
Abstract
Background:
For triple arthrodesis, a single medial incision has been proposed to avoid lateral wound complications and has demonstrated satisfactory fusion rates. This study aimed to compare the disruption to the arterial supply of the talus between the single-medial-incision approach and the 2-incision approach.
Methods:
The 2 approaches for triple arthrodesis were compared by analyzing the disruption of arterial vasculature in 14 cadaveric specimens in randomized fashion. The arterial disruption was determined using CT angiography before and after surgery combined with analysis from dissection. The area of joint preparation from each technique was also analyzed and compared.
Results:
The single-medial-incision approach caused a high incidence of damage to the deltoid artery (6 of 7 specimens, 86%) and the artery of the tarsal canal (7 of 7 specimens, 100%). The 2-incision approach resulted in damage to the artery of the tarsal sinus in all specimens (7 of 7 specimens, 100%), but the medial vasculature was spared given the limited dissection required to access the talonavicular joint. Through the single-medial-incision approach the percentage of debridement of the calcaneocuboid joint (36%) was significantly lower than the debridement using the 2-incision approach (85%, P < .01). There was no significant difference in joint preparation of the talonavicular and subtalar joints between the 2 approaches with the number of specimens available.
Conclusion:
From this cadaveric study, we found that both approaches could result in substantial disruption of the main blood supply to the talus. The single-medial-incision approach consistently disrupted the majority of blood supply to the talar body, while the 2-incision approach caused various degrees of vascular disruption to the talar head and neck. Using the single-medial-incision approach, the calcaneocuboid joint did not show adequate removal of articular cartilage due to difficulty accessing the joint surfaces.
Clinical Relevance:
Vascular sparing to the talus should be considered when selecting an appropriate operative approach for triple arthrodesis. Although the clinical significance of this cadaveric study is limited, the 2-incision approach appeared to cause less vascular disruption to the talar body while allowing more complete joint preparation.
Adequate blood supply to the talus is an important consideration for successful fusion following a triple arthrodesis.25,28 Damage to the main arterial supply of the talus, which includes the artery of the tarsal canal, deltoid artery, and artery of the tarsal sinus, may occur during such procedures. 7 Disruption to 1 or more of these arteries could compromise blood supply and result in complications such as nonunion or even avascular necrosis (AVN).15,21,23 Therefore, in addition to adequate joint surface preparation, preservation of blood supply to the osseous framework is essential for effective fusion and to reduce the likelihood of other complications. Occasionally triple arthrodesis is combined either concomitantly or as consecutive surgeries with a total ankle replacement for alignment correction of the hindfoot.16,32 AVN or a decrease in blood supply to the talus can result in failure of the joint replacement and is a contraindication to the procedure. 11
Triple arthrodesis commonly involves a combined medial and lateral incision, which is thought to allow the best access to the talonavicular, subtalar, and calcaneocuboid joints for debridement and preparation.3,8 While this approach is widely accepted, lateral incision complications such as difficult wound healing can occur especially in cases with severe pes planus deformity causing contracture of the lateral soft tissue.6,9,13,18,29,30 This has encouraged some surgeons to prepare all joints with a single medial incision when severe planovalgus deformity is present, thus avoiding the lateral wound.12-14,19 The change in the operative approach for triple arthrodesis could influence the effectiveness of joint preparation and/or the degree of damage to the blood supply of the talus.
The purpose of this study was to quantify the resultant vascular disruption of the talus from 2 approaches for the triple arthrodesis (single medial incision vs 2 incisions) using CT angiography and subsequent guided dissection. A comparison of joint preparation between the 2 approaches was also evaluated.
Methods
A total of 14 unembalmed cadaveric lower limb specimens without obvious deformity or evidence of prior surgery were used to demonstrate disruption of peritalar arterial supply coupled with an operative approach. Seven paired limbs were used. Average age of the specimens was 82 years (range, 51-94 years). Specimens were blindly assigned to an operative approach using a random number table: 7 legs were assigned to the single-medial-incision approach and 7 were assigned to the 2-incision approach.
The arterial vasculature of each limb was investigated after injections of barium sulfate and latex suspension into the posterior tibial, anterior tibial, and peroneal arteries with an 18-gauge needle coupled to a 30 mL syringe. A small skin incision was made in the first web space at the level of the metatarsophalangeal joints. This incision provided access for visualization of the latex suspension to ensure penetration to the distal vessels in the foot. Each leg was imaged before surgery using a high-resolution, 3D computed tomography scanner. For imaging, each limb was placed in a support frame with the ankle at neutral position and scanned in 1 mm sections from the plantar surface through midtibia. Postscan analysis and 3D reconstruction were completed using software (Osirix, Pixmeo SARL, Switzerland). Peritalar arterial patterning was observed and recorded.
All operative procedures were completed by a fellowship-trained orthopaedic surgeon (PP). For the single-medial-incision approach, a single medial incision was used for all joint preparation (Figure 1). A straight longitudinal incision was made starting from the tip of the medial malleolus toward the center of the naviculocuneiform joint medially. Subcutaneous tissue was incised sharply along the incision. The tibialis posterior tendon sheath was opened and the tendon was retracted posteriorly. Sharp dissection was then carried along the medial aspect of the talonavicular joint toward the palpable middle and posterior facets of the subtalar joint. The interosseous ligament was released, and a Hintermann distractor was used to distract the subtalar and talonavicular joints. The joint debridement was accomplished using curettes and osteotomes, while preserving the subchondral bone. The calcaneocuboid joint was then debrided using the same technique through the distracted talonavicular interval.
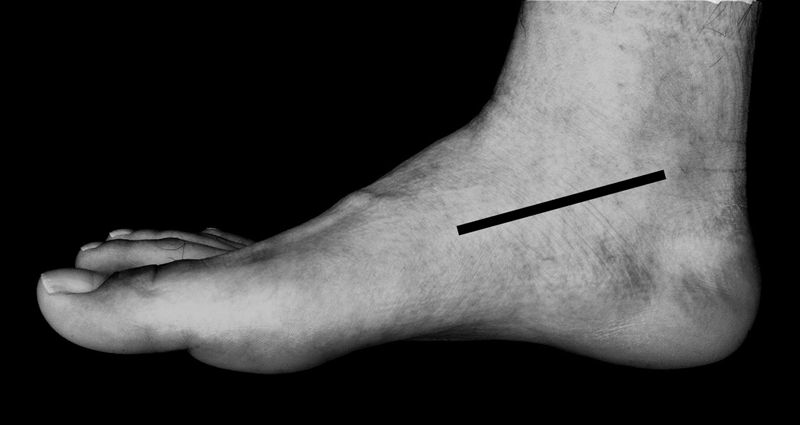
The picture demonstrates the skin incision for the single-medial-incision approach on a right foot.
For the 2-incision approach, a curvilinear incision was made beginning from the posterior aspect of the tip of the lateral malleolus toward the anterior process of the calcaneus, and then curved to the base of the fourth tarsometatarsal joint (Figure 2). Subcutaneous tissue was incised sharply along the incision. The extensor digitorum brevis muscle was then incised and retracted medially. The inferior extensor retinaculum, cervical, and interosseous talocalcaneal ligaments were sharply released. With distraction provided by the Hintermann distractor, cartilage from the subtalar and the lateral part of the talonavicular joints was debrided using curettes and osteotomes, while preserving the subchondral bone. The calcaneocuboid joint was directly identified and the capsule was excised. The joint was distracted and debrided in the same fashion. The medial part of the talonavicular joint was distracted and debrided through a separated 4 cm incision just lateral to the tibialis anterior tendon.
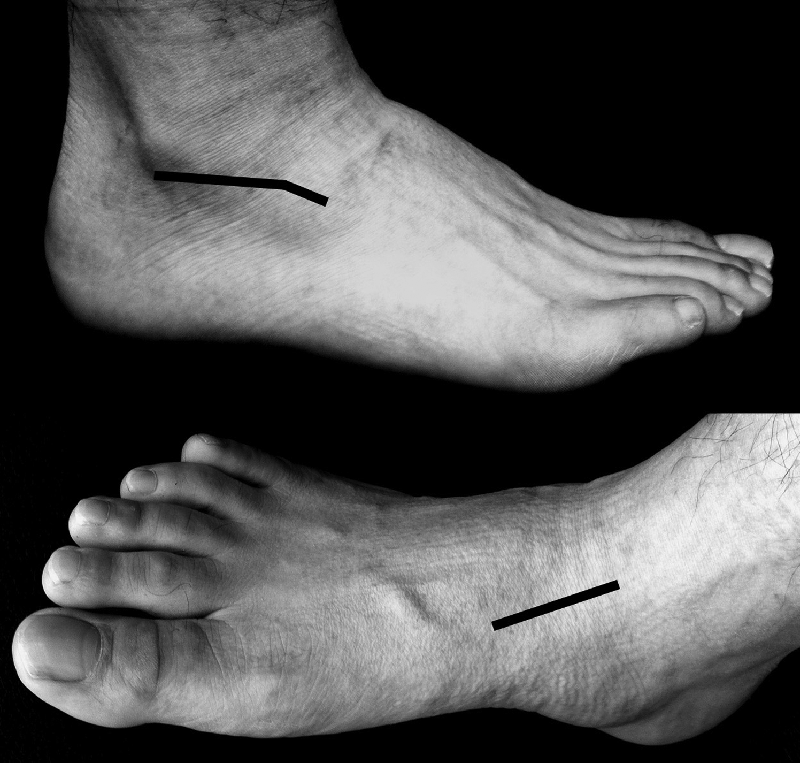
The picture demonstrates the skin incisions for the 2-incision approach on a right foot.
After surgery, the legs were again imaged using a CT scanner and analyzed using 3D reconstruction techniques to determine disruptions of peritalar arterial branches as compared to the images before surgery (Figures 3 and 4). Following the imaging, each leg underwent guided dissection aided by the CT reconstructions and loupe magnification (×3.5). Dissection of main arteries and their branches known to supply the talus proceeded in a proximal to distal direction. The latex dye further assisted in detection of vascular disruption and allowed more accurate observation of the vascular patterning. An experienced anatomist (MP), who was not directly involved in the operative procedure, reviewed and confirmed all vascular disruptions.
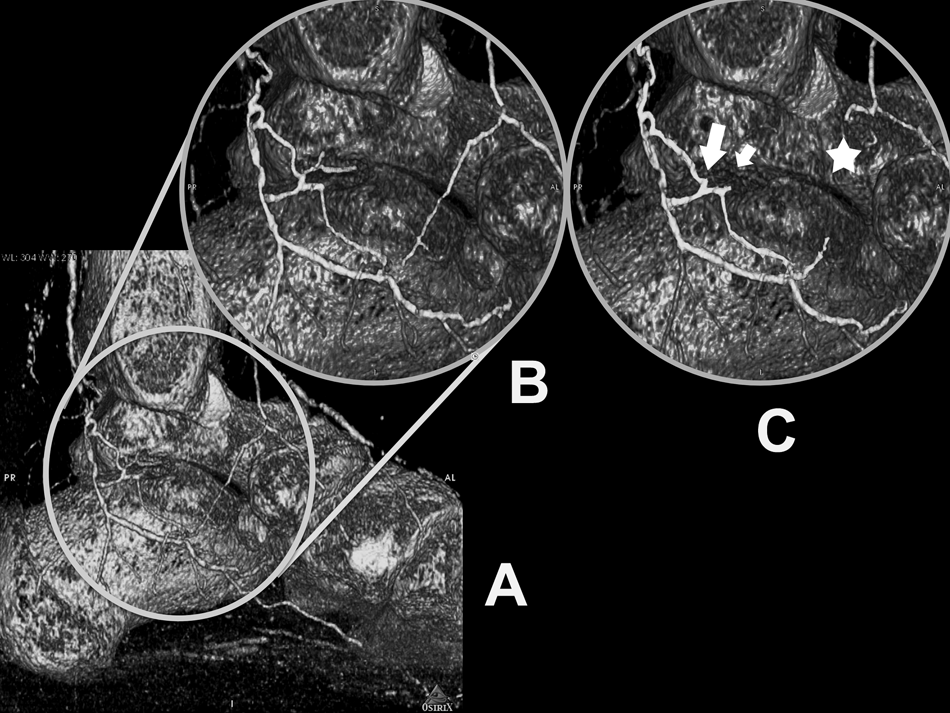
CT angiography with 3D reconstructions displays the arterial patterning of an intact left hindfoot observed from the medial aspect. This specimen was assigned to the single-medial-incision approach. Before surgery, imaging study (A) and its magnified view (B) demonstrate the arteries supplying the talus. After surgery, the imaging study indicates disruptions of the deltoid artery (large arrow), artery of the tarsal canal (small arrow), and the medial recurrent tarsal artery (star).
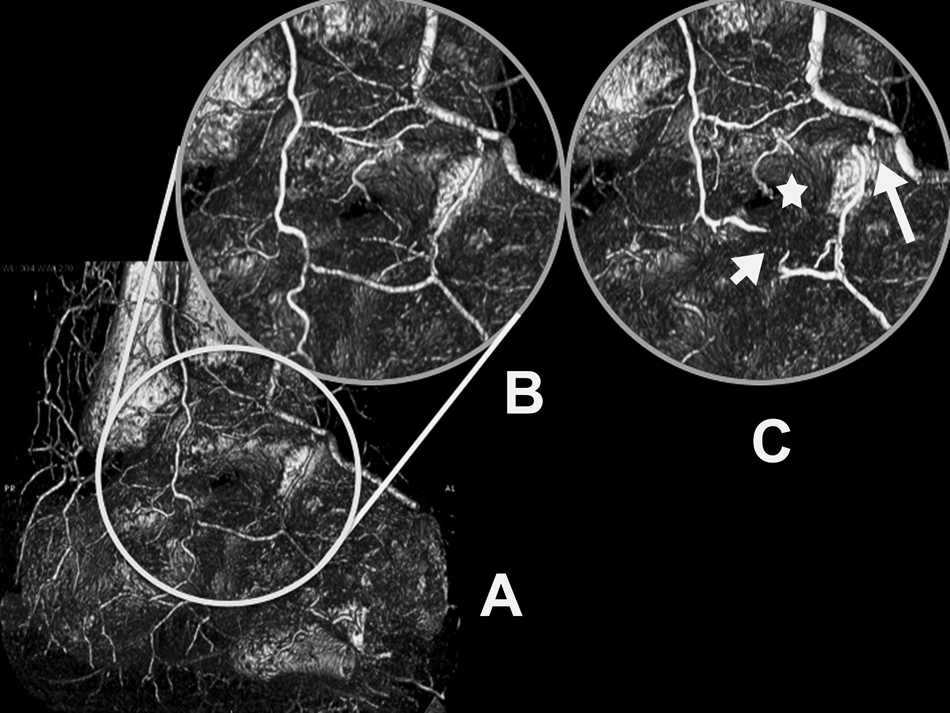
CT angiography with 3D reconstructions displays the arterial patterning of an intact right hindfoot observed from anterolateral aspect. This specimen was assigned to the 2-incision approach. Before surgery, imaging study (A) and its magnified view (B) demonstrate the arteries supplying the talus. After surgery, imaging study indicates disruptions of the lateral tarsal artery (long arrow), posterior recurrent branch of the lateral tarsal artery (short arrow), and the artery of the tarsal sinus (star).
The debridement of the articular surfaces of the talus, calcaneus, navicular, and cuboid were analyzed using a translucent-film mapping technique. 33 While the joints were stabilized in neutral position using K-wires, the articulating joint surfaces were outlined with marker and cleared of any remaining tissue. Each joint surface and the remaining articular cartilage was outlined and traced using semitransparent paper. The mapping of each articular surface was scanned and the total surface area and area of remaining articular cartilage were calculated using image-analysis software (Image-J, Wayne Rasband, National Institutes of Health, Bethesda, MD). Two members of the research team (JH and TV) who were not directly involved with the operative procedure completed and analyzed the mapping.
The frequency of each arterial injury was compared between the 2 approaches using Fisher’s exact test. The area of joint preparation from each technique was also analyzed and compared using a paired t test. A P value of less than .05 was used for statistical significance.
Results
After surgery, CT angiogram guided dissection revealed that both approaches caused damage to 1 or more of the 3 main arteries supplying the talus (Table 1). The single-medial-incision approach was found to consistently damage both the deltoid artery and the artery of the tarsal canal in most specimens, while the artery of the tarsal sinus was always disrupted by the 2-incision approach. The frequencies of arterial disruption for all the 3 main branches were significantly different between approaches (all P < .01). Other arteries that were occasionally injured in the 2-incision approach were proximal branches of the dorsalis pedis that supply the head of the talus including the lateral talar artery and the medial talar artery. The medial recurrent artery was damaged in all specimens regardless of their assigned approach. There was no significant difference in the frequency of disruption of the lateral branches, including lateral tarsal artery, anterior lateral malleolar artery, and posterior recurrent lateral talar artery with the number of specimens available.
Summary of Arterial Disruption Between the 2 Approaches
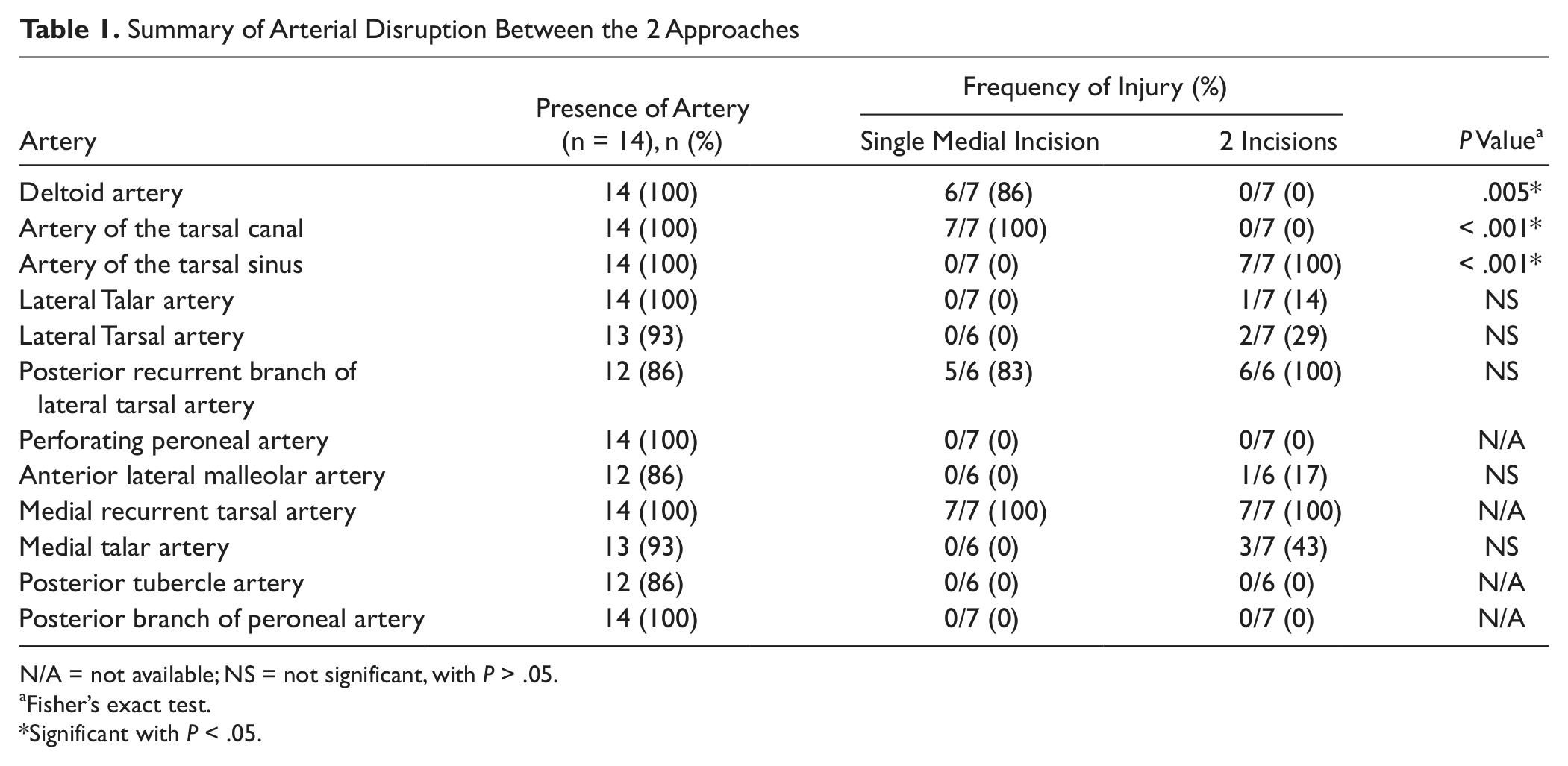
N/A = not available; NS = not significant, with P > .05.
Fisher’s exact test.
Significant with P < .05.
Analysis of the articular surfaces joint preparation (Table 2) showed that, with the number of specimens available, there was no significant difference in the mean percentage of joint debridement for the talonavicular and subtalar joints, when comparing single-medial-incision and 2-incision approaches, respectively. There was also no difference when each facet of the subtalar joint was compared separately. However, there was a significant difference between the 2 approaches when comparing the joint preparation at the calcaneocuboid joint. The 2-incision approach accomplished more complete joint debridement at the calcaneocuboid joint compared to the single-medial-incision approach.
Average Joint Debridement Between the 2 Approaches
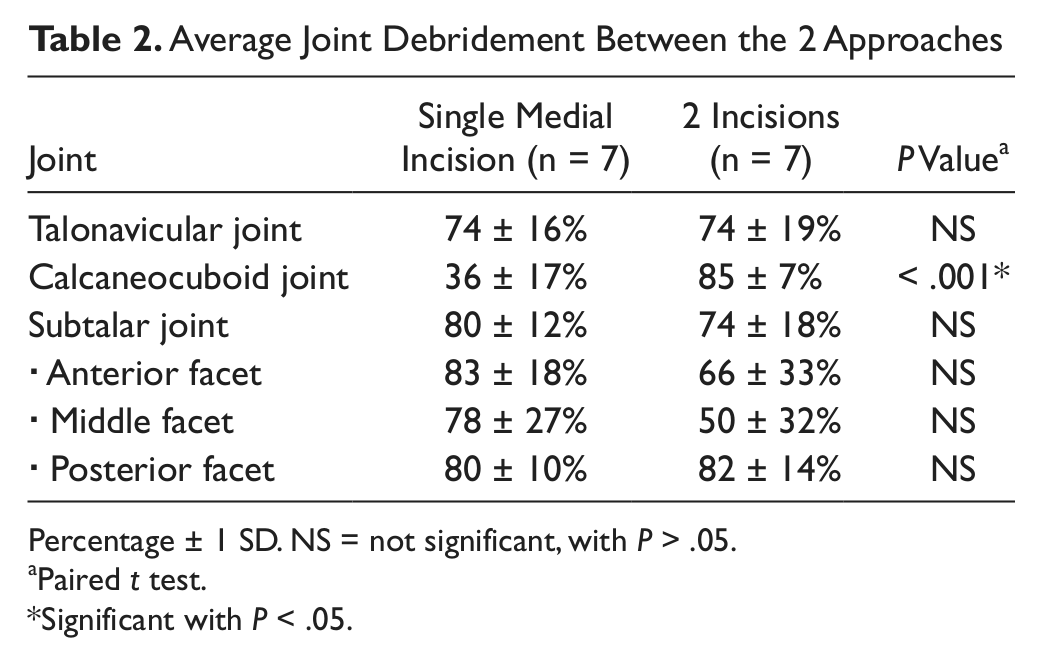
Percentage ± 1 SD. NS = not significant, with P > .05.
Paired t test.
Significant with P < .05.
Discussion
We have found that substantial damage could occur to the peritalar arterial blood supply from either single-medial-incision or 2-incision approach used for triple arthrodesis. The peritalar vascular map as outlined by Mulfinger and Trueta 26 in 1970 and by Gelberman and Mortensen 7 in 1983 clearly described the contributions of both extraosseous and intraosseous vessels to the talus. These primary vessels include the artery of the tarsal canal, artery of the tarsal sinus, and the deltoid artery (Figure 5). Using this information, the combined damage to the artery of the tarsal canal and the deltoid artery that consistently occurred from the single-medial-incision approach may theoretically reduce blood flow to three-fourths of the talar body (middle one-half and medial one-fourth), assuming similar arterial pressures and distribution. The damage to the artery of the tarsal sinus that consistently occurred from the 2-incision approach could theoretically reduce blood supply to the lateral one-fourth of the talar body and the inferior lateral one-third of the talar head. Concerning the integrity of the talar body, the 2-incision approach appeared to cause less arterial disruption to the area. While the interpretation of vascular disruption to the talus from Gelberman and Mortensen’s model clearly favored the 2-incision approach, the resulting damage to other contributing arterial branches has not been well studied. A recent study by Miller et al demonstrated the presence a rich anastomotic network of arterial supply to the talus both intraosseously and extraosseously. 24 A reduction in blood supply to the talus by disrupting arterial branches over a certain threshold may increase the risk of AVN similar to the phenomenon observed in a displaced talar neck fracture.4,7,10,15,21,23
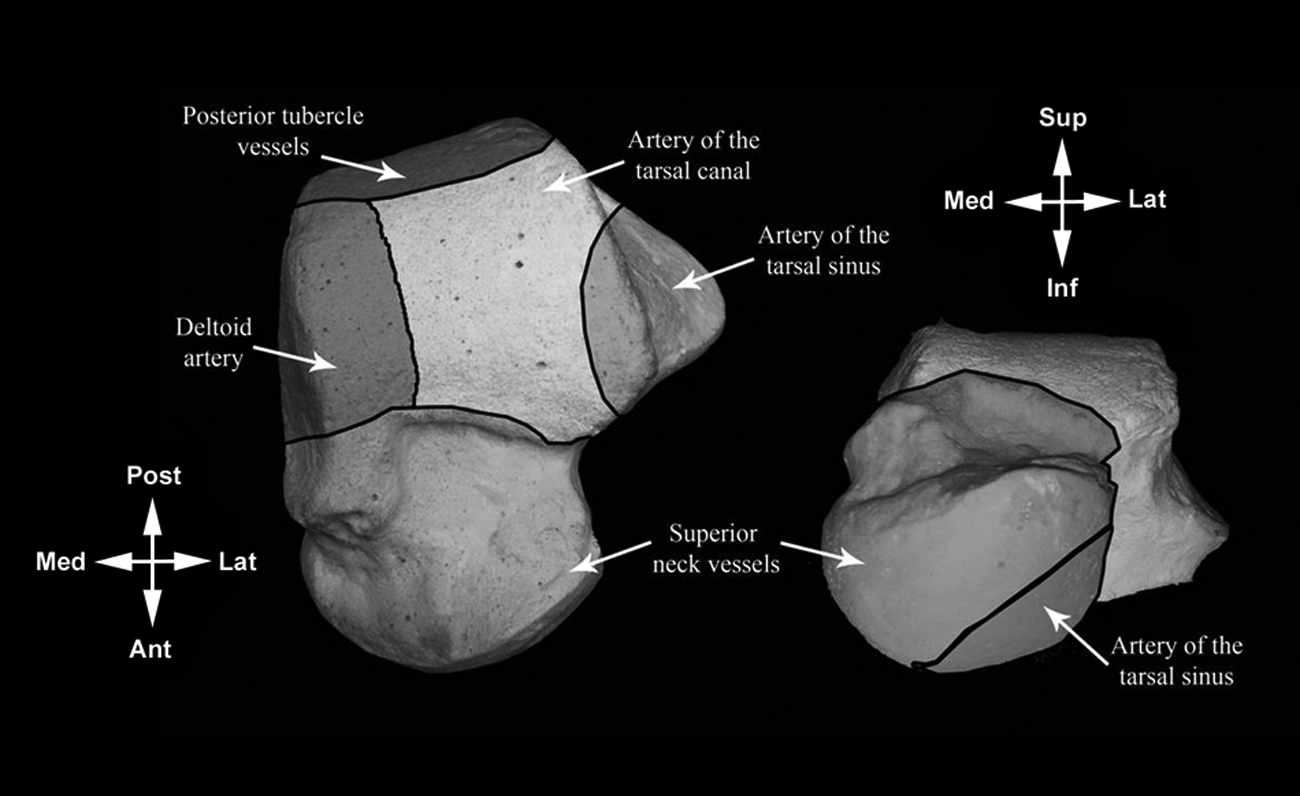
Intraosseous blood supply of the talus is demonstrated. The medial one-fourth, the middle one-half, and the lateral one-fourth of the talar body are supplied by the deltoid artery, the artery of the tarsal canal, and the artery of the tarsal sinus, respectively. The superomedial two-thirds of the talar head is supplied by the superior neck vessels, while the inferolateral one-third is supplied by the artery of the tarsal sinus. Adapted from Gelberman and Mortensen. 7
AVN of the talus is a rare but recognized complication after a triple arthrodesis.1,5,15,20,22,28 Pain and disability in patients with a collapsed talar dome often necessitated a conversion to pantalar arthrodesis or required a long-term ankle-foot orthosis.4,15,22 As observed in the current study, triple arthrodesis can result in major disruption to arterial branches along the path of dissection and joint preparation and necessitates considering vascular sparing when selecting an appropriate operative approach. For example, in patients with a history of previous surgery, an approach utilizing the same incision without disturbing the intact part of the vascular network is preferred. Further studies may determine whether CT angiography performed before surgery may provide useful information regarding the degree and location of preserved peritalar arterial branches.
We have found that both operative approaches could allow effective debridement of the subtalar and talonavicular joints. The calcaneocuboid joint preparation was more complete in the 2-incision approach which is in contrast to a cadaver study by Jeng et al, 13 where no difference was found. Several aspects the present protocol (eg, preservation of the tibialis posterior tendon, inferolateral part of the spring ligament, etc) and analysis (translucent film technique for joint debridement using independent evaluators) were different from those of the previous study. We believe the calcaneocuboid joint is difficult to access from the single-medial-incision approach due to the curvature of the joint surfaces and the difficulty of accessing the joint from across the foot through the talonavicular joint. In the absence of arthritis of the calcaneocuboid joint, several authors recommended using a single medial approach to limit dissection and operative time17,31,34 while correcting hindfoot deformities as effectively as the triple arthrodesis.2,13,14,27,34
This study has limitations due to the use of specimens from donors with an average age of 82 years. The relative stiffness of the specimens and the inadequate soft tissue release may have made the exposure more difficult although all of them were free of obvious arthritic changes. We also could not define the contribution of vascular disruption from other vascular branches other than those described by Gelberman and Mortensen. 7 Further studies using gadolinium-enhanced magnetic resonance imaging or other injection techniques may be able to elucidate the effect of triple arthrodesis more realistically providing the peritalar anastomoses are taken into account. 24
In conclusion, substantial damage can occur to the peritalar arterial blood supply from both single-medial-incision and 2-incision approaches for a triple arthrodesis. The single-medial-incision approach consistently disrupted the majority of blood supply to the talar body, while the 2-incision approach caused various degrees of vascular disruption to the talar head and neck. Using the single-medial-incision approach, the calcaneocuboid joint did not show adequate removal of articular cartilage due to difficulties accessing the joint surfaces from the medial aspect across the foot. Vascular sparing to the talus should be considered when selecting an appropriate operative approach for triple arthrodesis. Although clinical significance of this cadaver study is limited, the 2-incision approach appeared to cause less vascular disruption to the talar body while allowing more complete joint preparation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.