
Abstract
Background:
The purpose of this study was to evaluate the cost and benefit of routinely submitting hammertoe specimens for histopathological examination. We hypothesized that such examination rarely shows a new diagnosis and seldom alters postoperative care.
Materials and Methods:
Three hundred and fourteen proximal interphalangeal (PIP) joint and 37 extensor tendon specimens from 187 consecutive hammertoe correction surgeries were submitted by 2 surgeons for histopathological examination between January 2009 and December 2011. Each patient’s chart was reviewed to determine whether the histopathological examination revealed a diagnosis other than degenerative joint or degenerative tendon and whether subsequent patient management was altered. The total reimbursements for professional charges were calculated using the average reimbursement from common insurance providers for two Current Procedural Terminology (CPT) codes: 88304 (soft tissue examination) and 88311 (decalcification).
Results:
Almost all of the specimens were diagnosed as degenerative: 97.5% (307/314) of the PIP specimens and all (37/37) of the tendon specimens. Seven PIP specimens (2.2%, 7/314) from 5 patients (2.7%, 5/187) and no tendon specimens had other diagnoses. These diagnoses were rheumatoid arthritis (5/314, 1.6%), osteomyelitis (1/314, 0.3%), and pigmented villonodular synovitis (PVNS) (1/314, 0.3%). Only the PVNS was a new diagnosis. A total of $56,750 was spent to determine 1 new diagnosis.
Conclusion:
The routine submission of hammertoe specimens for pathological evaluation was not cost-efficient. Our analysis showed that new diagnoses were rarely found and patient management was not affected.
Level of Evidence:
Level IV, retrospective case series.
“Hammertoe” generally refers to a plantar flexion deformity of the proximal interphalangeal (PIP) joint of the lesser toes. 12 In rare cases, the cause is congenital. When acquired, hammertoe occurs due to a musculoskeletal imbalance of the intrinsic and extrinsic muscles of the lesser toes. 3 Trauma and/or inflammatory joint diseases affecting the joint capsule, synovium, collateral ligaments, and musculature may cause unstable joints and ultimately hammering. Perhaps the most common cause is overload of the lesser metatarsals that occurs in the setting of hallux valgus. 2
The routine histopathological examination of surgical specimens after hammertoe reconstruction surgery is a standard practice at our institution. The Joint Commission on Accreditation of Healthcare Organization requires surgeons, pathologists, and administrators to determine and agree which surgical specimens are required to be submitted and which specimens do not need to be submitted. This list of which specimens do not need to be submitted must be part of the policy manual for institutional operating rooms. 5 A routine histopathological examination is used to establish or confirm a diagnosis, guide future management of the diagnosis, and understand the pathophysiological characteristics of the disease.1,6 It also gives hospitals a system for quality control and medicolegally documents the procedures performed.1,6
In a previous study, we assessed the routine submission of specimens after hallux valgus surgery and noted that a new diagnosis was made in only 1 case and management was changed in no cases despite a total cost of $42,027. The conclusion from that study was that the routine submission of hallux valgus specimens was not cost-effective as new diagnoses were rarely made and postoperative management rarely changed. 9
The specimens that can be routinely submitted for histopathological analysis at the time of corrective hammertoe surgery are extensor tendon segments cut during extensor brevis tenotomy and bone from the PIP or distal interphalangeal (DIP) joints used during resections to correct rigid hammertoes. We conduct PIP/DIP resections through completely separate incisions over the respective joints. The extensor tenotomy is performed through an incision made over the dorsum of the foot: the extensor longus is “z-lengthened,” whereas the extensor brevis is tenotomized and a section sent for pathological evaluation. Histopathological evaluation can theoretically aid in management when an infection or other metabolic or inflammatory disease is present. 10
The cost-effectiveness of routine pathological evaluation in hammertoe reconstruction surgery has not been investigated. The purpose of this study was to determine the cost and benefit of such evaluation. We sought to determine how many histopathological examinations reported a diagnosis other than degenerative joint disease (DJD) in the case of joint specimens and “degeneration” or “normal” in the case of tendon specimens. When other diagnoses were present, we aimed to determine how many were new diagnoses and how many altered patient care. We hypothesized that almost all histopathological diagnoses would be DJD for the joint specimens and “degeneration” and “normal” for the tendon specimens. Of the diagnoses that were not, we predicted that the diagnosis would already be known prior to surgery and would not affect postoperative management. Using this data we could determine the cost and benefit to patients from routinely submitting specimens from hammertoe reconstruction surgery.
Methods
This study was carried out as a retrospective review of 187 consecutive surgeries that included hammertoe reconstruction performed between January 2009 and December 2011 by 2 trained foot and ankle surgeons. There were a total of 176 patients, 11 of whom underwent bilateral surgery. The condyles resected from PIP resections were routinely submitted for histopathological analysis for gross and microscopic assessment. Depending on how many toes the patient had reconstructed, 1 to 4 PIP specimens were submitted. Extensor tenotomy and release was not performed in all cases. When performed, it was not always submitted despite hospital requirements. From the consecutive surgeries reviewed, there were a total of 314 PIP joint and 37 extensor tendon specimens. A chart review was performed in each case in order to find and record preoperative diagnoses. Pathology reports were prepared by 1 of 3 board-certified pathologists working full time at our institution. The reports for each patient and specimens were also reviewed in order to record the final histopathological diagnoses.
To test the hypothesis that routine histopathological analysis rarely reveals a diagnosis other than DJD in the case of joint specimens and “degeneration” or “normal” in the case of tendon specimens, the number of new diagnoses was calculated as a percentage of the total number of the joint and tendon specimens evaluated. To account for systemic diseases such as rheumatoid arthritis that would be found in multiple specimens from the same patient, the number of patients with an alternate diagnosis was calculated as a percentage of the total number of patients. To test the hypothesis that routine histopathological examination rarely alters postoperative management, the number of cases in which postoperative treatment was altered given the results of the examination was calculated as a percentage of the total number of cases sent for review. To determine the professional cost of histopathological examinations, we used the Current Procedural Terminology (CPT) codes 88304 (soft tissue examination) and 88311 (decalcification), which are the CPT codes billed for the analysis and preparation of the specimens, respectively. The former code is for a professional fee paid to the pathologist for the interpretation of the specimen. The latter is a general fee for the preparation of the specimen, even though in some cases it is not always decalcification (ie, as in the case with the tendons). The average reimbursement for each CPT code was calculated using data from the 5 most commonly used payers at our institution. All reimbursements were calculated using 2011 data. To calculate cost-effectiveness, the cost per new diagnoses was computed by dividing the overall reimbursement by the number of new diagnoses.
Results
Patient History and Demographics
Before surgery, 3 patients were diagnosed and treated for rheumatoid arthritis, 1 patient was diagnosed with osteomyelitis, and 1 patient had a history of cancer. The remaining 171 patients had no previous diagnosis of a systemic disease that could have caused hammertoe deformity. Of the patients analyzed, there were 26 males and 150 females, who had a mean age of 61.9 years (range, 23-100 years).
Assessment of Histological Diagnosis
The histopathological examination results reported DJD in 97.5% (307/314) of the PIP specimens, degeneration in 91.9% (34/37), and “normal” in 8.1% (3/37) of the tendon specimens. The 7 different PIP specimen diagnoses (2.2%, 7/314) resulted from 5 patients (2.6%, 5/187): rheumatoid arthritis (1.6%, 5/314 specimens and 1.6%, 3/187 patients), osteomyelitis (0.3%, 1/314 specimens and 0.5%, 1/187 patients), and pigmented villonodular synovitis (PVNS) (0.3%, 1/314 specimens and 0.5%, 1/187 patients). PVNS was the only new diagnosis (Figure 1). In no case did the results of histopathological examination alter patient management.
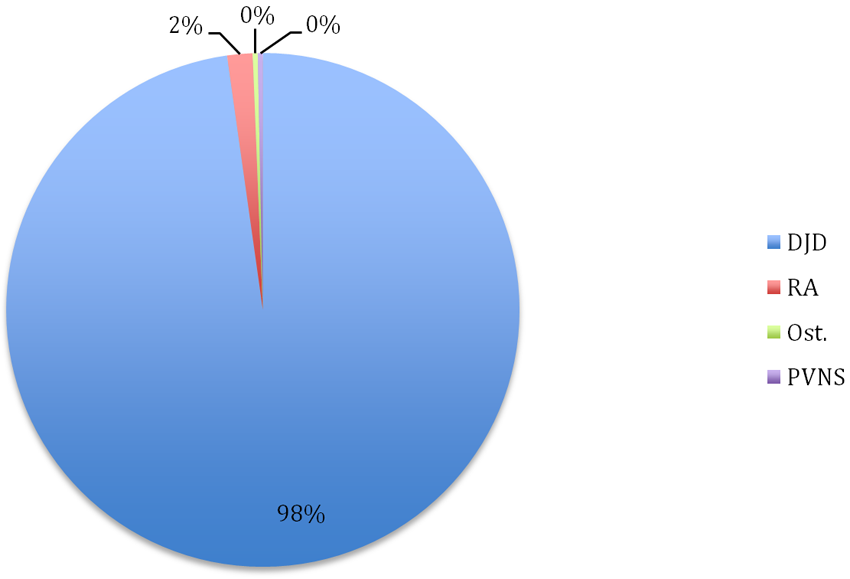
Pathological diagnosis. Histopathological diagnoses in hammertoe specimens are expressed as a percentage of the total number of specimens submitted for review. DJD, degenerative joint disease; Ost, osteomyelitis; PVNS, pigmented villonodular synovitis; RA, rheumatoid arthritis.
Cost-Effectiveness
Reimbursement for the professional fees of the histopathological examination for the CPT codes 88304, soft tissue examination, and 88311, decalcification, differed by payer. The average reimbursement for the 5 most commonly used payers for the CPT code 88304 was $126.25 and for the CPT code 88311 was $35.42 (Table 1). Thus, the total average reimbursement for both codes was $161.68. When we combined the 314 PIP specimens and the 37 tendon specimens analyzed, $56,749.68 was spent to establish 1 new diagnosis. Patient management was never changed, so the same amount of money was spent for no change in patient care.
Pathology Fee Reimbursement by Provider a
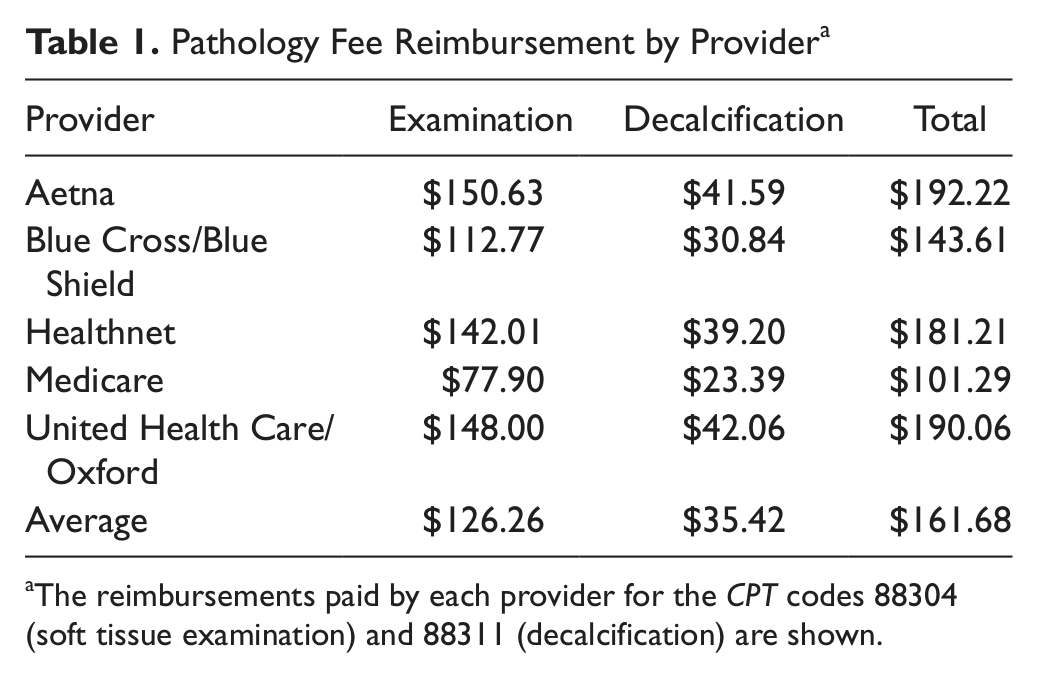
The reimbursements paid by each provider for the CPT codes 88304 (soft tissue examination) and 88311 (decalcification) are shown.
Discussion
The majority of the PIP specimens and all of the tendon specimens from the hammertoe reconstruction surgeries showed degeneration. There were only 7 other diagnoses in 5 patients. The only new diagnosis was PVNS, but this was in a patient with a history of cancer. The management did not change for any of the patients. Therefore, we conclude that the routine submission of hammertoe specimens is not warranted.
There have been numerous previous analyses of the routine submission of specimens for histopathological examination during hip and knee arthroplasty and hand and wrist surgeries. Guitton et al 4 examined the necessity of submitting specimens after operative excision of wrist ganglions. Of the 429 specimens they reviewed, 98.6% (424/429) were concordant diagnoses, 1.4% (5/429) were discrepant diagnoses, and 0 were discordant diagnoses. The investigators concluded that not submitting a specimen for routine histopathological review would not alter quality of care. 4 Lawrence et al 7 analyzed 1388 consecutive primary knee and hip arthroplasties in 1136 patients. Twelve pathological or impending fractures were diagnosed preoperatively and then confirmed intraoperatively. From the histological results, 11 of the specimens were malignant and 1 showed evidence of a benign rheumatoid geode. The histological results of the remaining 1376 arthroplasties confirmed the preoperative diagnoses of a benign cause. The authors found that the surgeons’ clinical diagnoses had a sensitivity of 100% and therefore no harm would come from ceasing to submit specimens for routine histopathological examination for hip and knee arthroplasties. 7 Lin et al 8 retrospectively examined 1363 routine elective primary hip or knee joint arthroplasties in 1247 patients. The investigators grouped the diagnoses into 3 classes based on the following definitions: concordant (clinical and histological diagnoses agreed), discrepant (clinical and histological diagnoses differed but resulted in no change in treatment), and discordant (diagnoses differed, which resulted in a change in treatment). After comparing preoperative, postoperative, and histopathological diagnoses, the investigators found that 97.9% (1335/1363) were concordant, 2.1% (28/1363) were discrepant, and none were discordant. The investigators concluded that routine histopathological submission of specimens from elective primary arthroplasty surgeries increased medical costs and rarely changed patient management. 8
Besides the previously mentioned investigation of routine submission of specimens from hallux valgus surgery, there have been no additional analyses of routine histopathological submission from foot and ankle surgeries. Furthermore, no such studies have specifically addressed hammertoe specimens. 9
The most common cause of hammertoe is mechanical. Hammertoe can be caused by the imbalance of the intrinsic and extrinsic muscles of the toes or from overloading of the lesser toes from hallux valgus. Although rare, trauma or inflammatory joint disease can destabilize the lesser toe joints and cause a hammertoe deformity. 11 The pathological assessment provided by routine submission of specimens for histopathological assessment does not aide the mechanical diagnosis. For the rarer causes of hammertoe, the pathological assessment would most likely only confirm the surgeon’s diagnosis, as these causes can be found clinically. 10 The treatment for correcting the hammertoe would proceed the same way regardless of the pathological results.
The major limitation of this study is the retrospective nature of this study. In addition, extensor tendons were not submitted for all toes. Finally, we did not create a more elegant metric of cost-effectiveness, as did some previous studies. 8
In conclusion, this study was the first to assess routine submission of specimens from hammertoe reconstruction surgeries that we found to not be cost-effective. In an age of increasing health care costs, ceasing the routine submission would better direct our health care expenditures. We should continue to develop metrics to measure the cost of effectiveness of our health care practices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.