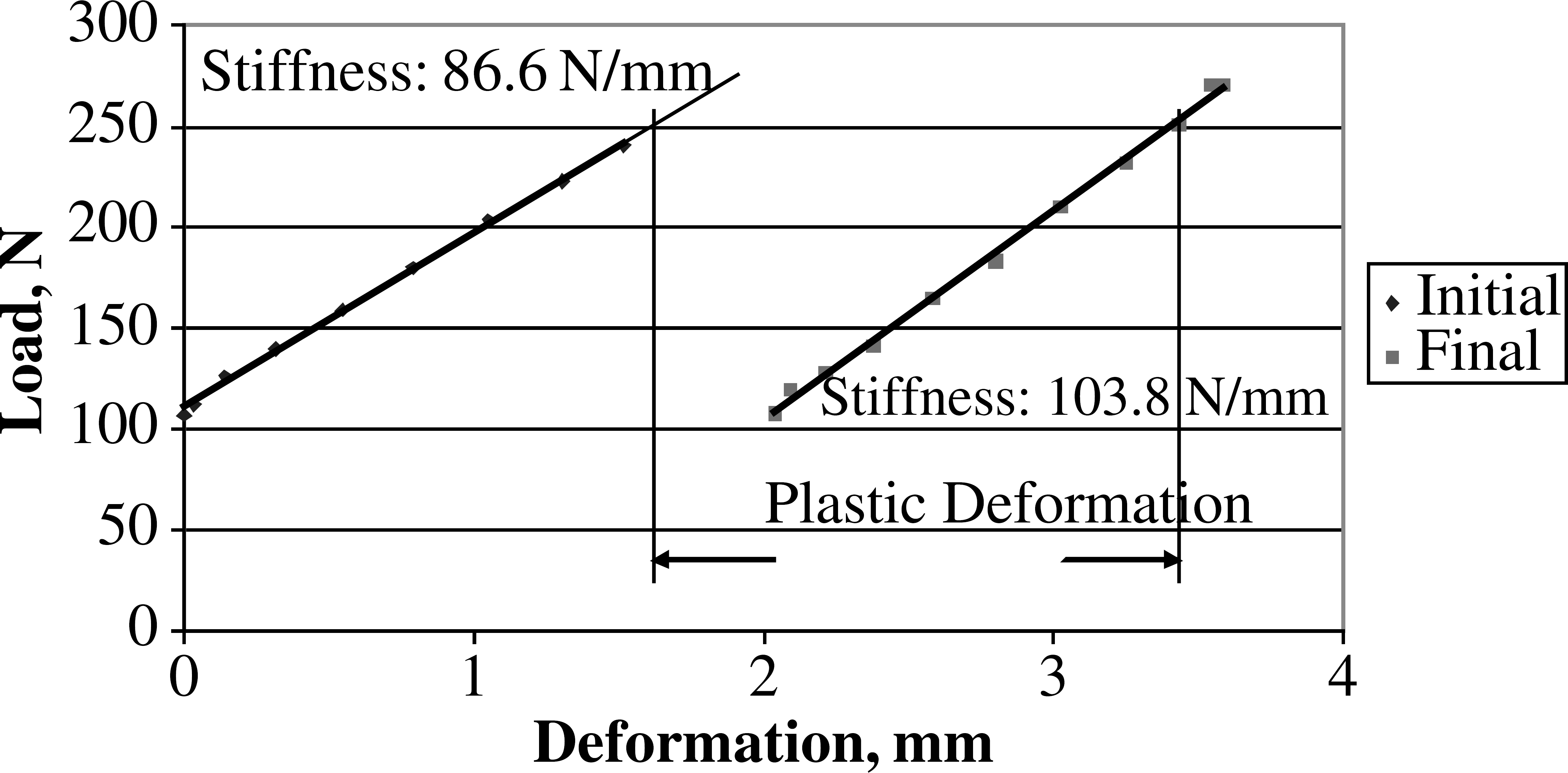
The eight matched pairs of cadaver legs (16 total specimens) were cyclically loaded in dorsiflexion to a maximum of 260 N at a rate of 3 Hz for 250,000 cycles. These values were chosen to simulate fatigue loads in a patient bearing partial weight heel to toe in postoperative crutch-facilitated gait for a 6-week period. Specimens were cyclically loaded until completion of 250,000 cycles or failure. Failure was defined as 10 degrees of dorsiflexion calculated using trigonometric functions and the actual axial displacement of the sample or fracture with catastrophic failure. The amount of dorsiflexion representing failure was somewhat arbitrary but was chosen to reflect gross failure that would not be expected to heal clinically. Load and deflection data were recorded during the initial load cycle and subsequently every 2,000 cycles. Initial fixation was calculated from the initial load data. At the end of 250,000 cycles, a final load deflection curve was generated with the specimen being taken from the original position to failure of 10 degrees of dorsiflexion or fracture. A measure of effective deformation was recorded for each specimen. The amount of effective deformation at a load of 250 N was defined as the difference between axial displacement at the beginning of the fatigue test and the end of the fatigue test.

Test set-up. The load frame was used for dorsiflexion loading.
The bone mineral density of the posterior calcaneus of each cadaver specimen was determined by dual energy x-ray absorptiometry (DEXA) using a QDW-1000/W Scanner (Hologic, Bedford, MA).
Statistical Analysis
The initial and final stiffness values and the final failure load were calculated and compared. A Student two-tailed paired t-test was used to determine whether differences in stiffness values or failure loads between the two different screw placement directions were significant. The correlation between bone mineral density and the difference in construct deformation with posterior-to-anterior and lateral-to-medial screw orientation was determined by the Pearson correlation coefficient. Statistical significance was set to a p-value 0.05 or less.
RESULTS
Placing screws in a posterior-to-anterior direction provided significantly higher final stiffness values (203.1 ± 23.1 N/mm versus 146.6 ± 46.2 N/mm, p = 0.05) (Figure 4) and static failure after cyclic loading values (1130.0 ± 362.0 N compared to 801.0 ± 227 N, p = 0.01) when compared with lateral-to-medial screw placement during cyclic fatigue testing. The final effective deformation was also significantly lower with the posterior-to-anterior placed screws (2.4 ± 1.5 mm compared to 3.8 ± 2.3 mm, p = 0.04) (Figure 5). No significant difference in initial dorsiflexion stiffness was observed between the specimens with posterior-to-anterior (123.8 ± 47.2 N/mm) and lateral-to-medial (107.0 ± 42.2 N/mm) screws.
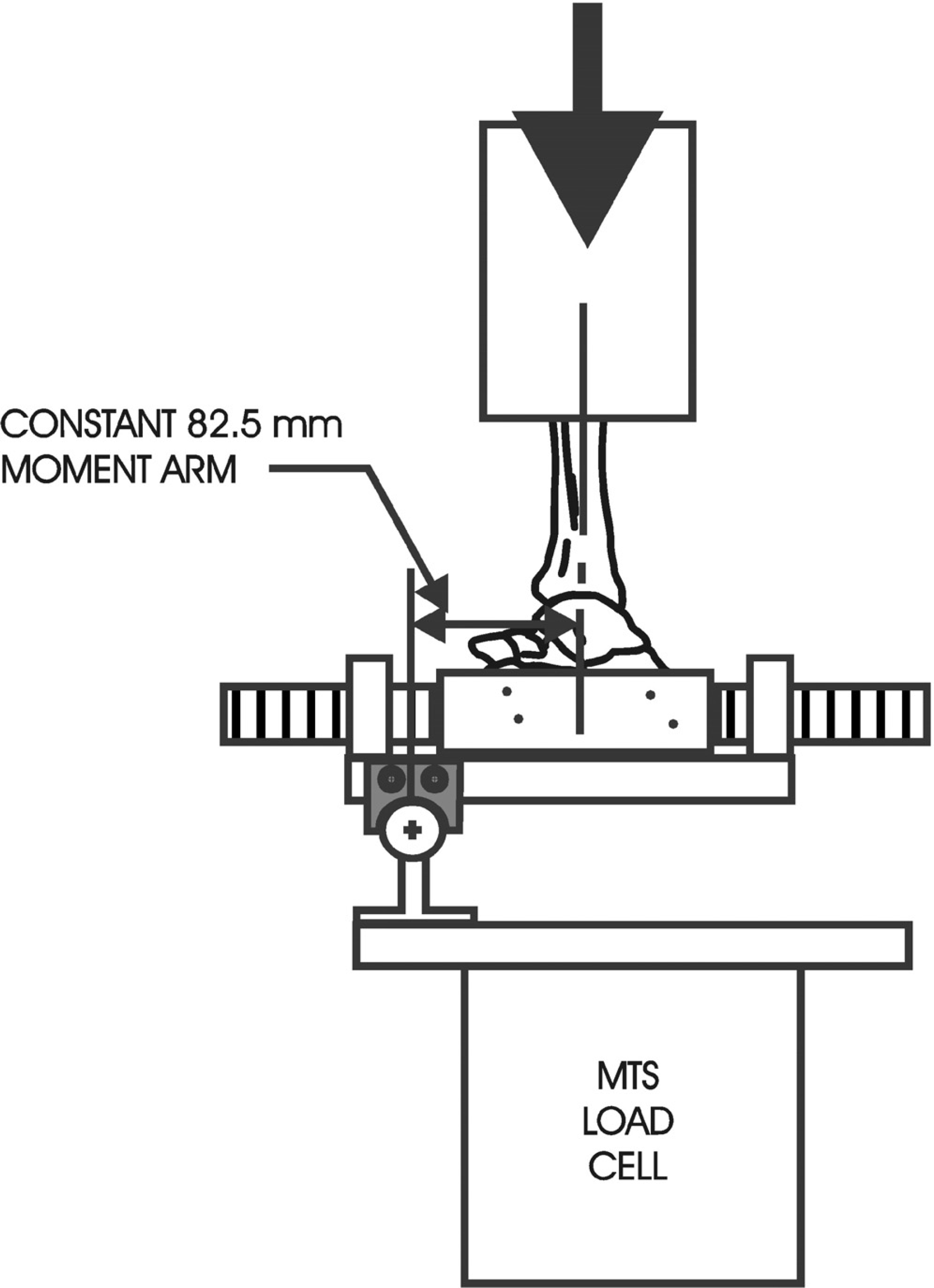
Schematic of test set-up for test of stiffness and load-to-failure dorsiflexion. The circle with the (+) in the center is the axis of rotation.
The average bone mineral density for the samples was 0.49 g/cm 2 (range, 0.28 to 0.73 g/cm 2 ). There was a correlation between bone mineral density and the difference in construct deformation with both posterior-to-anterior and lateral-to-medial screw orientation (r = 0.76, p = 0.03) (Figure 6). Analysis was based on logarithmic transformation due to the unequal variances of the data.
DISCUSSION
Several clinical and biomechanical studies have found overall good results for fixation of tibiotalocalcaneal arthrodesis with a retrograde IM rod and transverse lateral-to-medial distal screws 5,10,15,16 or with a blade plate, cannulated cancellous screws, external fixation, or a combination of these methods. 1,4,9,17,19,20,22 However, there are few clinical studies with a large series of patients because tibiotalo-calcaneal arthrodesis is a relatively uncommon procedure used primarily in challenging end-stage salvage situations in which patients are heterogeneous and comparison can be difficult. 5 These patients often are posttraumatic, diabetic, postsurgical, or infected, which makes this patient population more difficult to study. In an ideal situation with a normal physiologic bone healing environment and normal patient compliance, such as strict nonweightbearing and immobilization until healing, any means of fixation, even Kirschner wires or staples, is acceptable. However, candidates for TTC fusion often are disabled orthopaedically or medically and are unable to be immobile or limit weightbearing on the limb. Poor bone stock often is a concern. Given these factors, optimally stable fixation plays a critical role in patients who have TTC fusion.
Several biomechanical studies have used various testing methods to compare available methods for TTC fusion. A biomechanical cadaver study by Berend et al. 3 with bending and torsion testing showed that retrograde IM rod fixation was stronger than two crossed cannulated screws in dorsiflexion, plantarflexion, inversion, and eversion and with torsional force. In a biomechanical study using an artificial bone model by Nasson et al., 18 crossed screws produced superior stiffness in dorsiflexion and valgus stressing when compared with blade plate fixation for ankle arthrodesis. Chiodo et al. 4 found higher final stiffness and lower construct deformation with dorsiflexion loading for cadaver specimens fixed with a blade plate and a supplemental screw as compared with a retrograde IM nail system with distal screws placed lateral-to-medial. In a study testing the stiffness under external rotation loading of IM nail fixation, Mann et al. 13 showed that one posterior-to-anterior distal screw provided a significantly stiffer construct than one lateral-to-medial distal screw. That study did not test loading in dorsiflexion, plantarflexion, or inversion-eversion. Further, these investigators used a nail that is designed with the distal hole to accommodate a posterior-to-anterior screw and the other holes oriented at 90 degrees to the distalmost screw, allowing use of two lateral-to medial screws (ankle arthrodesis nail, Biomet, Warsaw, IN). With this device, the surgeon chooses to fill any number of these distal holes, but cannot insert all three screws lateral-to-medial or all three screws posterior-to-anterior. These investigators did not study the use of screws placed in both directions. The current study agrees with the findings of Mann et al. 13 in showing that an IM nail with posterior-to-anterior screw orientation provided more stable fixation, but the method of testing and the hardware and distal screw configuration options were substantially different.
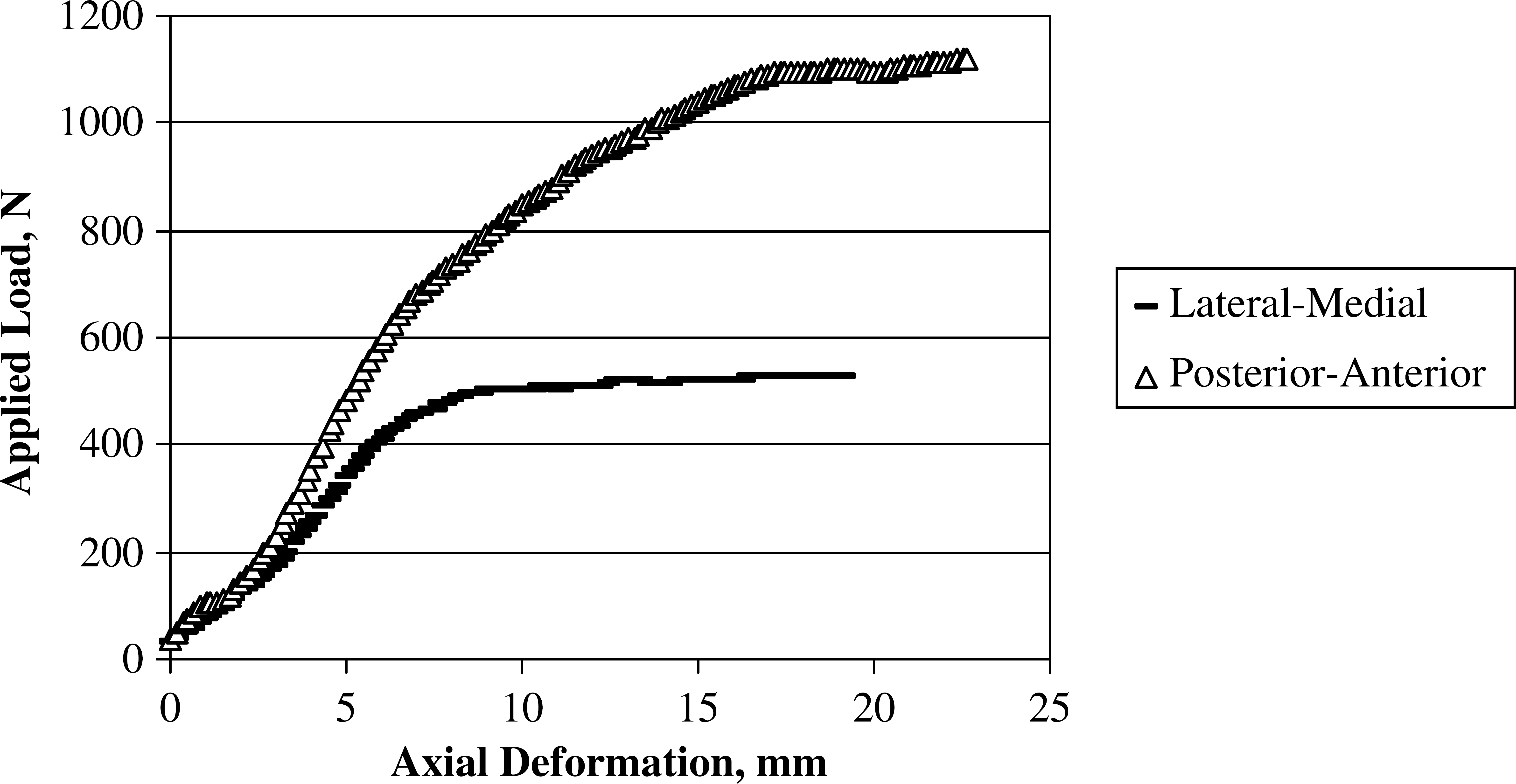
A representative load-deformation curve of one specimen tested with cyclic loading in dorsiflexion to a maximum of 260 N at a rate of 3 Hz for 250,000 cycles.
The current biomechanical model was limited to one loading direction and did not include plantarflexion, inversion-eversion, or internal-external rotation. Forces through the ankle act in all of these directions, and the fixation construct could be expected to experience different stresses with additional types of loading. We chose dorsiflexion as the loading method that we believed represented the stress found most often clinically in the postoperative period as the patient moves from heel to toe in gait. Dorsiflexion has the longest moment arm to achieve maximal stress on the fixation construct. Further, we tested the construct with loads higher than those experienced clinically in the postoperative period. Testing in dorsiflexion provides a useful view of fixation performance using IM nails with different screw positions, but other stresses should also be tested.
Many patients who have TTC arthrodesis have poor bone density as a result of diabetes, disuse osteopenia, advanced age, or inflammatory arthropathy, which creates a further challenge for the surgeon. 8,12,16 A recent biomechanical study reported a significant inverse relationship between bone density and construct deformation. 4 In the current study, there was a significant correlation between bone mineral density and construct deformation with both posterior-to-anterior and lateral-to-medial screw orientation. This finding suggests that posterior-to-anterior screw orientation may be the more stable of these two constructs, because it is less aversely impacted by bone mineral density. However, these preliminary findings on a small sample suggest that further studies on the effects of bone quality should be considered.
Final effective deformation was significantly lower with the posterior-to-anterior placed screws than with the lateral-to-medial screws (2.4 ± 1.5 mm compared to 3.8 ± 2.3 mm, p = 0.04) at a load of 250 N.
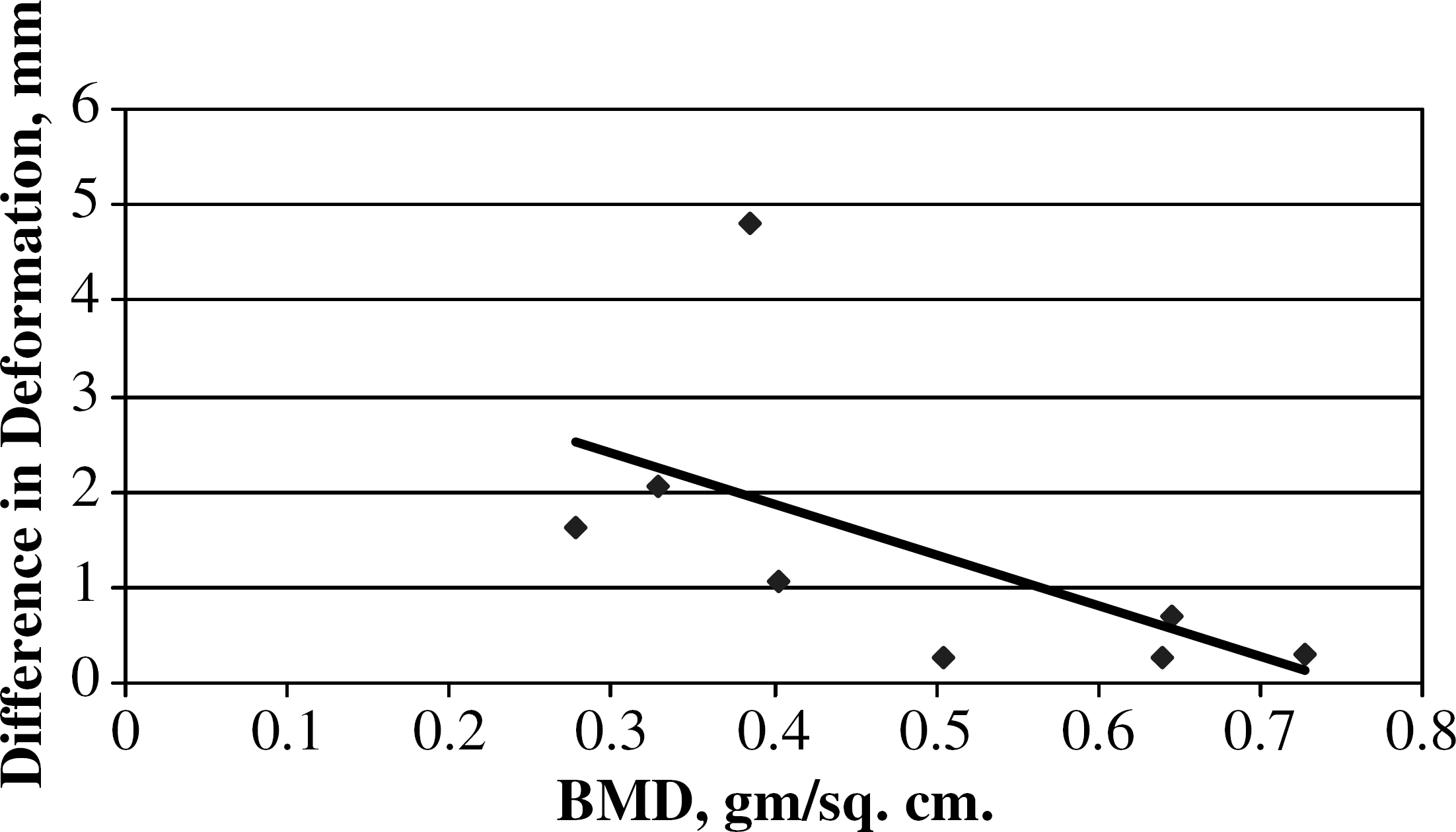
Correlation between bone mineral density (BMD) and the difference in construct deformation with posterior-to-anterior and lateral-to-medial distal screw orientation. The analysis was based on logarithmic transformation because of unequal variances in the data.
Our study used a short nail instead of the long nail used in a previous study by McGarvey et al. 14 A long nail may have an advantage in fixation across the isthmus of the tibia and may contribute to stiffness, but a longer nail often requires translation of the talus and calcaneus under the tibia medially. 14 In the current study, a medial malleolar osteotomy was not required because the rod could be inserted through the distal aspect of the tibia. Though this method may lack the potential benefit of stability of fixation associated with a long nail, we gained some natural stability by retaining the medial malleolus.
Stiffness was used to assess initial fixation, although many dependent variables can affect stiffness. Bone quality, characteristics of the hardware, placement of fixation, congruency of apposed surfaces, and method of insertion (with or without compression, amount of compression, use of lag or distraction mode), and method of stressing may all affect stiffness findings. We looked at stiffness because this allowed us to evaluate the construct as a whole, although independent variables that influence stiffness were not assessed.
Surgical stabilization with IM nailing in TTC arthrodesis has several theoretical advantages, including use of a load-sharing device, potential relative preservation of the soft tissue envelope, and ability to use a reproducible technique, but there is room for improvement with regard to the successful fusion rate. Future biomechanical studies could compare IM rod fixation with posterior-to-anterior distal screw placement to blade plate and screw fixation, especially with a consideration of the effects of bone density differences.