
Abstract
Background:
Recently, arthroscopic-assisted techniques have been described to treat lateral ankle instability with excellent results. However, complications including neuritis of the superficial peroneal or sural nerve, and pain or discomfort due to a prominent anchor or suture knot have been reported. The aim of this study was to describe a novel technique, the “all-inside arthroscopic lateral collateral ankle ligament repair,” and its results for treating patients with ankle instability.
Methods:
Sixteen patients (10 men and 6 women, mean age 29.3 years, 17-46) with lateral ankle instability were treated with an arthroscopic procedure. Using a suture passer and a knotless anchor, the ligaments were repaired with an all-inside technique. The right ankle was affected in 10 cases. Mean follow-up was 22.3 (12-35) months.
Results:
On arthroscopic examination, 13 patients had an isolated anterior talofibular ligament (ATFL) injury, and in 3 patients, both the ATFL and calcaneofibular ligament (CFL) were affected. All-inside arthroscopic anatomic repair of the lateral collateral ligament complex was performed in all cases. All patients reported subjective improvement of their ankle instability. The mean AOFAS score increased from 67 preoperatively to 97 at final follow-up. No major complications were reported.
Conclusion:
The all-inside arthroscopic ligament repair was a safe, reliable, and reproducible technique that both provided an anatomic repair of the lateral collateral ligament complex and restored ankle stability while preserving all the advantages of an arthroscopic technique.
Level of Evidence:
Level IV, retrospective case series.
The most common mechanism of injury in lateral ankle sprains occurs with excessive plantarflexion and inversion of the ankle. The most commonly injured ligament is the anterior talofibular ligament (ATFL), followed by the calcaneofibular ligament (CFL). Most patients with acute ankle sprains can be successfully managed with conservative treatment, such as bracing and physical therapy. However, approximately 15% to 20% of patients will remain symptomatic, with the most commonly described complaints being ankle weakness, giving-way, pain, and, occasionally, stiffness. 11
If residual instability is still present after a solid course of nonoperative treatment, the patient should be presented with surgical options to restore ankle stability. 25 Several surgical techniques have been described for the treatment of chronic lateral ankle instability. They can be divided into anatomic repair, nonanatomic reconstruction, and anatomic reconstruction.
The anatomic repair technique is generally preferred over reconstruction procedures.2,16,22,29,30 Numerous studies have shown good to excellent results with anatomic repairs, with over 85% of patients achieving good outcomes.4,19,29,39 The long-term success of anatomic repairs is well established. Bell and colleagues 4 followed 22 patients who underwent a Brostrom technique type of repair for 26 years and reported over 90% good to excellent results. Patients with long-standing instability, poor tissue quality, history of a previous repair, generalized ligamentous laxity, and cavovarus foot deformity have been reported to have poor result with anatomic repairs. For this group of patients the nonanatomic and anatomic reconstructive procedures are options to consider.
Recently, some authors have developed arthroscopic-assisted suture anchor techniques to repair the lateral collateral ankle ligaments with excellent results.1,8,27,34 However, neurological complications or prominent implants have been described as some of the associated complications.
We present an all-inside arthroscopic repair of the lateral collateral ankle ligament complex with a knotless suture anchor technique that resulted in an anatomic repair and ankle stability while still preserving all the advantages of an arthroscopic technique.
Methods
In the period of 2010 to 2012, 16 consecutive patients (10 men and 6 women, mean age 29.3 years, range 17-46 years) with lateral ankle instability were treated with an arthroscopic approach. The right ankle was affected in 10 cases. Mean follow-up was 22.3 months (range, 12-35 months).
All patients had sustained an inversion injury of the ankle during sports activity. Patients reported pain laterally and an instability sensation of the ankle during activity. None of the patients had undergone previous foot or ankle surgery or had suffered a foot or ankle fracture. Physical examination showed no foot deformity. We palpated and tested around the lateral malleolus of the ankle for swelling and tenderness. Range of motion, anterior drawer test and talar tilt were examined clinically before and after surgery. We compared the injured and the contralateral side. We considered a hard stop on the anterior drawer test or talar tilt as normal, and the presence of a soft stop, a nonstop, or a sulcus sign in the anterolateral area of the ankle as pathological. The anterior drawer test and talar tilt findings were positive in all ankles. No hypermobility or deficit of flexion-extension of the ankle were observed compared to the contralateral side.
No medial instability was observed. Two of the patients reported discomfort and “click” sensation of the peroneal tendons, but no peroneal tendon subluxation was reproduced during the examination. Patient assessment with the American Orthopaedic Foot and Ankle Society (AOFAS) clinical rating scale was carried out before and after the procedure.
Routine radiographs showed no abnormalities. Preoperative magnetic resonance imaging (MRI) of the ankle was performed in all cases to obtain a complete imaging study. MRI examination showed chronic injury of the ATFL in all cases, and osteochondral injury located in the medial area of the talus in 2 patients. Ankle arthroscopy was performed in all the patients in a standard manner. The arthroscopic procedure lasted a mean of 36 (range, 22 to 55) minutes.
Operative Technique
A suture passer (Microsuture lasso curved 70 degrees, Arthrex, Naples, FL), a 2:0 or 0 nonabsorbable suture (Fiberwire, Arthrex, Naples, FL), and a knotless anchor (Pushlock 2.9 mm × 15 mm, Arthrex, Naples, FL) were used for ligament repair.
Spinal anesthesia was used. The patient was placed in supine position with the affected extremity on a thigh holder located under the knee. Both the hip and the knee were flexed approximately 45 degrees, allowing the leg to be placed parallel to the floor. A thigh tourniquet was used.
The following landmarks were marked: the anterior joint line, which is easily palpated by moving the joint through plantar and dorsiflexion; the anterior tibialis tendon; the peroneus tertius tendon which is present in 90% of cases (in its absence, the extensor digitorum longus tendon will be found); the lateral malleolus; and the superficial peroneal nerve (Figure 1). Clinical examination maneuvers to identify the nerve were performed systematically12,38: the nerve moves with ankle motion, 9 and its subcutaneous course becomes evident with inversion of the ankle and plantarflexion of the fourth toe (Figure 2).
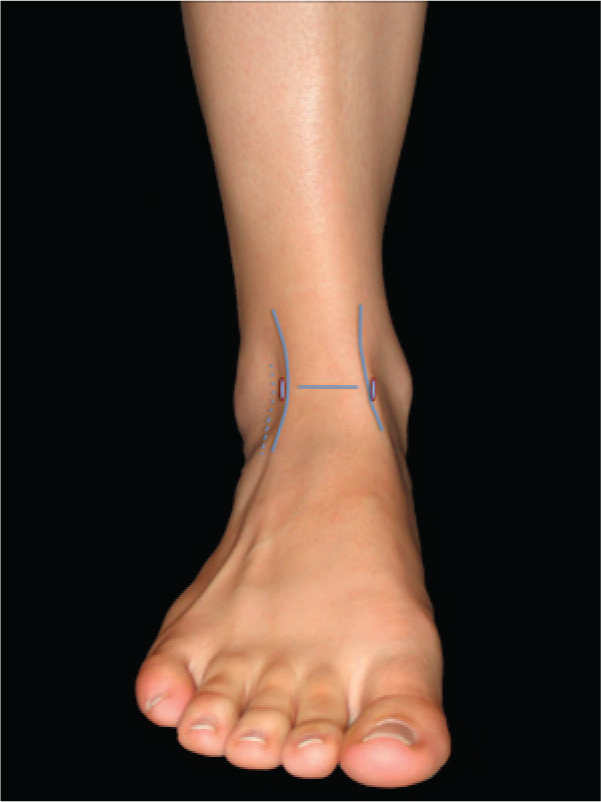
Anatomical landmarks of the anterior aspect of the ankle, and anterior portals for the ankle arthroscopy.
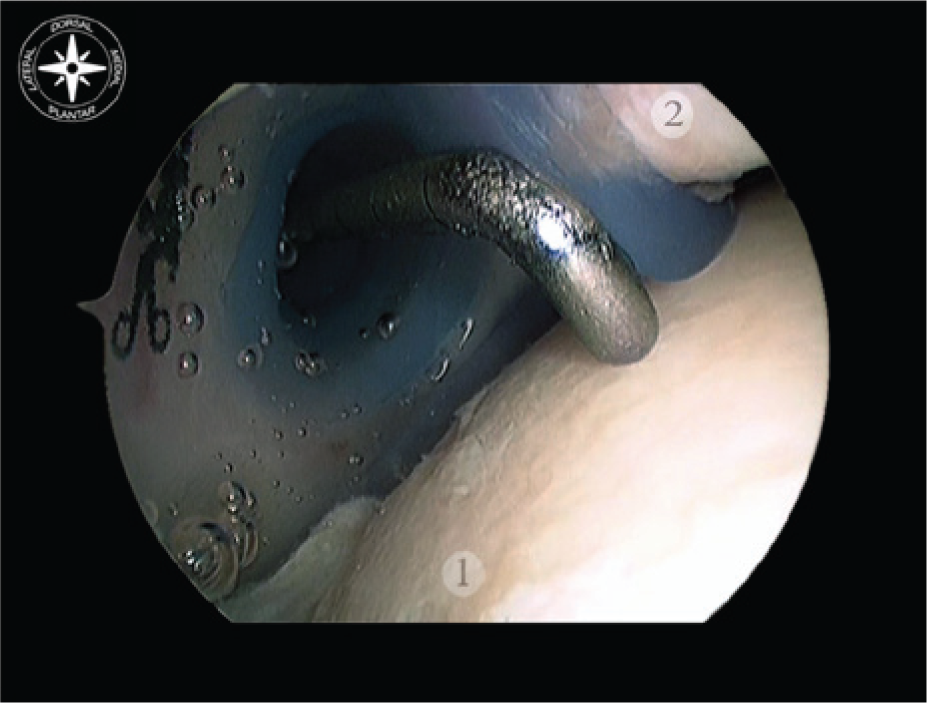
Cannula introduced in the anterolateral portal to avoid peroneal superficial nerve injuries during procedure. Probe introduced through the cannula. (1) Talus. (2) Anterior and distal portion of the tibia.
Distraction of the ankle was not used during the arthroscopic procedure. The anterior capsular insertion into the tibia and talus occurs at a distance from the cartilaginous surface. This anatomic feature creates a potential anterior working space when the ankle is in dorsiflexion. 17 Dorsiflexion of the ankle without distraction allows good visualisation and easy access to the lateral and medial recesses of the ankle. 41 The all-inside arthroscopic technique for lateral collateral ligament repair requires creation of 3 portals. An accessory anterolateral portal was performed during the procedure. This accessory portal was created just anterior to the fibula, at 0.5-1 cm proximal from the tip of the lateral malleolus (Figure 3).
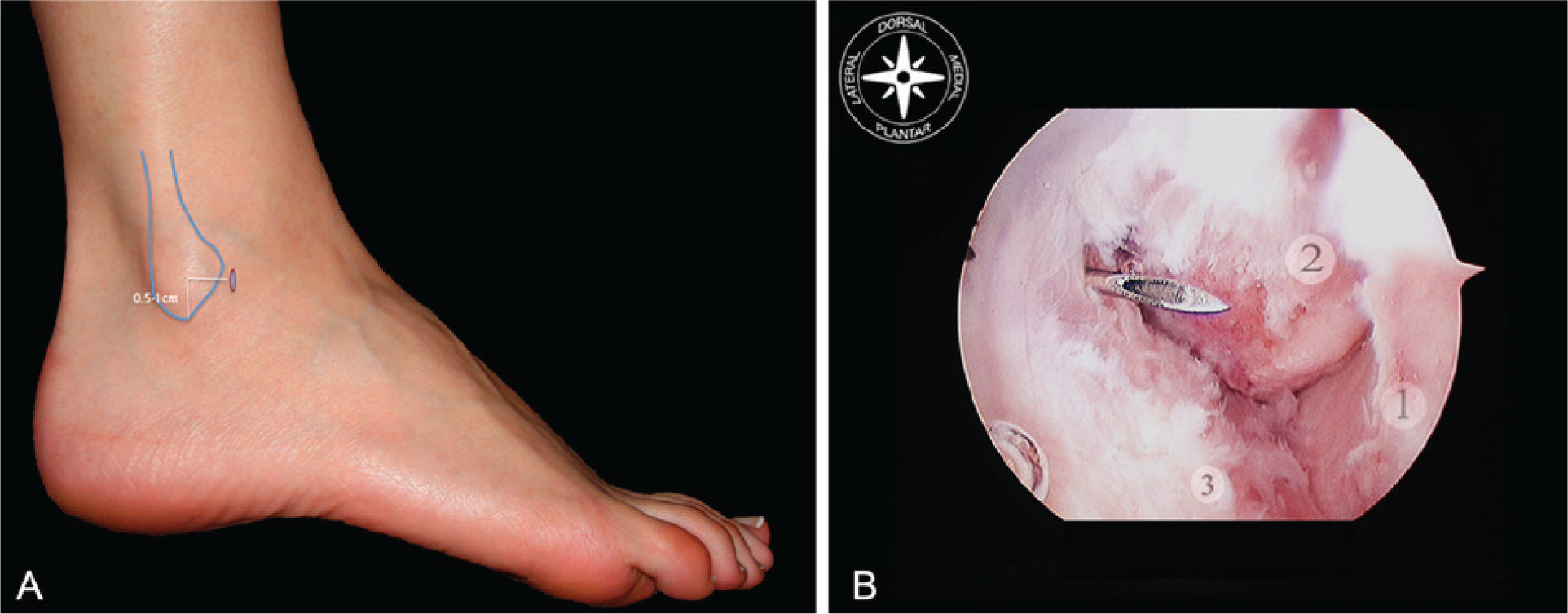
Location of the accessory anterolateral portal. (A) Lateral view of the foot and ankle. The accessory portal is created just anterior to the fibula, at 0.5-1 cm proximal from the tip of the lateral malleolus. (B) Arthroscopic view in a right ankle of the needle introduced through the accessory anterolateral portal. (1) Talus. (2) Lateral malleolus. (3) Anterior talofibular ligament desinserted from its fibular origin.
After a full arthroscopic exploration, the lateral collateral ligaments were repaired under direct arthroscopic view. Any other arthroscopic procedure, such as chondral debridement and microfracturing, should be performed before the ligament repair (Figure 4).
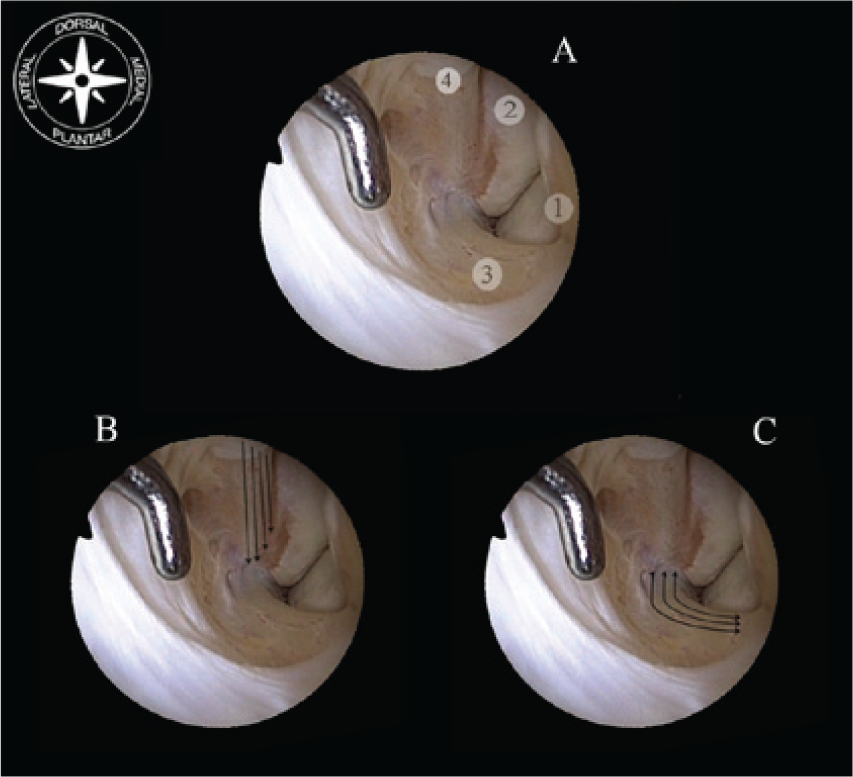
Arthroscopic view of the lateral gutter in a right ankle. Scope introduced through the anteromedial portal, and probe through the anterolateral portal. Ankle in dorsiflexion. (A) Anatomic structures of the lateral gutter. The anterior tibiofibular ligament reaches the origin of the superior band of the anterior talofibular ligament. (B) Arrows indicating direction of the fibers of the distal portion of the anterior tibiofibular ligament, and indicating its insertion the lateral malleolus. (C) Arrows indicating direction of the fibers of the anterior talofibular ligament, from its origin in fibula to its insertion in talus. In dorsiflexion of the ankle the ligament is relaxed. (1) Lateral wall of the talus. (2) Anterior aspect of the distal portion of the lateral malleolus. (3) Superior band of the anterior talofibular ligament. (4) Distal portion of the anterior tibiofibular ligament.
Arthroscopic criteria of ATFL injury was defined as partial or complete desinsertion of the fibular attachment with vision of the ATFL footprint. ATFL and CFL injury was defined as complete desinsertion of the fibular attachment of the ATFL, and partial or complete desinsertion of the fibular attachment of the CFL, with vision of the corresponding footprint areas or of a denudated fibular tip.
The footprint for the fibular attachment of the lateral collateral ligaments was debrided with a shaver introduced through the anterolateral portal (Figure 5). The suture passer was introduced through the anterolateral portal, and under direct arthroscopic visualization, the ligament was penetrated from lateral to medial. Then, the Nitinol loop wire was pulled out through the accessory anterolateral portal with the help of an arthroscopic grasper (Figure 6). The suture was placed through the loop, and pulled back. Although a simple suture could be passed, we recommend passing a double suture through the ligament to avoid tearing the ligament when the suture is tensioned. The suture ran from the accessory portal through the ligament to the anterolateral portal. In case of a double suture technique, 2 limbs of the suture were located in the accessory portal while the loop of the suture was in the anterolateral portal. The limbs of the suture located in the accessory portal were passed through the anterolateral portal. An arthroscopic grasper was helpful for this suture passage. Next, the limbs of the suture were passed through the loop suture. By pulling the suture limbs, the loop was introduced into the joint and the ligament was grasped by the suture (Figure 7). The location for the suture anchor was identified on the distal portion of the lateral malleolus along its anterior aspect and about 1.5 cm proximal to the fibula tip for the ATFL.
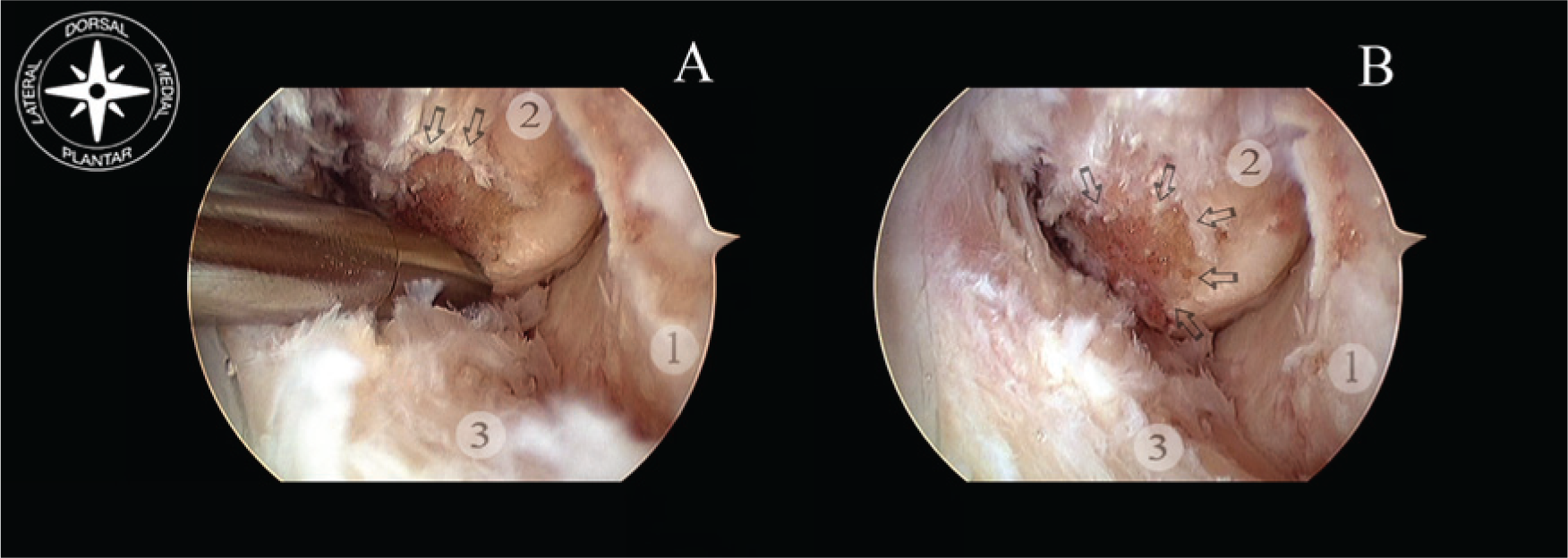
Arthroscopic view of the lateral gutter in a right ankle. Scope introduced through the anteromedial portal. Ankle in dorsiflexion. (A) The footprint for the fibular attachment of the anterior talofibular ligament is debrided with a shaver introduced through the anterolateral portal. Arrows indicating fibular insertion of the distal portion of the anterior tibiofibular ligament. (B) Fibular footprint of the anterior talofibular ligament is indicated with arrows. (1) Lateral wall of the talus. (2) Anterior aspect of the distal portion of the lateral malleolus. (3) Anterior talofibular ligament desinserted from its fibular origin.
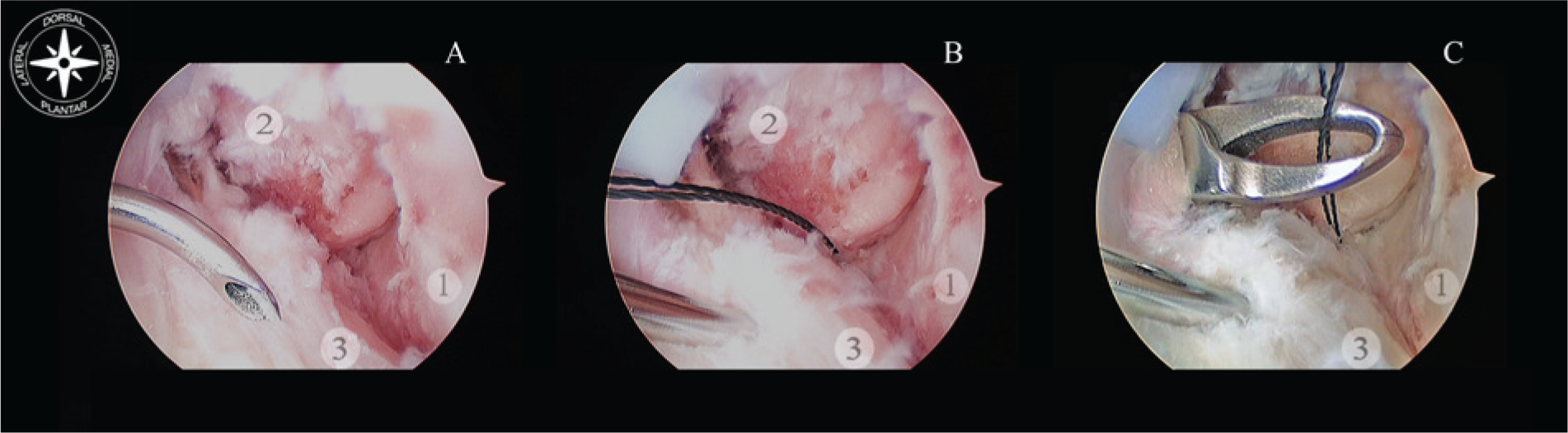
Grasping the ligament with a suture is the first step for the all-inside arthroscopic ankle ligament repair with a knotless suture anchor. (A) The suture passer is introduced through the anterolateral portal and the ligament is penetrated from lateral to medial. (B) The Nitinol loop wire is pulled. (C) With the help of an arthroscopic grasper introduced through the accessory lateral portal, the Nitinol is pulled out. (1) Lateral wall of the talus. (2) Anterior aspect of the distal portion of the lateral malleolus. (3) Anterior talofibular ligament desinserted from its fibular origin.
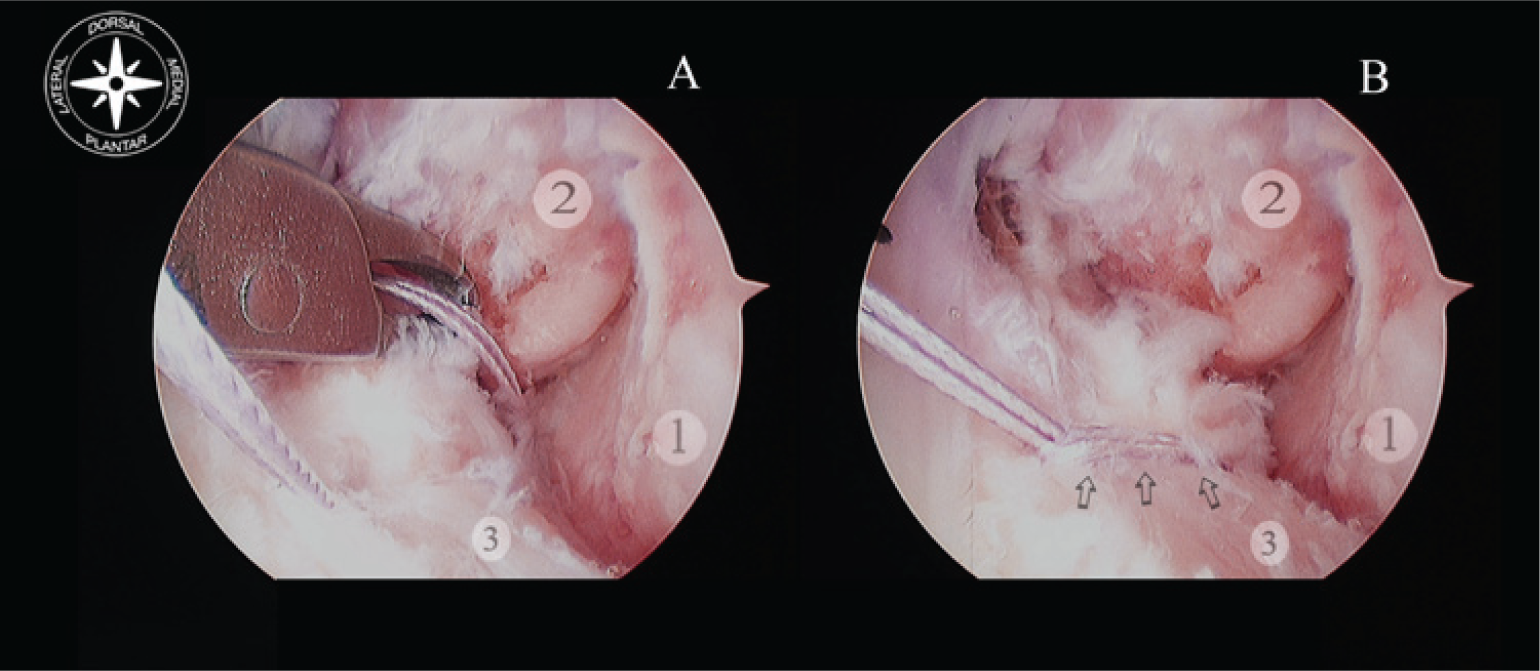
A doble suture is placed through the loop of the Nitinol, and pulled back, running from the accessory portal through the ligament to the anterolateral portal. (A) The limbs of the suture located in the accessory portal must be passed through the anterolateral portal with the help of a grasper. (B) The limbs of the suture are passed through the loop suture. Pulling the suture limbs, the loop is introduced into the joint and the ligament is grasped by the suture. Arrows indicate the suture grasping the ligament. (1) Lateral wall of the talus. (2) Anterior aspect of the distal portion of the lateral malleolus. (3) Anterior talofibular ligament desinserted from its fibular origin.
To reproduce the native insertion of the ATFL, the anchor must be located on the fibular attachment of the anterior inferior tibiofibular ligament insertion or just distal to it. The drill was directed from anterior to posterior, and parallel to the plantar plane as well as the plane of the lateral gutter (Figure 8, A and B). The hole was drilled and the bone anchor with the suture passed through the portal was introduced into the hole by impaction. Tension of the suture can be modulated before introducing the anchor. Tensioning of the suture was possible when the suture limbs passed through the eyelet of the knotless anchor. Once the anchor was introduced, the tension of suture could not be controlled. The ATFL was reattached with the ankle in dorsiflexion and valgus (Figure 9). Using the same technique as outlined above, an anchor was placed for the CFL if some insufficiency is detected. For this purpose the drill guide was introduced through the accessory portal and placed lateral and about 0.5 cm proximal to the lateral malleolus tip while aiming from distal to proximal and anterior to posterior. The CFL was reattached with the ankle in neutral position and valgus. The CFL should be repaired first if both ATFL and CFL are being repaired.
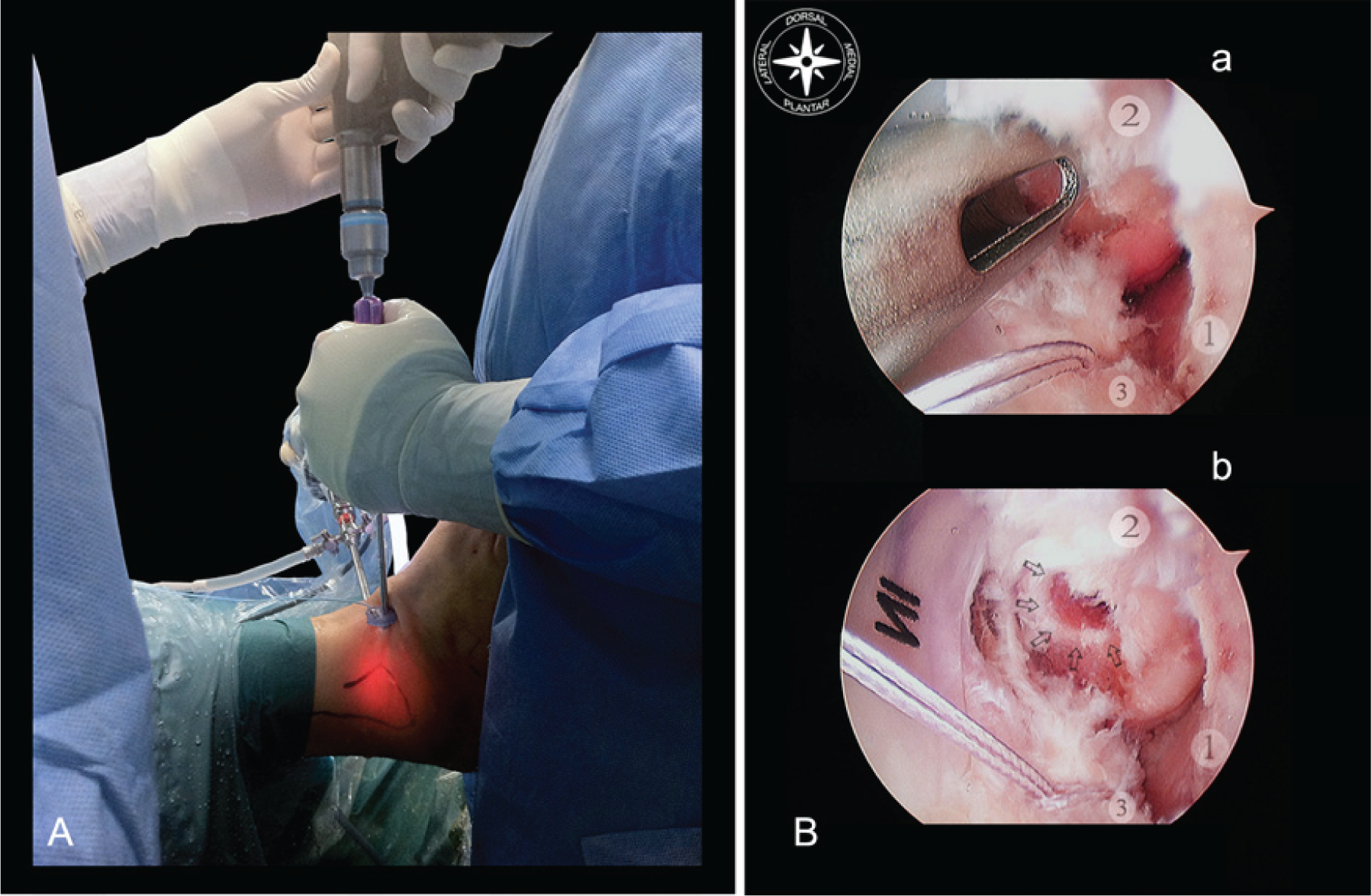
Drilling of the suture anchor. (A) External view of the position of the foot and ankle. Drill must be directed from anterior to posterior, and parallel to the plantar plane as well as the plane of the lateral gutter. (B) Arthroscopic view of the drilling. (a) The drill guide is placed through the anterolateral portal and centered just distal to the anterior inferior tibiofibular ligament fibular insertion. (b) Hole, indicated with arrows, must be recognized. (1) Lateral wall of the talus. (2) Anterior aspect of the distal portion of the lateral malleolus. (3) Anterior talofibular ligament grasped with the suture.
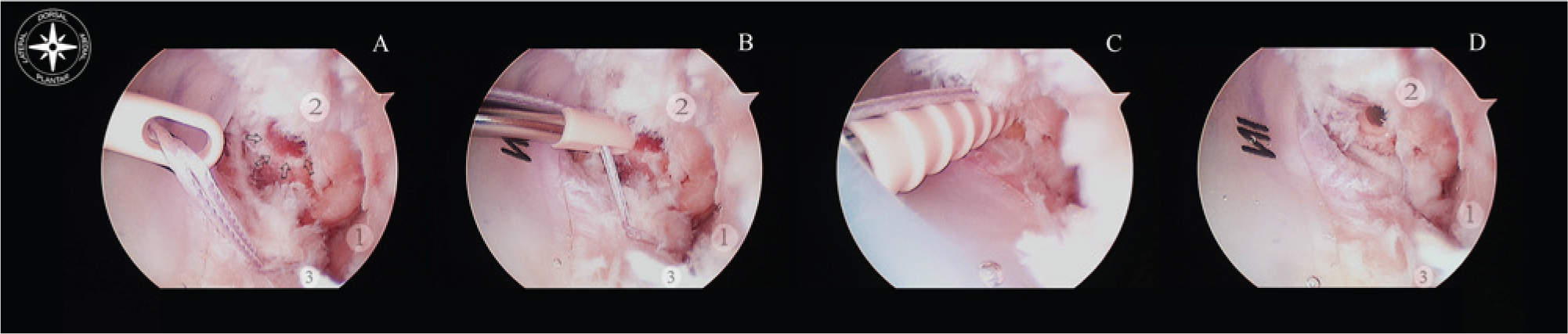
Introduction of the suture anchor. (A) The anchor with the suture passed is introduced through the anterolateral portal. Arrows indicate the hole drilled. (B) Tension of the suture can be modulated before introducing the anchor in the hole. (C) The anchor is introduced into the hole by impaction. Dorsiflexion and valgus of the ankle are necessary to reattach the ATFL. (D) The ligament is attached on its footprint. (1) Lateral wall of the talus. (2) Anterior aspect of the distal portion of the lateral malleolus. (3) Anterior talofibular ligament.
A compressive bandage and a posterior plaster splint with the ankle in neutral position were applied and maintained for 2 to 3 days. The bandage was removed at the second or third postoperative day and was switched to a removable walking boot to begin partial weight bearing with an assistive device for the first 3 weeks.
Antithrombotic prophylaxis was used for 10 to 15 days, except in those patients with chondral or osteochondral injuries in which case the period of prophylaxis was extended to 6 weeks.
The removable walking boot was kept on at all times for the first 3 weeks, followed by the use of an ankle brace for another 3 weeks. Formal physical therapy was initiated at 3 to 4 weeks postoperatively after removal of the ankle brace. A return to noncontact sports was expected at 6 to 8 weeks. Patients may return to sports without limitations at approximately 3 months from the operation. In cases of chondral or osteochondral injuries, no weight bearing was allowed for 4 to 6 weeks. Formal physical therapy was initiated at 3 weeks postoperatively after removal of the ankle brace. A return to full activities could be expected at 3 to 6 months.
Results
Sixteen patients (16 ankles) underwent an all-inside arthroscopic lateral ligament repair with a knotless suture anchors technique. During the procedure, 13 patients were diagnosed with an isolated ATFL injury, and in 3 patients, both the ATFL and CFL were affected. Six patients had additional procedures on the ankle at the time of the arthroscopic lateral ligament repair. These additional procedures included osteochondral talar injury debridement and drilling in 2 patients, anterolateral soft-tissue impingement debridement in 2 patients, and tendoscopy of the peroneal tendons in 2 patients. During peroneal tendoscopy, a distal insertion of the muscle of the peroneus brevis tendon was removed in the 2 patients, and a debridement of a superficial tear of the peroneus brevis was performed in 1 patient.
At follow-up, all patients reported subjective improvement in their ankle stability. To date, no patient knowingly required revision lateral ankle ligament repair. The 3 first patients that were treated with this technique had a residual tilt after surgery during clinical exploration but were doing fine with subjectively improved stability.
All patients returned to their daily activities without difficulties. Patients that practiced sports, returned to that activity without limitations. Taping was recommended during sports activity. Six of the patients presented signs of plantarflexion deficit of the ankle compared to the contralateral side. Two patients had a deficit of more than 10 degrees of plantarflexion, and 4 patients presented a plantarflexion deficit from 5 degrees to 10 degrees.
The mean AOFAS score increased from 67 preoperatively (range, 59-77) to 97 (range, 95-100) at final follow-up. No major or neurological complications were reported. Superficial infection of the distal portal of the peroneal tendoscopy was observed in 1 case that resolved with conservative treatment. One of the patients had delayed wound healing of the anterolateral portal which was successfully treated with conservative measures.
Discussion
Lateral collateral ankle ligament repair should be considered in patients with chronic recurrent instability episodes despite appropriate conservative treatment. Recurrent instability of the ankle is a known sequela following inversion injuries, and is estimated to occur in approximately 10 to 20% of patients regardless of the type of initial treatment.6,24 Pijnenburg et al reported an abnormal anterior drawer sign in 42% of patients after an ankle sprain. 35
The ATFL is the most frequently injured ligament of the ankle. Brostrom 6 surgically explored 105 sprained ankles and found that two-thirds of the ankles had an ATFL tear, while a quarter of the ankles had a combined ATFL and CFL rupture. A thorough knowledge of the anatomy of the lateral collateral ligaments is absolutely necessary for a correct ankle ligament repair. The ATFL is a flat, quadrilateral ligament which originates in its entirety from the anterior margin of the lateral malleolus. From this origin it runs anteromedially to the insertion point at the talar body immediately anterior to the joint surface articulating with the lateral malleolus. The ligament is virtually horizontal to the ankle in the neutral position but moves upward in dorsiflexion and downward in plantarflexion. This ligament is in close contact with the capsule of the ankle joint, and commonly has a double-band morphology.10,18,33,37 The upper band is larger than the lower one. The upper band reaches the insertion on the fibula of the anterior tibiofibular ligament, and is observed during ankle arthroscopy to be located in the floor of the lateral recess of the ankle. This anatomic fact is critical to locating the anchor position during arthroscopic ligament repair. The inferior band reaches the origin of the calcaneofibular ligament.
The CFL is a thick, cordlike ligament that originates at the anterior edge of the lateral malleolus, right below the origin of the lower band of the anterior talofibular ligament, to which it can be joined by arciform fibers. It is important to note that the origin of this ligament does not reach the tip of the malleolus, which remains free from ligamentous insertions. In the neutral position, the ligament courses backward, downward, and medially inserts in a small tubercle in the posterior region of the lateral calcaneus posterior to the peroneal tubercle. This ligament becomes horizontal during extension and vertical in flexion, remaining tense throughout its entire arc of motion. The ligament is relaxed in the valgus position and tense in the varus position. 36
The arthroscopic treatment of the ankle continues to evolve. Due to several intra-articular conditions associated with ankle instability that can contribute to pain and dysfunction, arthroscopic evaluation may be beneficial.7,13,21,23,28 Chondral lesions, loose bodies, or other intra-articular pathology have been observed from 66% to 93% of unstable ankles on arthroscopic examination.5,21,23,28,40 Several investigators have proposed an increasing role for arthroscopy as a definitive treatment.1,8,27,31,32,34 Hawkins 20 was the first to describe an arthroscopic approach to lateral collateral ankle ligament repair with a stapling technique. A suture anchor technique was later developed to avoid problems caused by the prominent staples. 26 More recently, other authors have developed arthroscopic assisted suture anchor techniques to repair lateral collateral ankle ligament instability with excellent result.1,8,27,34 However, a high rate of complications (5.3% to 29%) has been described in these case series.
Neuritis of the superficial peroneal or sural nerve, and pain or discomfort due to a prominent anchor or suture knot are the most frequent complications reported.1,8,27 Complications related to the superficial peroneal nerve have been reported with arthroscopic techniques in the ankle.3,14,15 Arthroscopic experience of the surgeon and a thorough knowledge of foot and ankle anatomy are critical to reduce the risk of complications during the procedure. Proper caution on the part of the surgeon when creating portals, introducing instruments, or using instruments, is also important to reduce the risk of nerve injuries. The superficial peroneal nerve should be marked to avoid its injury when creating the anterolateral portal. However, the location of the superficial peroneal nerve changes with different foot and ankle positions. The nerve moves laterally when the ankle ranges from combined plantarflexion and inversion to the neutral or dorsiflexed position. This situation provides a false sense of safety when making the anterolateral portal in the normal or slight dorsiflexed position because the marking does not correspond to the subcutaneous location of the nerve in this position. The mean displacement of the nerve through ankle range of motion has been measured. When the ankle is moved from 10 degrees plantarflexion and inversion to the neutral ankle position, the nerve moves a mean of 2.4 mm to the lateral side. When moved from 10 degrees plantarflexion and inversion to 5 degrees of dorsiflexion, it moves 3.6 mm to the lateral side. 9 The use of a cannula introduced in the anterolateral portal will help to avoid peroneal superficial nerve injuries during the procedure. With regards to the sural nerve, the risk of injuries is greatly reduced by the all-inside technique when compared to other techniques where suture is passed outside the ankle through a skin incision.
All patients reported subjective improvement in their ankle stability, and returned to their daily activities and sports without difficulties. Six of them presented signs of plantarflexion deficit of the ankle during clinical exploration at follow-up. This well-tolerated stiffness may be a normal consequence of surgery and is therefore not recognized as a complication.
Finally, the use of a knotless suture anchor technique had advantages over traditional suture anchors. The possibility of a prominent anchor or suture knot were avoided with the new knotless anchors.
This study was limited by the fact that a control group was not included to compare the outcome with the all-inside arthroscopic ligament repair. Nonetheless, previous studies indicate that open surgery or arthroscopic-assisted procedures produce similar satisfactory results. However, arthroscopy has advantages over open surgery being a less aggressive surgery. Morbidity can be lower and the cosmetic result is better than open surgery. Concomitant intra-articular injuries can be evaluated and treated arthroscopically before the ligament repair, using the same portals. It can be easily converted to an open technique, if required.
Another limit of our study was the fact that the instability was not quantified preoperatively and postoperatively which is an inherent problem with all studies on ankle instability repair. Lateral ligament disruption of the ankle is generally diagnosed using stress radiography of the talocrural joint. However, this method provides only a mechanical assessment of the stability of the ankle under a limited stress force, which may be less than actual tensile force to the ligaments in sports or other strong activities. If there is a partial tear of a ligament and/or deterioration of the ligament with preserved continuity, stress radiography results can be negative despite the patients’ ankle disability. On the other hand, stress radiography uses selected force-plate postural control measures to assess ankle instability. However, no single force-plate measure is truly effective in predicting if an individual has ankle instability or not.
In conclusion, ankle instability can be successfully treated by arthroscopic methods. The all-inside arthroscopic lateral collateral ligament repair with a knotless suture anchors technique was a reproducible and safe technique. Concomitant intra-articular injuries were evaluated and treated arthroscopically before the ligament repair. This procedure required some arthroscopic skills and would likely not be ideal for the novice arthroscopist. The use of a knotless anchor significantly simplified the procedure. This arthroscopic technique provided an anatomic repair and restored ankle stability while still preserving all the related arthroscopic advantages.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.