
Abstract
Background:
There are conflicting data regarding the benefits of delaying operative fixation of calcaneus fractures to decrease wound complication rates. The purpose of this study was to examine the effect of delaying fixation on wound complication rates as well as to identify other risk factors.
Methods:
A retrospective review at 4 institutions, including 24 surgeons, identified 405 closed, operatively treated, intra-articular calcaneus fractures. We compared fractures with and without wound complications with regards to patient demographics, medical risk factors, fracture severity, time to fixation, operative approach, primary subtalar arthrodesis, and surgeon experience.
Results:
Wound complications were observed in 21% (87/405) of fractures, of which 33% (29/87) required operative intervention. Male sex (P = .032), smoking (P = .028), and the extensile lateral approach (P < .001) were associated with higher complication rates. Fractures treated with an extensile lateral approach had an overall wound complication rate of 32.1%, while those treated with a sinus tarsi or percutaneous approach had an overall wound complication rate of 8.3% (odds ratio [OR], 5.3; 95% confidence interval [CI], 2.9-9.5; P < .001). Among patients treated with an extensile lateral approach, delayed operative fixation did not decrease wound complication rates despite comparable fracture severity across time points. In contrast, among fractures treated with less invasive approaches, delayed fixation beyond 2 weeks resulted in a significantly increased wound complication rate of 15.2% as compared to a wound complication rate of only 2.1% among fractures treated within a week of injury (OR, 3.2; 95% CI, 1.3-9.5; P = .01). This was observed despite similar fracture severity across time points. Primary subtalar arthrodesis did not impact complication rates. A higher wound complication rate among senior surgeons was likely secondary to their predilection for the extensile lateral approach.
Conclusion:
Delaying definitive fixation of closed, intra-articular calcaneus fractures did not decrease wound complication rates when using the extensile lateral approach, and we found an increased wound complication rate when using less invasive approaches.
Level of Evidence:
Level III, observational study.
The calcaneus is the most commonly fractured tarsal bone, making up approximately 2% of all fractures.3,14,24,36 Males are disproportionately affected, as are younger individuals, with a peak incidence in the third decade of life. 24 The economic and social impacts on affected individuals and their families are tremendous.6,40,41 Approximately 30% of such fractures occur in manual laborers, and 20% are work related. 24 Functional outcomes may be similar to those incurred after myocardial infarction.14,41 Among heavy laborers, 25% are unable to return to work, and the remainder frequently do so at a diminished level.10,13,14
Many controversies surround the treatment of intra-articular calcaneus fractures. In a recent review of the Cochrane database, Bruce and Sutherland 7 found no difference between operative and nonoperative treatment with regards to functional status and health-related quality of life after 3 years. Buckley and Tough 10 also found similar results, although a subset analysis revealed a benefit to operative fixation in certain populations. 20 Other studies, however, have demonstrated that operative fixation leads to predictable medium-term to long-term improvement in functional outcomes. 31 Furthermore, even if posttraumatic arthrosis occurs, an initial operative intervention has been shown to facilitate subsequent subtalar arthrodesis with decreased wound complication rates and improved functional outcomes. 29 Indeed, for higher grade injuries, some have advocated primary subtalar arthrodesis, although such studies did not evaluate whether wound complications were higher with this strategy.17,23,26,28
Operative interventions have been shown to have an overall short-term wound complication rate approaching 30%, with reported complications ranging from superficial skin slough to deep infections. 22 The incidence of deep infections varies widely in the literature, ranging from 1.8% to 21%. 12 Due to relatively high rates of wound complications, surgeons have traditionally delayed operative treatment for 1 to 2 weeks to allow for a reduction in swelling and return of skin wrinkling.14,33 Although widespread, the benefit of operative delay is not clearly supported by the literature.
Less invasive operative approaches such as the sinus tarsi approach, external fixation, and percutaneous and arthroscopically assisted fixation have become increasingly popular in hopes of decreasing wound complication rates.11,20,30,35,42 While the complication rates of less invasive techniques have been reported to be between 6% to 8.5%, the optimal timing to operative fixation using these approaches has not been determined. 20
The purposes of this study were to assess whether delaying operative fixation of intra-articular calcaneus fractures resulted in decreased wound complication rates and whether other factors, including patient demographics, associated medical risk factors, fracture severity, operative approach, primary subtalar arthrodesis, and surgeon experience, impacted wound complication rates.
Methods
A retrospective review was performed at 4 institutions between 2002 and 2012. Inclusion criteria included any patient equal to or older than 17 years of age who sustained a closed, intra-articular calcaneus fracture and underwent operative fixation. Patients younger than 17 years of age, open fractures, and those who underwent initial external fixation were excluded.
Four hundred five closed, intra-articular calcaneus fractures treated operatively from 2002 to 2012 were included, with an average postoperative follow-up of 7 months (range, 0.5-13 months). All fractures had adequate follow-up to document either wound healing sufficient to allow suture removal or the development of a wound complication. The average age at presentation was 45 years (range, 17-79 years), of which 80% (325/405) were male and 20% (80/405) were female.
Patient demographics were collected from the medical record, as were medical risk factors including a history of smoking, diabetes, osteoporosis, rheumatoid arthritis, peripheral vascular disease, and postoperative noncompliance. Also recorded were the days from initial injury to definitive fixation and length of follow-up. Operative records were examined to determine the approach, classified as either extensile lateral, sinus tarsi, or percutaneous (defined as no direct visualization of fracture fragments). The choice of an operative approach was determined by the treating surgeon. Fractures that underwent primary subtalar arthrodesis were also noted. The Sanders classification was used to classify fractures into grades I, II, III, or IV.
Wound complications were substratified into 4 categories based on the treatment rendered. A superficial infection was defined as a postoperative wound complication requiring only oral antibiotics. A deep infection was one requiring intravenous antibiotics and/or irrigation and debridement. Superficial wound dehiscence was one necessitating local wound care. Deep wound dehiscence was one necessitating a return to the operating room for any further procedures.
All operative procedures and postoperative evaluations were performed by staff surgeons with either trauma or foot and ankle subspecialty training. Surgeon experience was arbitrarily stratified into categories designated as junior level (0-8 years in practice), intermediate level (9-15 years), and senior level (greater than 15 years).
All statistical analyses and interpretation of data were aided by a PhD-level statistician. For statistical analysis, patients were stratified into those who experienced a wound complication and those who did not. Univariate statistics included the Fisher exact test for binary proportions for assessing differences between patients with and without wound complications (infection, dehiscence) and the Pearson χ2 test for variables having more than 2 levels. In addition, median age and follow-up time were compared using the Mann-Whitney U test. Multivariate analysis was performed using logistic regression with a backward stepwise procedure and the likelihood ratio test to assess statistical significance; here, adjusted odds ratios (ORs) were calculated using maximum likelihood methods to provide measures of risk with precision around the estimates based on 95% confidence intervals (CIs).
Results
Overview
Results as related to fracture classification, time to definitive fixation, utilization of an operative approach, surgeon experience, and other comorbidities are detailed in Table 1. The overall wound complication rate was 21% (87/405). Wound dehiscence occurred in 14% (57/405) of fractures. Eleven percent (46/405) were superficial, and 3% (11/405) were deep. Wound infections occurred in 11% (45/405) of fractures. Seven percent (27/405) were superficial, and 4% (18/405) were deep. There was overlap between the various groups in that 2% (9/405) of fractures developed both superficial wound dehiscence and a superficial wound infection, while 1% (6/405) developed both deep wound dehiscence and a deep wound infection.
Characteristics and Wound-related Complications of the Calcaneal Fracture Cohort (N = 405).
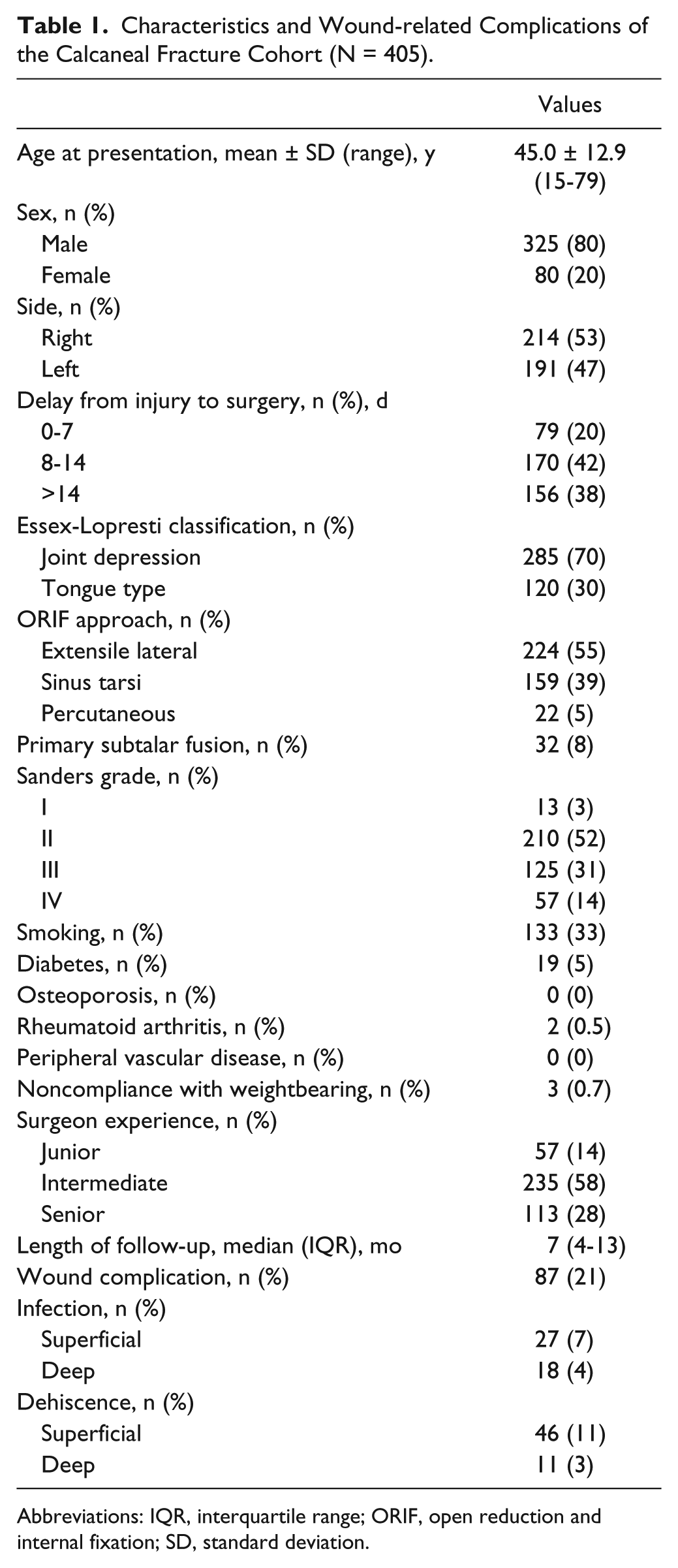
Abbreviations: IQR, interquartile range; ORIF, open reduction and internal fixation; SD, standard deviation.
Operative Approach
For the purposes of statistical analysis, data for patients undergoing percutaneous approaches were combined with those undergoing sinus tarsi approaches and ultimately compared to results from the extensile lateral approach. Univariate analysis across the entire cohort revealed a significant association between the operative approach and wound complication rates. Fractures treated with an extensile lateral approach had an overall wound complication rate of 32.1%, while those treated with a sinus tarsi or percutaneous approach had an overall wound complication rate of 8.3% (P < .001). Logistic regression highlighted that injuries treated with an extensile lateral approach were 5 times more likely to develop a wound complication than those treated with a sinus tarsi or percutaneous approach (OR, 5.3; 95% CI, 2.9-9.5; P < .001). Fracture severity as defined by the Sanders grade, however, was higher among fractures treated with an extensile lateral approach (P < .001).
Time to Surgery
A delay to operative fixation appeared to increase wound complication rates across the entire cohort (P = .015). Subgroup univariate analysis, however, underscored that this finding was dependent on the operative approach (Table 2). Among the 224 fractures treated with an extensile lateral approach, 32% (72/224) developed wound complications, but this was independent of whether operative fixation was performed at 0 to 7 days (11/32, 34%), 8 to 14 days (23/82, 28%), or greater than 14 days (38/110, 35%) (P = .61) (Figure 1). Injury severity was statistically similar across time points (P = .19), and the groups were otherwise matched for all other nonfracture variables examined. Among the 181 fractures treated with either a sinus tarsi or percutaneous approach, 8% (15/181) developed wound complications. There was an observed increase in wound complication rates with delayed operative fixation when comparing results at 0 to 7 days (1/47, 2%), 8 to 14 days (7/88, 8%), and greater than 14 days (7/46, 15%) after the injury. Patients who underwent operative fixation using a sinus tarsi or percutaneous approach more than 14 days after the initial injury were 3 times as likely to develop a wound complication than those who underwent operative fixation in the first week (OR, 3.2; 95% CI, 1.3-9.5; P = .01). This was true despite similar injury severity across both time points (P = .425).
Wound Complication Rates Stratified by Operative Approach and Time to Surgery.
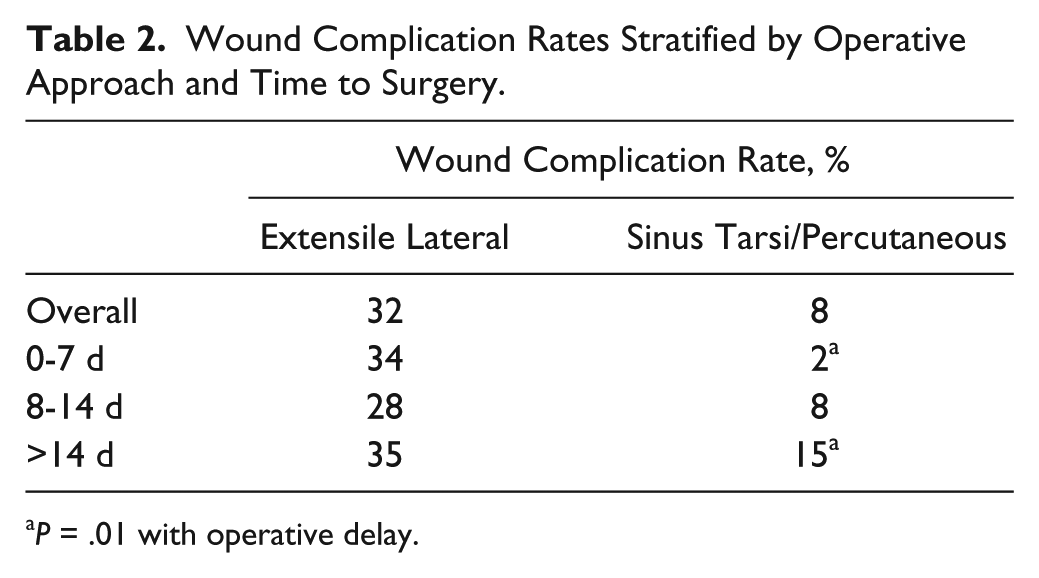
P = .01 with operative delay.
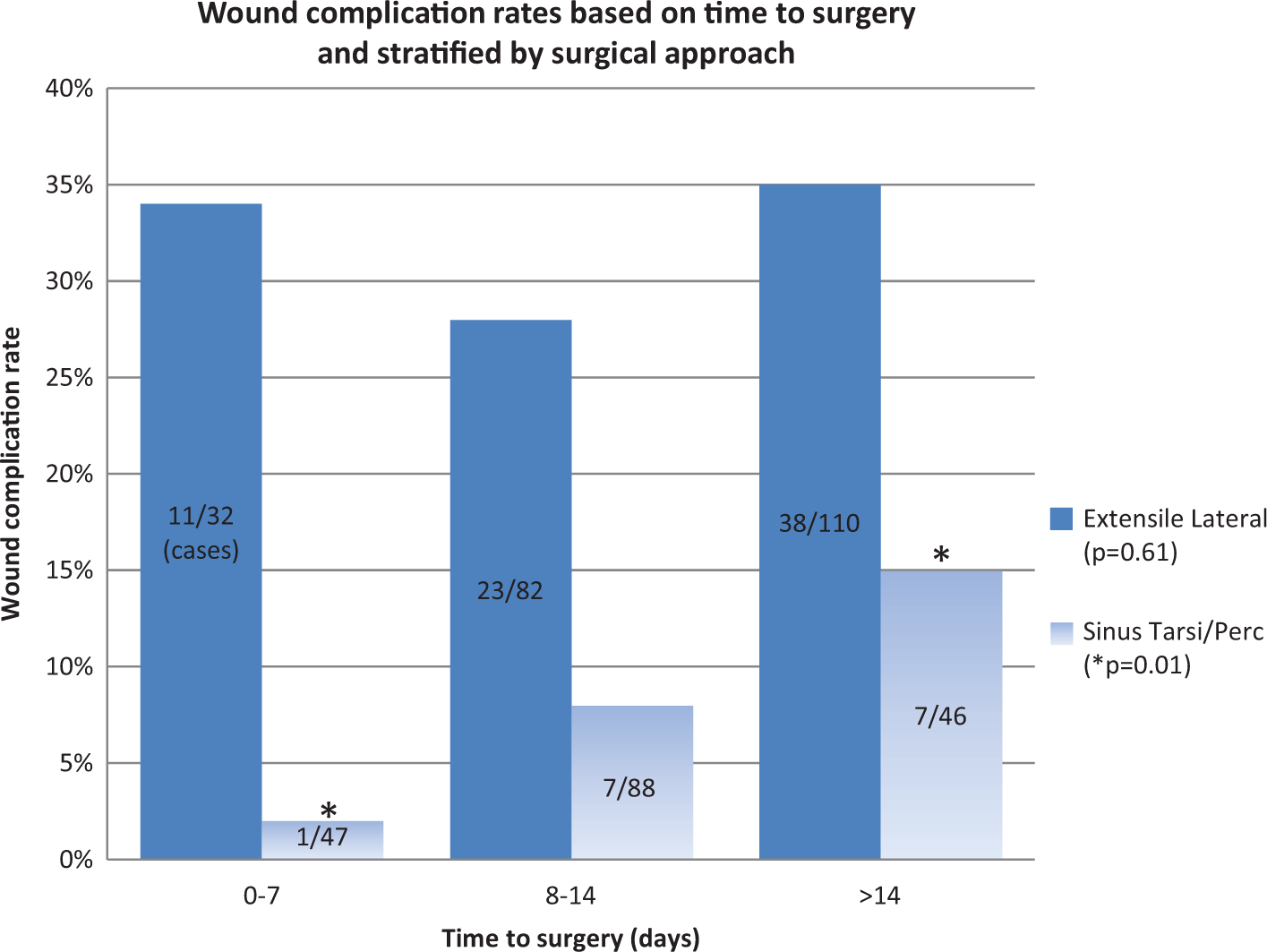
Demonstrates that delaying surgery does not decrease wound complication rates when using the extensile lateral approach and may actually increase wound complication rates when using the sinus tarsi or percutaneous approach.
Fracture Classification
A comparison of wound complication rates for Sanders grade I/II (low-grade injuries: 39/223, 17.5%) versus Sanders grade III/IV (high-grade injuries: 48/182, 26.4%) revealed that fracture severity did not significantly impact wound complication rates across the entire cohort (P = .13). Subgroup univariate analysis by operative approach, however, revealed that while fracture severity did not impact complication rates when using an extensile lateral approach (32.7% vs 31.7%, respectively; P = .88), it did do so when using a sinus tarsi or percutaneous approach (4.9% vs 15.3%, respectively; P = .018). Thus, high-grade fractures had significantly higher wound complication rates than low-grade fractures when using a sinus tarsi or percutaneous approach.
Surgeon Experience
There were 12 junior-level, 6 intermediate-level, and 6 senior-level surgeons included. Initial analysis suggested that wound complications were significantly more common in fractures treated by senior surgeons (P = .006). Further analysis of the operative approach based on surgeon experience, however, revealed that senior surgeons were more likely to utilize an extensile lateral approach (P < .001), which had higher wound complication rates, as discussed above (Figure 2). Notably, cohorts stratified by surgeon experience were otherwise comparable with regard to all other variables, including fracture severity (ie, senior surgeons were not predominantly treating more severe injuries).
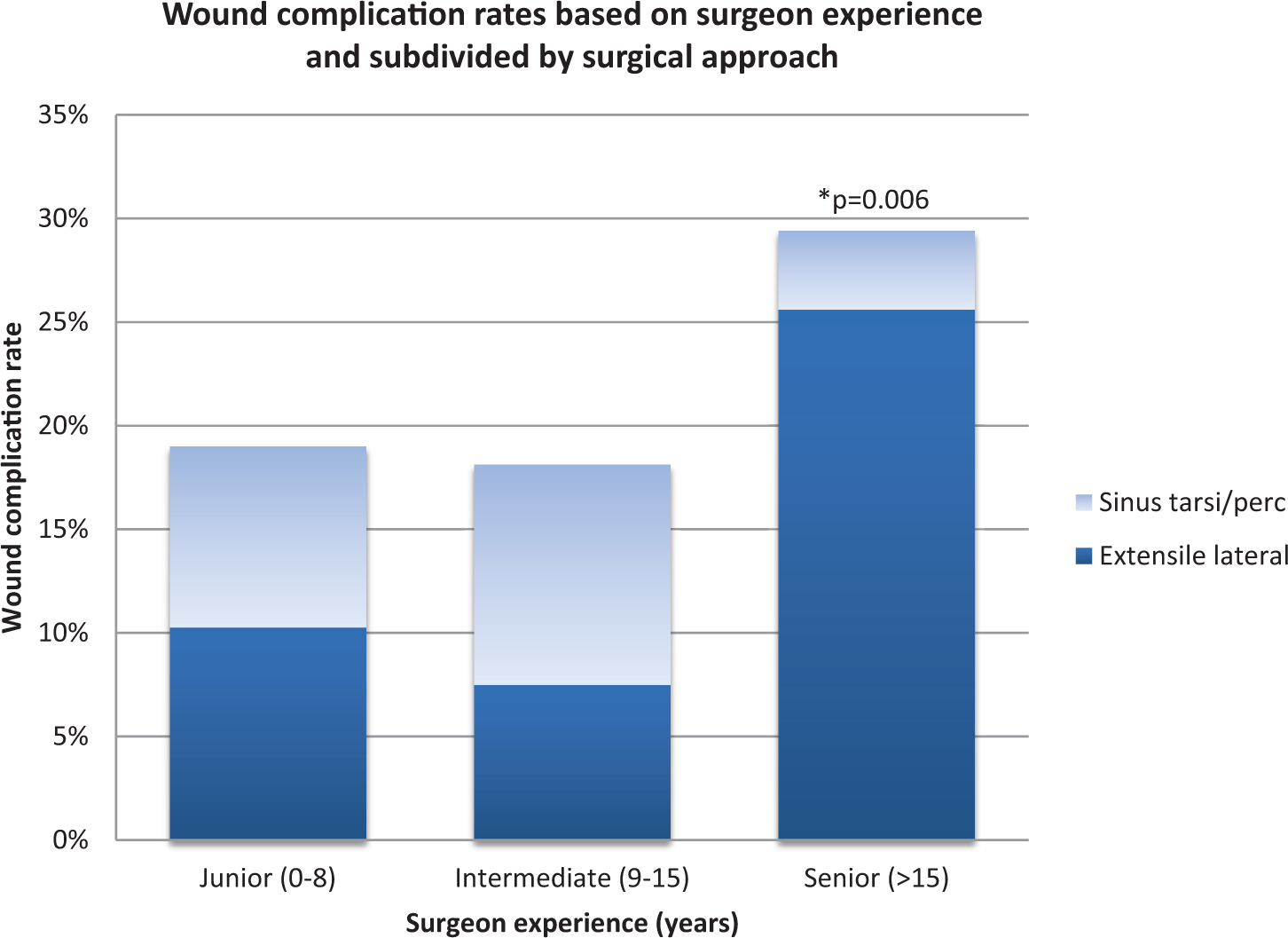
Senior surgeons experienced significantly higher wound complication rates than junior or intermediate surgeons, but their preference for the extensile lateral approach almost certainly underlay these higher rates given that fracture severity did not differ across groups.
Multivariable Analyses
Entire cohort
A multivariable logistic regression analysis was performed across the entire cohort to identify independent risk factors of wound complications. Only sex (OR, 2.1; 95% CI, 1.0-4.3; P = .032), smoking (OR, 1.9; 95% CI, 1.1-3.3; P = .028), and an extensile lateral approach (OR, 6.5; 95% CI, 5.5-12.3; P < .001) were significant risk factors for wound complications. Injuries treated with an extensile lateral approach had a 5-fold increase in wound complication rates as compared to those treated with a sinus tarsi or percutaneous approach (OR, 5.3; 95% CI, 2.9-9.5; P < .001). Diabetes was associated with an observed increase in wound complication rates, although with the numbers available, this did not reach statistical significance (P = .12).
Operative approach
Given the independent predictive value of the operative approach, a multivariable logistic regression analysis was performed for each demographic subgroup based on the operative approach. Among those fractures treated with an extensile lateral approach, smoking significantly increased the risk of wound complications (OR, 2.2; 95% CI, 1.2-4.2; P = .015). Among those fractures treated with a sinus tarsi or percutaneous approach, sex (P = .02), injury severity (P = .017), and delay greater than 14 days (P = .049) significantly impacted wound complication rates. Subgroup multivariable analysis revealed a 3-fold higher rate of wound complications with operative delay beyond 2 weeks when using less invasive approaches (OR, 3.2; 95% CI, 1.3-9.5; P = .01). This was independent of other risk factors such as sex, fracture severity, and smoking status.
Fractures treated with an extensile lateral approach were more likely to be high grade than those treated with a sinus tarsi or percutaneous approach (P < .001). Nonetheless, multivariable analysis demonstrated that when using an extensile lateral approach, fracture severity did not independently contribute to wound complication rates among those fractures treated with an extensile lateral approach (P = .25). In contrast, fracture severity directly impacted wound complication rates when utilizing a sinus tarsi or percutaneous approach, with high-grade injuries more likely to develop a wound complication (OR, 3.5; 95% CI, 1.3-10.3; P = .018).
Discussion
This study represents the largest series in the literature examining risk factors predictive of wound complication rates following operative fixation of closed, intra-articular calcaneus fractures. The overall wound complication rate was 21% (87/405), well within the range of 18% to 30% reported in the literature.13,14 The incidence of superficial and deep wound infections in our study was also comparable to prior studies that similarly defined superficial and deep infections.12,31
Timing to Operative Fixation
Our study did not support traditional teaching that delaying operative fixation of intra-articular calcaneus fractures decreases wound complication rates. We found that delaying operative treatment did not decrease wound complication rates when using an extensile lateral approach. Furthermore, when using a sinus tarsi or percutaneous approach, operative delay greater than 2 weeks was associated with significantly increased wound complication rates independent of fracture severity. Possible explanations include increasing consolidation of fracture fragments resulting in more difficult reductions, greater soft tissue manipulation when utilizing a more limited exposure, or soft tissue contraction around a shortened calcaneus associated with delayed intervention. Nonetheless, the sinus tarsi and percutaneous approaches had significantly lower wound complication rates than the extensile lateral approach, irrespective of time to surgery.
Traditional teaching that operative fixation should be delayed 1 to 2 weeks to allow for soft tissue swelling to subside is based on limited evidence and anecdotal experience.12,32,33 Several earlier studies demonstrated higher infection rates with operative delays less than 5 to 7 days.1,2 Conversely, surgeons have also been discouraged from delaying fixation beyond 3 to 4 weeks due to the difficulties of fracture reduction after consolidation has occurred. 32 Other studies have found increased infection rates when fixation was delayed greater than 14 days.21,38
More recent studies by Folk et al, 15 Court-Brown et al, 12 and Ho et al 18 have not demonstrated that delay to surgery influences wound complications. Fractures within these studies were treated exclusively by the extensile lateral approach, and the majority of patients were treated in less than 7 days. One study also included open fractures, which confounded interpretation and applicability to closed injuries. 15
While previous studies1,2,12,15,18,38 reported conflicting recommendations regarding the optimal timing of operative fixation, methodological issues related to statistical analysis make interpretation difficult. Without multivariable analysis, timing of operative interventions can be confounded by other variables.
Operative Approach
The extensile lateral approach offers excellent exposure to fracture fragments and continues to be popular among surgeons, especially for more complex fractures. Indeed, in our study, fractures treated by the extensile lateral approach were significantly more likely to be high grade than those treated with a sinus tarsi or percutaneous approach (55% vs 30%, respectively; P < .001). Nonetheless, multivariate analysis underscored that fracture severity did not independently predict wound complication rates when using the extensile lateral approach, suggesting that other factors are responsible.
The complication rates following the extensile lateral approach have been well scrutinized, varying from 2% to 29%.4,13,14,20 It is hypothesized that devascularization of fracture fragments, a larger surgical field, longer operative time, potential dead space, and tenuous fasciocutaneous flaps all play a role. 5 Our results support this hypothesis in suggesting that complication risks are inherent to the exposure and unrelated to the timing of operative fixation.
Another explanation is that multiple factors affect wound complication rates, with the predominant factor changing with a delay in operative fixation. Early on, incisions through a traumatized, contused, and edematous soft tissue envelope may be responsible. Later, complications may be due to soft tissue contractures and increased soft tissue tension after restoration of calcaneal anatomy. This theory, however, cannot be substantiated by the current study.
Minimally invasive techniques were developed because of complications related to the extensile lateral approach.11,20,30,42 Kline et al 20 found complication rates to be significantly less when utilizing the sinus tarsi approach (6% vs 29%, respectively). Other smaller studies have observed lower wound complication rates in the sinus tarsi or percutaneous cohorts, although without statistical significance. 20
Our results are similar in that wound complication rates are lower at all time points when using less invasive approaches. Interestingly, this advantage diminished when they were used to treat higher grade fractures. When either the sinus tarsi or percutaneous approach was used, higher grade fractures resulted in higher wound complication rates (P = .018).
Subtalar Arthrodesis
Primary subtalar arthrodesis has been proposed as an alternative treatment of high-grade calcaneus fractures.17,23,26,28 Proponents argue that primary subtalar arthrodesis allows for faster recovery and good to excellent clinical, functional, and radiographic outcomes.19,23,28 Due to small cohorts in previous studies, the complication rate following primary subtalar arthrodesis as it relates to the timing of operative fixation is not well established. To the best of our knowledge, this study is the first to suggest that performing primary subtalar arthrodesis as the index procedure for the treatment of intra-articular calcaneus fractures, as compared to a matched cohort of patients undergoing open reduction and internal fixation, may not be an independent factor for increasing wound complication rates, regardless of the operative approach.
Fracture Classification
The Sanders classification system is the most widely used for calcaneus fractures. Ding et al 13 suggested that the Sanders classification is predictive of wound complications after an extensile lateral approach, with higher grade injuries resulting in higher wound complication rates. This was attributed to increased operative time, blood loss, and extent of soft tissue damage.
It is unclear based on their statistical analysis whether the Sanders classification was an independent risk factor. Our study does not corroborate their findings. When using an extensile lateral approach, fracture severity as an independent factor did not appear to result in higher wound complication rates. In contrast, our work underscores that increased fracture severity does result in increased wound complication rates when using less invasive approaches.
Sex and Associated Medical Comorbidities
The association between male sex and calcaneus fractures is well established. Previous studies have found that males are between 2 to 3 times more likely to sustain calcaneus fractures and that females have better functional outcomes.14,24 The relationship between male sex and wound complication rates, however, is less established. Independent of the fact that males made up the majority of our cohort, male sex was statistically associated with increased wound complications. Although Buckley et al 8 demonstrated that women tend to have higher outcome scores after operative treatment, this study did not correlate sex with wound complications, nor did it correlate wound complications with outcomes. SooHoo et al 37 performed a large-scale review of short- and long-term complications in 4481 patients who underwent calcaneal open reduction and internal fixation using a state-wide discharge database and did not find any association with male sex and wound complications, but they only examined complications severe enough to require hospital readmission. The clinical significance of this finding in our study is unclear, and we are unable to postulate a cause for this difference in the context of the demographic variables examined. Smoking was also an independent risk factor but only when using an extensile lateral approach, consistent with the previous literature.1,13,15,25 Tobacco-associated peripheral vascular disease and the vasoconstrictive effects of nicotine may impede blood flow to the skin flap elevated in the extensile lateral approach. 13
With the numbers available to us, we observed higher wound complication rates in patients with diabetes, which is consistent with previous studies (P = .12). Diabetes and its effect on microvasculature are well established.13,15 Some studies have shown it to be an important risk factor for wound complications after calcaneus fractures, while others have found no correlation.5,13,15 This study adds to, but does not solve, that debate.
Surgeon Experience
Previous studies have demonstrated that surgeon experience inversely correlates with complication rates.12,34 Sanders et al 34 found a year-to-year improvement in outcomes over the first 4 years of a surgeon’s practice as measured by the Maryland Foot Score. Court-Brown et al 12 also found that high-volume surgeons who specialize in orthopaedic trauma have significantly fewer complications than nonspecializing surgeons. Poeze et al 27 demonstrated that increasing fracture volume by institution led to fewer complications, implying that increasing experience leads to decreased wound complications and a subsequent need for subtalar arthrodesis. Sanders et al 34 proposed that 35 to 50 cases are required when performing calcaneus fixation before predictable results can be achieved when treating Sanders grade II and III fractures. To our knowledge, no previous study has examined the influence on the operative approach as it relates to surgeon experience. Our study suggests that senior surgeons (greater than 15 years’ experience) may prefer the extensile lateral approach, and the contribution of an operative approach towards complication rates far outweighs the impact of surgeon experience. While there may be several explanations for this, surgeon unfamiliarity with newer techniques is possible.
While the exact experience of each surgeon in this study as it pertains to the volume of calcaneus fractures treated could not be easily quantified, all were staff orthopaedic surgeons fellowship trained in either foot and ankle or trauma. Furthermore, this multicenter study was performed at 4 sites, 3 of which were level I trauma centers and the fourth site being a tertiary care referral center for foot and ankle conditions. Therefore, the staff surgeons likely had a reasonable amount of familiarity with the treatment of calcaneus fractures.
Limitations
There are several limitations to the current work, including the retrospective nature of data collection. Although several authors have established objective grading systems for wound dehiscence/infection,16,32 the application of such criteria in a retrospective manner is inaccurate and impractical. The accuracy of treatment rendered, specifically as it relates to an oral antibiotic regimen or local wound care, was based on the accuracy of the medical record. The exclusion of a small number of cases due to poor documentation may have altered our results. The absence of documented wound complications does not mean that they did not occur. Some patients may have received their postoperative care in another health care facility, in which case complications would not be documented in our records. Furthermore, some patients may have presented with infections after the follow-up period of this retrospective review. Of note, all but 1 of the 405 fractures were followed at least a month and all to suture removal, suggesting that the vast majority of soft tissue complications were captured in this data set. Furthermore, although 15 cases had documented dehiscence and infections based on our criteria, there may have been other cases in which both complications were present but the medical record reported only a single complication. In addition, a small subset of patients who had a very short follow-up may have developed a wound complication unbeknownst to the authors.
While we examined a relatively large number of variables, there are several others that we did not, including body mass index, workers’ compensation, litigation status, hospital admission status on initial presentation, use of compressive devices to further decrease swelling, diuresis, length of surgery, use of bone substitutes, and number of people in the operating room. These variables have all been suggested to affect complication rates.9,13,39 It should also be noted that we did not specifically examine any potential relationships between the quality of reduction or application of a particular chosen operative technique. Each of these variables may influence wound healing, and we recognize that further analysis of these variables could potentially confound conclusions drawn about the pathoetiology of wound complications presented in this work.
Due to the multicenter nature of this study, there is an inevitable degree of variability among various surgeons and institutions. Timing of surgery is influenced by many factors and not solely soft tissue status alone. The “wrinkle sign” is often used by orthopaedic surgeons to signify sufficient resolution of swelling to allow operative fixation, but the presence or use of the wrinkle sign could not be deduced retrospectively. In our cohort, however, higher grade fractures with presumably more tenuous soft tissues were not preferentially delayed. Nonetheless, an assessment of the exact conditions of the soft tissues at either the time of injury or surgery could not be accurately captured retrospectively, and no assumptions can be made that the soft tissue envelope was optimal at the time of surgery. In addition, given the multicenter retrospective nature of this study, it is impossible to reconcile any observed wound complications with each particular surgeon’s indications for surgery and decisions as to the appropriate timing of surgery.
Most importantly, no patient-based outcome measures were reported. Although it may seem intuitive that patients sustaining wound dehiscence or infections would have worse outcomes, we cannot extrapolate this from the current work. As such, no effect of wound complications on functional outcomes or patient satisfaction can be inferred. In addition, there was no comparative assessment of the quality of fracture reduction, and therefore, we are unable to comment on any relationship between the degree of anatomic reduction and any resultant wound complications.
Future studies may choose to focus on outcomes as related to the severity of complications as this may be more meaningful information for treating surgeons. We did not specifically stratify our results based on the severity of the wound complication, given the overall small number that would make additional subset analysis prohibitive. However, we recognize that minor wound complications (which may be defined as not requiring operative interventions) likely have a different impact on the patient as compared to those requiring surgery.
Conclusion
Our study found that delaying definitive fixation of calcaneus fractures did not decrease wound complication rates. When delaying operative fixation greater than 2 weeks, wound complication rates were unchanged when using an extensile lateral approach and increased when using a sinus tarsi or percutaneous approach. The operative approach appeared to have a marked effect, wherein the extensile lateral approach had a significantly higher wound complication rate as compared to less invasive approaches. Fracture severity did not impact wound complication rates when using an extensile lateral approach, but it did when using less invasive approaches. Regardless, even severe fractures treated by less invasive approaches had lower complication rates. Primary subtalar arthrodesis did not lead to increased wound complication rates. Patient characteristics including smoking and male sex contributed to higher wound complications. Although multivariate regression modeling was utilized to identify timing of surgery as an independent variable, the inclusion of certain variables not examined in this work may have led to different results.
Footnotes
Editor’s Note
The authors are to be congratulated for reporting on a large series of patients who underwent operative fixation of calcaneus fractures and the effect of various factors, notably timing of surgery, on wound complication rates. They clearly demonstrated higher wound complication rates for the extensile approach compared to minimally invasive approaches consistent with other studies on that topic. However, as pointed out by them in their limitations, the condition of the soft tissue was not evaluated in this study due to its retrospective design; thus, fracture severity, per the Sander classification, was used to infer the condition of the soft tissue, which may or may not be an accurate measure of the soft tissue condition. Also, it was not possible to determine why patients underwent surgery when they did. It may have been due to the resolution of soft tissue edema, but some part of it may also have been related to the availability of operative time. This study sheds further important light on this challenging problem, wound complications, and ideally will be followed by a prospective study that includes an objective assessment of the soft tissues at the time of surgery.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John Y. Kwon, MD, reports royalty compensation from Trimed Inc and royalty and consulting compensation from Paragon 28, outside the submitted work. Clifford Jeng, MD, is a consultant for OrthoHelix/Tornier and receives fellowship financial support from Arthrex and Synthes, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.