
Abstract
Background:
Among the various operative treatments of Morton’s neuroma, deep transverse metatarsal ligament (DTML) release has been performed for decompression of neuroma. However, the main lesion of Morton’s neuroma is located between the metatarsal head and the metatarsophalangeal (MTP) joint and more distal than the DTML. Hence we performed the metatarsal shortening osteotomy along with DTML release for decompression of neuroma, and investigated the clinical outcomes of it and compared the outcomes with those of DTML release alone.
Methods:
We retrospectively reviewed 84 consecutive patients (86 neuromas) who underwent surgery for a Morton’s neuroma between February 2008 and March 2011. The first 46 neuroma (group A) were treated with DTML release alone, and the next 40 neuroma (group B) underwent the metatarsal shortening osteotomy with DTML release. Clinical outcomes were compared between the groups and the associations between clinical outcomes and neuroma size were assessed.
Results:
Clinical outcomes were significantly improved after surgery in both groups but there were significant differences in clinical outcomes between the 2 groups at final follow-up. There were significant correlations between neuroma size and outcomes in group A, whereas no significant correlations were found between neuroma size and outcomes in group B.
Conclusion:
The metatarsal shortening osteotomy with DTML release resulted in better outcomes compared with DTML release alone in patients with Morton’s neuromas.
Level of Evidence:
Level III, retrospective comparative series.
Morton’s neuroma is a compressive neuropathy of an interdigital nerve between metatarsal heads and is more prevalent among adult women, with the most likely time of onset being in the fifth decade of life. Gauthier 8 first observed that Morton’s neuroma was a nerve entrapment syndrome in which the nerve was compressed between the plantar soft tissue and the anterior edge of the deep transverse metatarsal ligament (DTML), which is thick and rigid at the level of the metatarsal heads. As a result of this entrapment, the nerve enlarges and progressively becomes a pseudoneuroma wrapped in inflammatory tissue. 21
Various operative treatments have been reported for Morton’s neuroma.1,2,15,21,22,24 Among these, 1 of the most common approaches has been a decompression of neuroma by release of the DTML. However, according to an anatomical study by Kim et al, 13 the main lesion of Morton’s neuroma is located between the metatarsal head and the metatarsophalangeal (MTP) joint and more distal than the DTML, thus questioning the suggestions of previous studies that compression by the DTML is the major causative factor in the development of Morton’s neuroma. We hypothesized that metatarsal shortening osteotomy would be an effective treatment for the decompression of a Morton’s neuroma located between the metatarsal head and the MTP joint. The aims of this study were to investigate the clinical outcomes of the metatarsal shortening osteotomy along with the release of the DTML for intermetatarsal decompression, to compare the outcomes thereof with those of DTML release alone, and to assess the associations between clinical outcomes and neuroma size.
Methods
We retrospectively reviewed 84 consecutive patients (86 feet, 86 neuromas) who underwent surgery for a Morton’s neuroma between February 2008 and March 2011. The first 46 neuroma (group A) were treated with the release of DTML alone from February 2008 to June 2009, and the next 40 neuroma (group B) underwent treatment with the metatarsal shortening osteotomy along with DTML release between July 2009 and March 2011. All patients had been managed with various conservative treatments such as shoe-wear modification, use of orthotic devices, administration of nonsteroidal antiinflammatory medications, and corticosteroid injections into the involved intermetatarsal space before they were referred for surgery. The inclusion criteria were persistent pain, numbness, tingling sensation, and functional impairment despite a minimum of 3 months of conservative therapy. All patients underwent preoperative MRI to confirm the diagnosis, identify the intermetatarsal space affected, measure the neuroma size and rule out other pathologies. To avoid potential bias, an independent observer who was a musculoskeletal trained radiologist, not involved in the care of the patients and blinded to the intention of this study, evaluated the MRI films. Patients with a history of previous surgery for neuromas, MTP joint pathologies including arthritis, synovitis, dislocation, Freiberg’s infraction, or other associated foot disorders including hallux valgus, hallux rigidus, and lesser toe abnormalities were excluded. The study protocol was approved by our ethics committee, and all patients provided written informed consent.
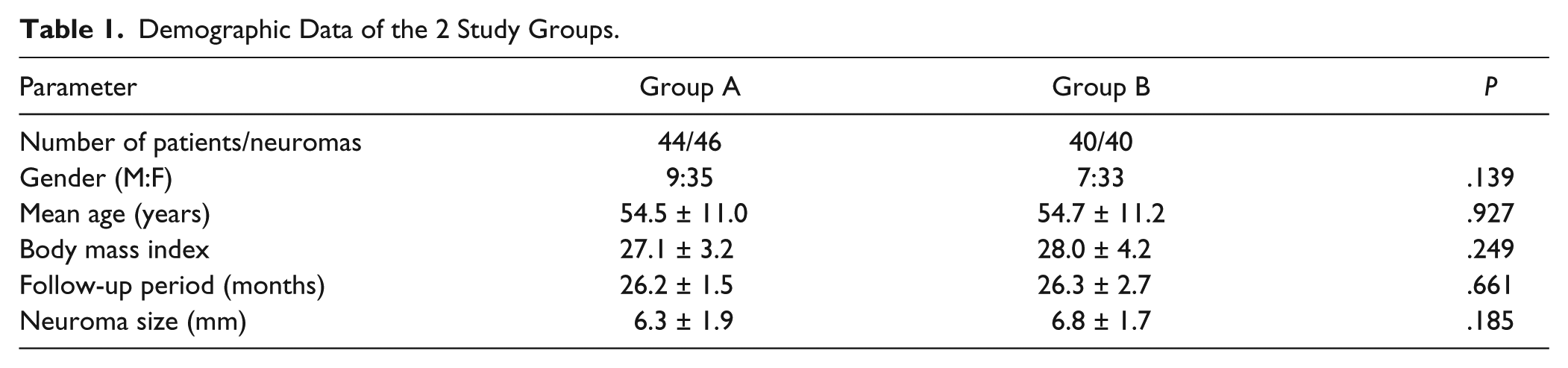
The study included 68 women and 16 men whose average age at the time of surgery was 54.5 years (range, 35-67 years). Among a total of 86 neuromas, 41 occurred in the right foot, 43 occurred in the left foot, and 2 patients had lesions in both feet. Nine neuromas involved the second intermetatarsal space and 77 the third intermetatarsal space. All neuromas were visible on MRI. The mean size of neuromas on MRI was 6.6 ± 1.8 mm (range, 3.9-11.2 mm). The mean duration of follow-up was 26.3 months (range, 24-35 months). There were no significant differences in basic characteristics between the 2 groups regarding patient sex, age, body mass index, follow-up period, and neuroma size (Table 1).
Demographic Data of the 2 Study Groups.
During the preoperative examination, we obtained anteroposterior weight-bearing radiographs to measure the metatarsal lengths of lesser toes following the guidelines of Maestro et al 14 (Figure 1). The osteotomy was planned for the longer of the metatarsal bones adjacent to the neuroma to maintain the metatarsal parabola to the maximum extent possible.
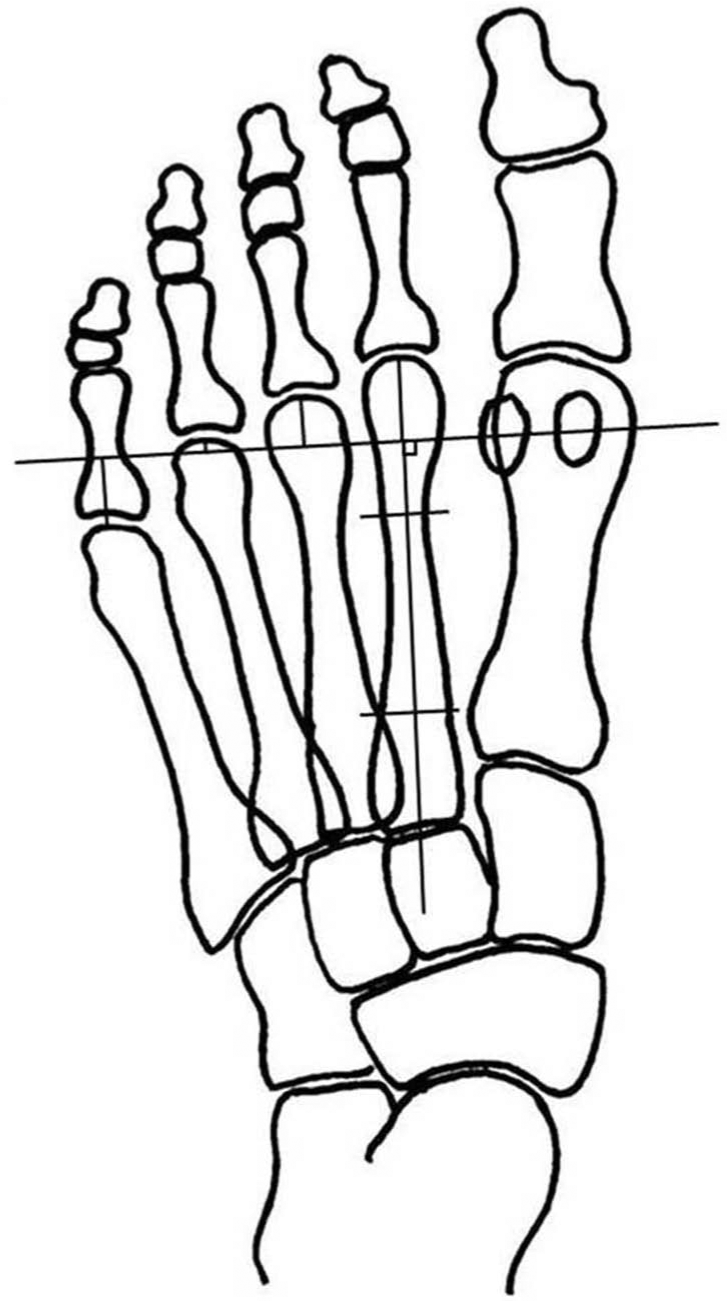
Method for the measurement of metatarsal lengths of lesser toes. Metatarsal lengths were determined by measuring the distances from apex of each metatarsal to transmetatarsal line centered from lateral sesamoid and perpendicular to the second metatarsal axis.
Operative Technique
Patients were placed in the supine position, and surgery was performed under spinal anesthesia. A dorsal, 3-cm longitudinal incision was made over the involved interspace. After careful dissection for identifying the DTML and the interdigital nerve, a curved elevator was passed underneath the ligament, and the ligament was released while visualizing the interdigital nerve (Figure 2).

Photograph showing the Morton’s neuroma (N) after release of the deep transverse metatarsal ligament (DTML; dotted lines). The neuroma was located between the metatarsal head and the metatarsophalangeal joint and more distal than the DTML.
For the metatarsal shortening osteotomy, the joint capsule was then incised, and the metatarsal shortening osteotomy was performed in a horizontal plane parallel to the foot once protection of soft tissue was ensured while keeping the toes in plantarflexion. The osteotomy was performed starting at the dorsal base of the head approximately 3 mm from the articular cartilage. Once the osteotomy was finished, we displaced the head proximally based on measurements obtained during the planning stage. The osteotomy was stabilized using a single screw (Spin Screw; Integra LifeScience Co., Plainsboro, NJ, USA) with a low profile head and nonthreaded lag from the dorsal to the plantar direction and perpendicular to the plane of the osteotomy. The resulting dorsal protuberance was resected. After the osteotomy with DTML release, decompression of neuroma was achieved by widening of the intermetatarsal space (Figure 3).

Preoperative and postoperative radiographs. After the metatarsal shortening osteotomy with the release of the deep transverse metatarsal ligament, decompression of Morton’s neuroma was achieved by widening of the third intermetatarsal space.
Postoperatively, patients were allowed to bear weight on their heel as tolerated in an open, hard-soled operative shoe for 4 weeks in both groups. Upon radiographic evidence of healing at the osteotomy site, usually 4 weeks later, transfer of weight to the forefoot in a regular shoe was permitted.
Clinical Outcome Evaluations
For clinical evaluation, the Foot Function Index (FFI) score and the subscales of FFI including foot pain, disability and activity limitation were utilized. The American Orthopaedic Foot and Ankle Society (AOFAS) forefoot score was also used for clinical evaluation. Furthermore, patients rated their overall satisfaction with the operation as excellent, good, fair, or poor and were asked whether they would undergo the procedure again under similar circumstances.
Statistical Analysis
The Wilcoxon signed-rank test was conducted to evaluate changes in preoperative and final follow-up values and the Mann–Whitney U test was performed for the comparison of outcomes between groups A and B. All clinical values were reported as mean ± standard deviation. To analyze the association of clinical outcomes and the sizes of the neuromas, we used stepwise multivariate linear regression to assess the correlation between neuroma size and final follow-up clinical outcomes in each group. We used SPSS (version 15.0; SPSS Inc, Chicago, IL, USA) for all analyses, and statistical significance was accepted for P values of less than .05.
Results
Clinical Outcomes
Clinical outcomes including the FFI score and AOFAS score were significantly improved after surgery in both groups (P < .05, respectively). There were significant differences in mean FFI score and AOFAS score between the 2 groups at final follow-up (P < .05, respectively; Table 2).
Comparison of Clinical Outcomes Between the 2 Study Groups.
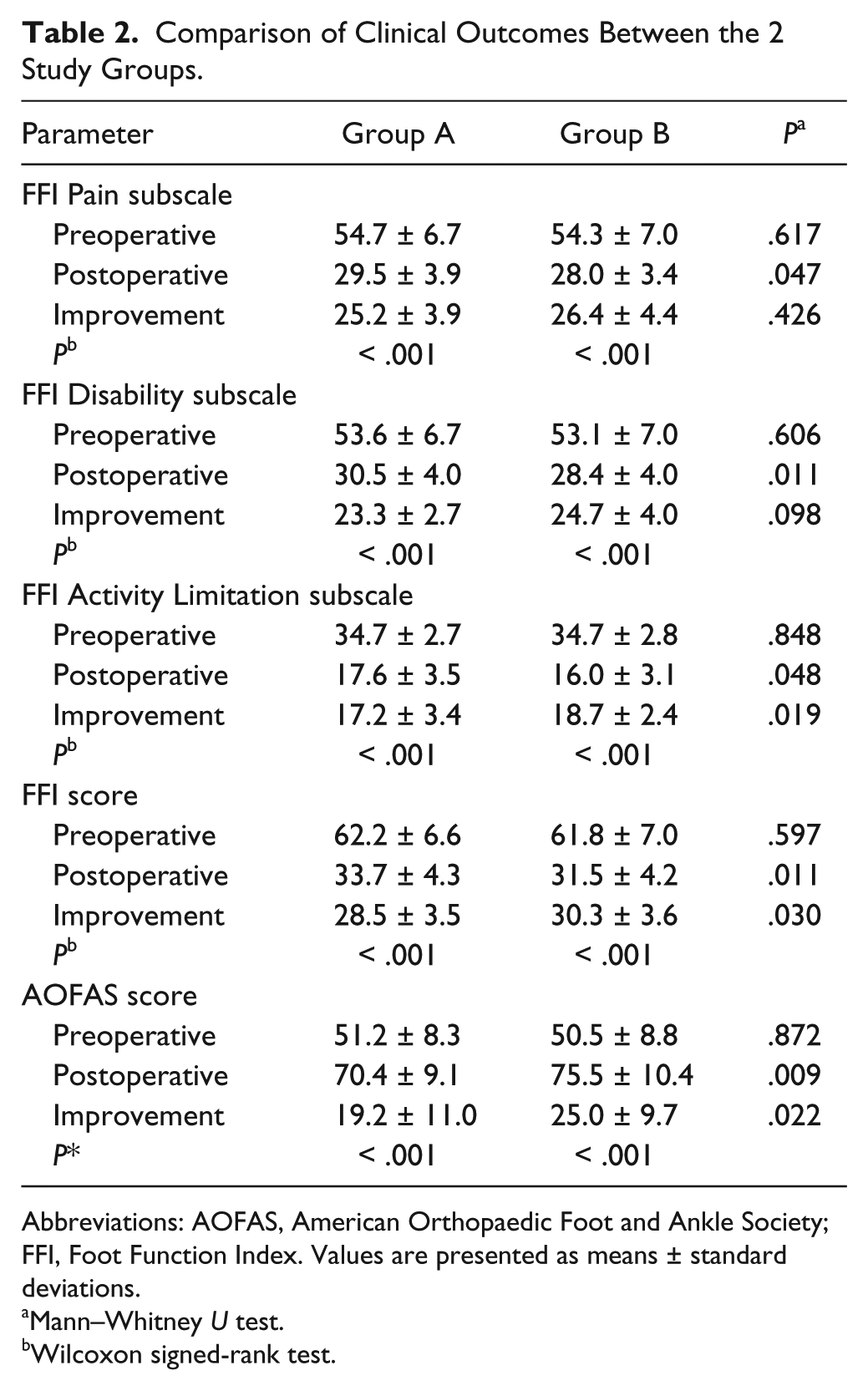
Abbreviations: AOFAS, American Orthopaedic Foot and Ankle Society; FFI, Foot Function Index. Values are presented as means ± standard deviations.
Mann–Whitney U test.
Wilcoxon signed-rank test.
The mean neuroma size was 6.3 ± 1.9 mm in group A and 6.8 ± 1.7 mm in group B (P = .185). In multivariate analysis, for the final follow-up FFI score, the neuroma size accounted for 52.3% of the variability in group A and 4.9% in group B. For the final follow-up AOFAS score, the defect size accounted for 51.4% of the variability in group A and 5.6% in group B (Figure 4). As illustrated in the scatter plot, patients with a neuroma size larger than 6.6 mm (median value) had significantly worse outcomes according to the final follow-up FFI score and AOFAS score than patients with a neuroma size smaller than 6.6 mm in group A (P < .001, respectively). When considering the results of final follow-up FFI score and AOFAS score, neuroma size was an independent predictor of clinical outcomes of the release of DTML. However, neuroma size did not independently predict the clinical outcomes of the metatarsal shortening osteotomy along with the release of DTML (P = .171 for FFI score and P = .141 for AOFAS score).
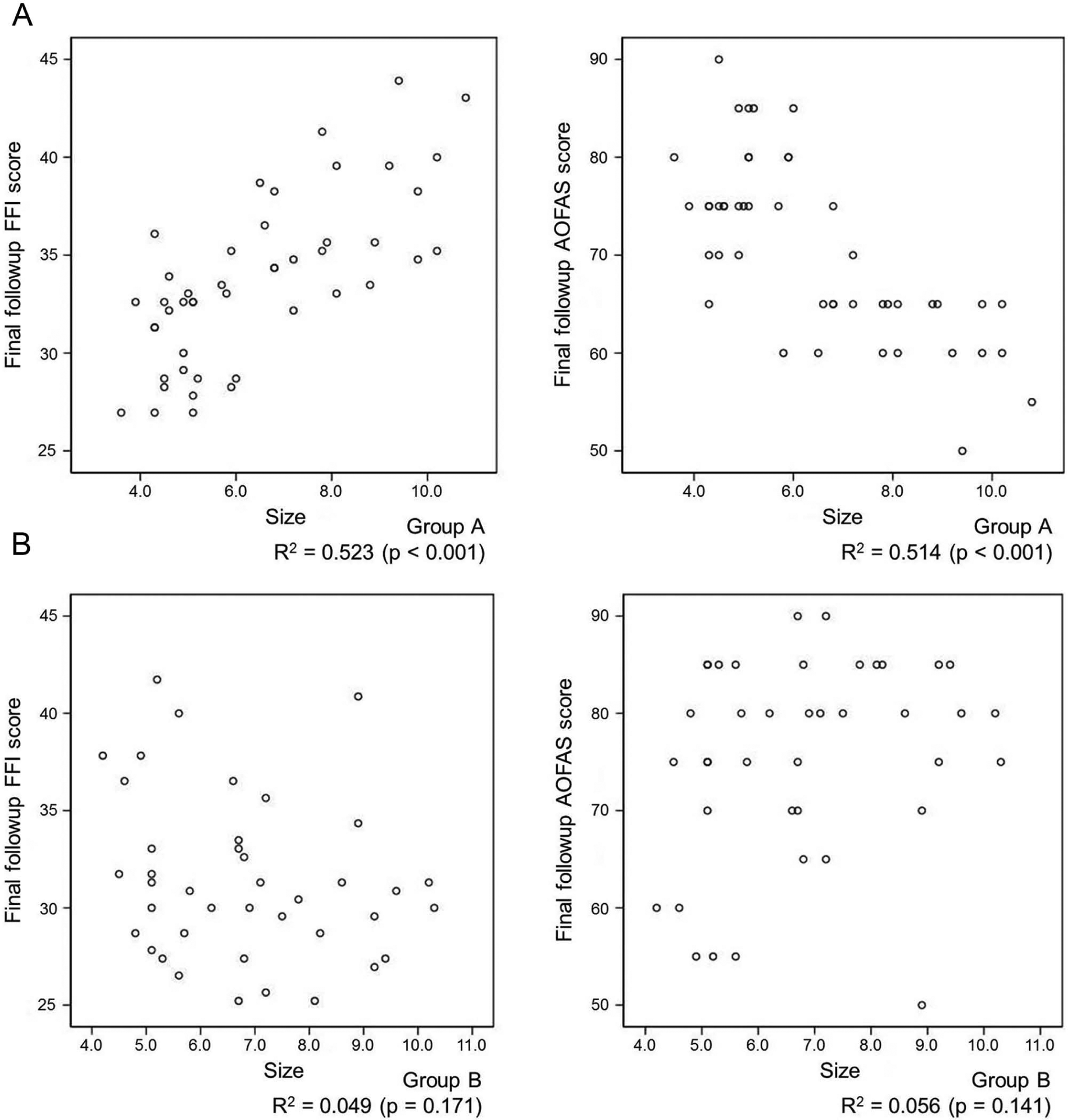
Scatter plots show the correlations between neuroma size and final follow-up clinical outcomes including Foot Function Index (FFI) score and American Orthopaedic Foot and Ankle Society (AOFAS) score in both groups. (A) Good correlations are found between neuroma size and final follow-up clinical outcomes in group A. (B) There are no significant correlations between neuroma size and final follow-up clinical outcomes in group B.
Regarding overall patient satisfaction with the operation, 20 patients reported their satisfaction as excellent (45%), 17 good (39%), 5 fair (11%), and 2 poor (5%) in group A and 25 excellent (63%), 13 good (33%), and 2 fair (5%) in group B. Two patients with poor satisfaction in group A underwent additional neuroma excisions for involved neuromas at 8 and 10 months after the initial surgery, respectively. In group B, none of the patients reported poor satisfaction with the operation and all 40 patients stated that they would be willing to undergo the same operation for their 40 neuroma again.
Complications
Three patients of group A and 2 of group B developed superficial wound infections, which were treated successfully with antibiotics. In group B, there were no other complications such as sensory loss of affected toes, avascular necrosis of metatarsal heads, nonunion of the osteotomy site, or painful plantar keratosis. Four patients had asymptomatic floating toes, and 2 patients had mild stiffness of the MTP joints following the operation. However, floating toes or stiff MTP joints did not appear to affect the function of the feet significantly during the follow-up periods.
Discussion
Various operative treatments for Morton’s neuromas have been reported.1,17,21,22,24 Although excision of neuroma is still the most common operative approach to Morton’s neuroma, several complications have been reported by many authors. Johnson et al 11 have reported persistent symptoms because of inadequate initial resection of the nerve, and Coughlin and Pinsonneault 5 have pointed out that after excision, a stump neuroma may occasionally arise and can be painful in the weight-bearing area. Excision also leads to sensory loss in the affected toes and dysesthesia in the area of the dorsal cutaneous nerve territory.2,9 Morton’s neuroma is not a true neuroma, rather it is a pseudoneuroma wrapped in inflammatory tissue resulting from entrapment. 21 Therefore, features associated with the lesion include perineural fibrosis, local vascular proliferation, edema of the endoneurium, and axonal degeneration. Because of these findings, in the present study, we hypothesized that excision of neuroma is not a proper method for treating Morton’s neuroma.
Alternative treatments such as decompression of the interdigital nerve using endoscopic and minimally invasive techniques have been reported in recent years,17,24 and open decompression of the nerve by releasing the DTML has also been described.6,21 However, in their anatomical study, Kim et al 13 reported that if Morton’s neuroma occurs because of increased pressure and irritation of surrounding structures, then the location of compression would cause the lesion to be more distal than the DTML. They suggested that Morton’s neuroma is caused by pinching of the interdigital nerve by the adjacent metatarsal heads and the MTP joint during walking. This indicates that the MTP joint is a more important landmark for treatment of the lesion than the more commonly approached DTML and implies that decompression of neuroma by releasing the DTML is insufficient to decompress the intermetatarsal space. Therefore, we performed the metatarsal shortening osteotomies for the decompression of Morton’s neuromas located between the metatarsal head and the MTP joint (Figure 2).
The metatarsal shortening osteotomy is usually used to adjust the length of the metatarsals in patients with metatarsalgia, intractable plantar keratosis, or MTP joint dislocation.10,12,20 It can provide controlled shortening of the lesser metatarsals. In the ideal anatomical configuration of the metatarsal curve (metatarsal parabola), the optimal length of the metatarsals decreases laterally from the second metatarsal in geometric progression, as described by Maestro et al. 14 This provides an equal transference of pressure across the forefoot from midstance through to toe-off.3,7 Several biomechanical studies have shown that the metatarsal shortening osteotomy produces the expected metatarsal shortening, which is often accompanied by plantar placement of the metatarsal head.12,19 In this respect, we thought that as the metatarsal head is moved proximally and to a plantar aspect relative to the original site, both longitudinal and axial decompressions of the intermetatarsal space can be achieved. However, the comparative metatarsal length discrepancy may cause complications including postoperative extension contractures as well as floating and stiff toes. 10 Therefore, a harmonized shortening of the metatarsals is crucial during the osteotomy, and our efforts to maintain the metatarsal parabola included preoperative planning, as mentioned. We cannot define the exact association between postoperative complications and the degree of metatarsal shortening, but there were no severe complications such as plantar metatarsalgia, painful plantar keratosis, symptomatic floating toes, or severe stiffness of the MTP joints after the osteotomy in our study. For more accurate quantification of this association, an evaluation of preoperative and postoperative plantar peak pressures under the metatarsal heads could be performed using the dynamic pedobarography and power analysis should be needed.
A few studies have examined association of neuroma size with clinical symptoms or operative outcomes in Morton’s neuroma. Zanetti et al 23 and Redd et al 16 indicated strong correlation between lesion size larger than 5 mm and the presence of symptoms, whereas Sharp et al 18 reported that the neuroma size did not correlate with either the presenting symptoms or the change in symptoms after surgery. Biasca et al 4 reported that lesions smaller than 5 mm but producing symptoms such as metatarsalgia were treated successfully with neurolysis and division of the intermetatarsal ligament, whereas larger lesions were treated with excision. In our study, we found significant correlation between neuroma size and final follow-up clinical outcomes in group A (Figure 4A), which indicated that release of DTML is insufficient to decompress the neuroma in larger lesions. However, neuroma size did not influence final follow-up clinical outcomes in group B (Figure 4B). Accordingly, we discerned that the metatarsal shortening osteotomy along with the release of DTML had an influence on the better outcomes of treatment in patients with larger neuroma.
The present study had some limitations. First, the number of patients was relatively small, and data were collected retrospectively. For more accurate evaluation of the effect of the metatarsal shortening osteotomy in Morton’s neuroma, a prospective study with a larger series of cases is required. Second, the follow-up period was short. Although the short-term follow-up outcomes of this study were satisfactory and there were no severe complications immediately after the osteotomy, the long-term outcomes remain unknown, and the influence of the changed metatarsal parabolas cannot be predicted. Third, we cannot define the exact association between the amount of metatarsal shortening and the effectiveness of decompression of neuroma. In this study, the widening of intermetatarsal space could be achieved by the metatarsal shortening osteotomy, but we cannot quantify the amount of metatarsal shortening to obtain the effect of decompression of neuroma, within maintaining the metatarsal parabola. Cadaveric study is required to understand the impact of a metatarsal shortening osteotomy on the effectiveness of intermetatarsal widening. Fourth, we performed the metatarsal shortening osteotomy with DTML release. Additional studies are required for evaluating the effect of the metatarsal shortening osteotomy alone, distinguishing it from the effect of DTML release. Last, because we did not excise the neuromas, no histological diagnostic confirmation was available, making it impossible to estimate the sensitivity, specificity, and positive and negative predictive values of MRI from the data available. Furthermore, as the neuroma size was measured only by MRI, the actual association of clinical outcomes with neuroma size may have been affected.
In conclusion, this study showed encouraging results for the metatarsal shortening osteotomy with DTML release compared with DTML release alone in Morton’s neuroma. Furthermore, the metatarsal shortening osteotomy with DTML release influenced better outcomes of treatment in patients with larger neuromas. Although still in the early stages of application, the metatarsal shortening osteotomy was effective in relieving pain from Morton’s neuroma.
Footnotes
Editor’s Note
The authors are to be congratulated for a new method with an anatomic theory for its effectiveness. It was somewhat surprising that they did not have any symptomatic plantar keratosis after an isolated metatarsal osteotomy in this patient population. I would certainly encourage them to evaluate subsequent patients with pre- and postoperative pedobarographic studies to assess the magnitude of change in the plantar pressures. Also, I would encourage them to compare a group of patients with nerve excision, which is still the most commonly performed operative treatment today in most centers, to their DTML release and metatarsal osteotomy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.