
Abstract
Background:
Proximal tibia bone autograft (PTBG) is regularly used in reconstructive foot, ankle, and maxillofacial surgery. Although many surgeons prefer PTBG rather than the conventional iliac crest, little is known about the remodeling capacity of the proximal tibia after harvesting cancellous bone.
Methods:
Via bilateral postoperative computed tomography of 17 harvesting sites, comparing the defect side with the healthy side, we measured the repair capacity of the proximal tibia in response to bone defect created by the harvest at medium-term follow-up (mean 29 months; range, 7-55 months).
Results:
16 of 17 (94%) cortical defects showed complete consolidation. Cancellous remodeling was graded 0 to 3, with 2 defects showing complete remodeling (grade 3), 4 defects partial remodeling (more than 50%), 8 defects partial remodeling (less than 50%) and 3 defects no remodeling at all (grade 0).
Conclusion:
The proximal tibia has the potential to form new cancellous bone after cancellous bone graft harvesting. More data are required to identify possible variables influencing this remodeling capacity. When performing knee surgery, knee surgeons should take into account the relatively small defect size and the consolidation of the cortical window after proximal tibia bone harvesting.
Level of Evidence:
Level IV, case series.
Proximal tibia bone autograft (PTBG) is regularly used in reconstructive foot, ankle, and maxillofacial surgery.6,22 In foot and ankle surgery, the anatomical location of the proximal tibia metaphysis and relatively low complication rate provide arguments to prefer the proximal tibia metaphysis rather than the traditional iliac crest for bone grafting. Conventional iliac crest bone grafting is associated with a relatively high donor site morbidity including chronic pain, nerve injury to the superficial lateral femoral cutaneous nerve, hematoma, hernia, infection, and fracture of the iliac wing. 3 Proximal tibia bone grafting is particularly convenient because of the anatomical location of the proximal tibia. It can be harvested from the ipsilateral leg without the need for repositioning or draping modifications during surgery. Furthermore, the proximal tibia provides about 30 mL of cancellous bone and is associated with minor complications.8,9,18,27 A complication rate of 1% to 4% is described in the literature, including hematoma, tibial eminence fracture, and superficial wound infection.* The graft may be harvested via the lateral or medial approach with an equal amount of bone graft available.4,10,17 Whitehouse et al 28 reported no major complications over a 5-year period, with 96% of patients being pain free. There has been some debate regarding weight bearing following bone graft harvesting from the proximal tibia. Experimental results on cadavers show that a large amount of cancellous bone can be harvested from the proximal tibia without increasing the risk of fracture when full weight bearing is allowed.2,25 However, there was a negative correlation between the volume of harvested bone and the mean of maximal compressive strength. 25 This implies that the higher the bone volume harvested, the more risk of fracture occurring in the tibia plateau. Nine cases of tibial fracture have been reported in the literature.7,11,13,19,23,24 In the case of Galano and Greisberg, 7 the graft harvested was cortical rather than cancellous, possibly increasing the risk of tibial plateau fracture.
The cancellous bone strength of the proximal tibial metaphysis is particularly of interest for knee surgeons who obtain maximal fixation for various types of reconstructive procedures like anterior cruciate ligament reconstruction and knee arthroplasty. There may be some concerns in this regard whether the fixation after proximal tibia bone grafting is sufficient. Furthermore, there might be a clinically important increased fracture risk after proximal tibia bone grafting.
The goal of this study was to measure the trabecular bone loss and reparative capacity of the proximal tibia after bone grafting. To our knowledge this is the first study that provides postharvesting in vivo data of the remodeling capacity of the proximal tibia. We also wanted to provide objective data about fracture risk in relation to harvesting technique and volume.
Methods
From February 2008 to August 2013, proximal tibia cancellous bone was harvested in 46 patients. This procedure was always performed in combination with foot surgery (hindfoot and midfoot fusions) in the same operative session, and the patients’ medical records were retrospectively reviewed.
Between 5 and 55 months postoperatively, all 46 (100%) patients were contacted and participated in a telephone questionnaire. No postoperative complications were noted in any of the 46 PTBG procedures. Seventeen patients (37%) volunteered to participate in the radiographic portion of the study and signed the informed consent; these patients were further assessed by bilateral computed tomography (CT) of the proximal tibia, comparing the grafting site with the contralateral healthy side. We evaluated cortical consolidation, cancellous remodeling, and morphological characteristics of the defect. Both assessors (V.V., G.V.) were blinded for comparative assessment of the bilateral proximal tibia CT examinations. Interobserver reliability was 100% for grading cortical consolidation and 94% for grading the cancellous remodeling. Mean age of participants was 55 years (range, 35-69 years) and mean remodeling time between harvesting and CT imaging was 29 months (range, 7-55 months).
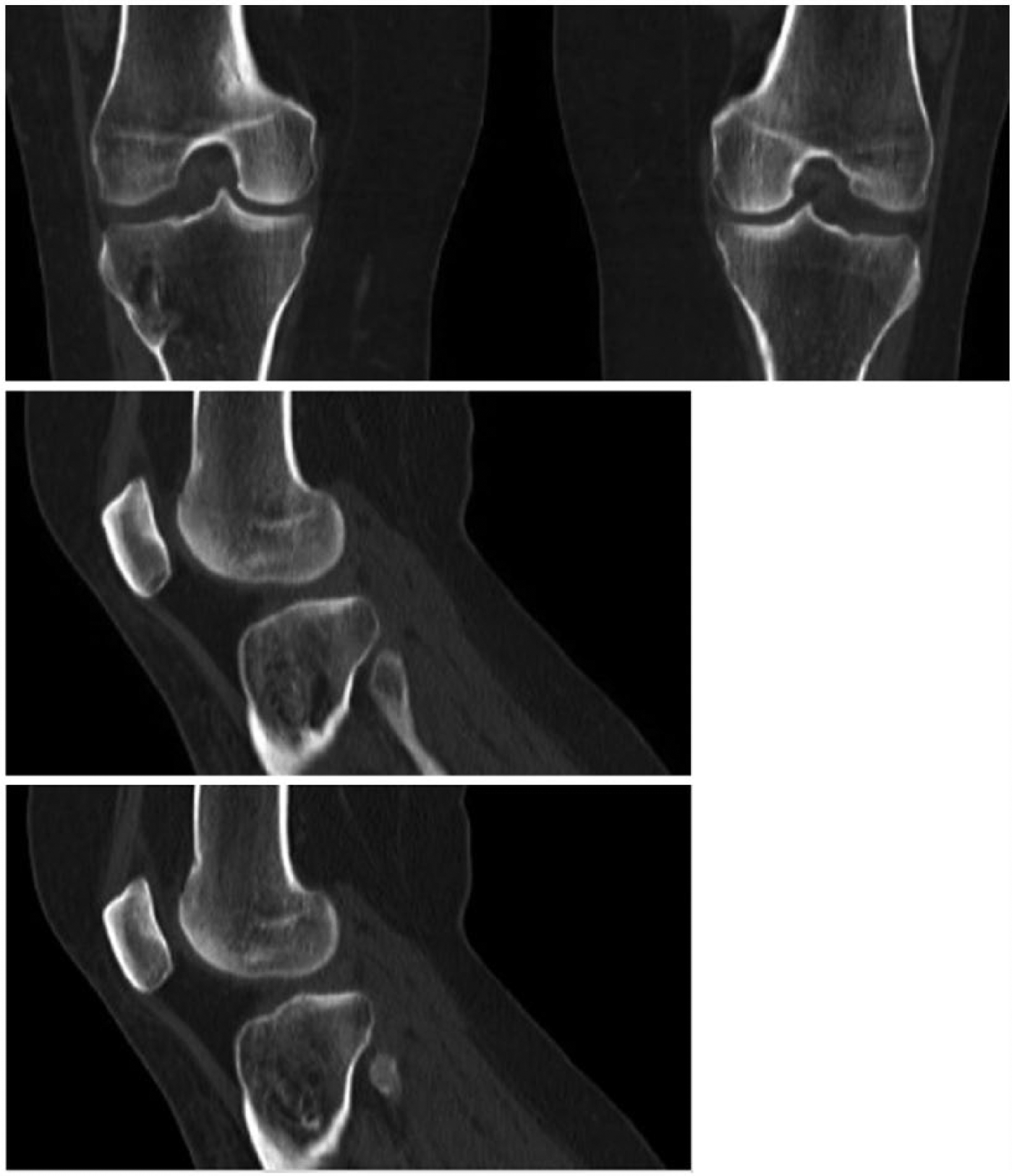
Cortical consolidation was graded either 0 (no continuity of the cortex in the frontal, coronal, and sagittal plane) or 1 (continuity of the cortex in the frontal, coronal, and sagittal plane). The remodeling capacity (ie, the postoperative remodeling status of the cancellous bone) was graded 0 to 3. Grade 0 indicated no remodeling; the metaphyseal defect had a sclerotic lining without any trabecular pattern crossing the defect (Figure 1). Grade 1 indicated that less than 50% of the defect was filled with new trabecular bone. Grade 2 corresponded to more than 50% retrabecularization of the volume of the defect (Figure 2). Grade 3 was complete remodeling, with a symmetric appearance compared with the contralateral proximal tibia and with Hounsfield units (measured over the complete axial surface of the proximal metaphysis) that were equal to or higher than those of the contralateral leg.

Little remodeling 33 months after proximal tibia bone autograft. This lesion was classified as grade 0 remodeling. Note the consolidation of the cortical defect.
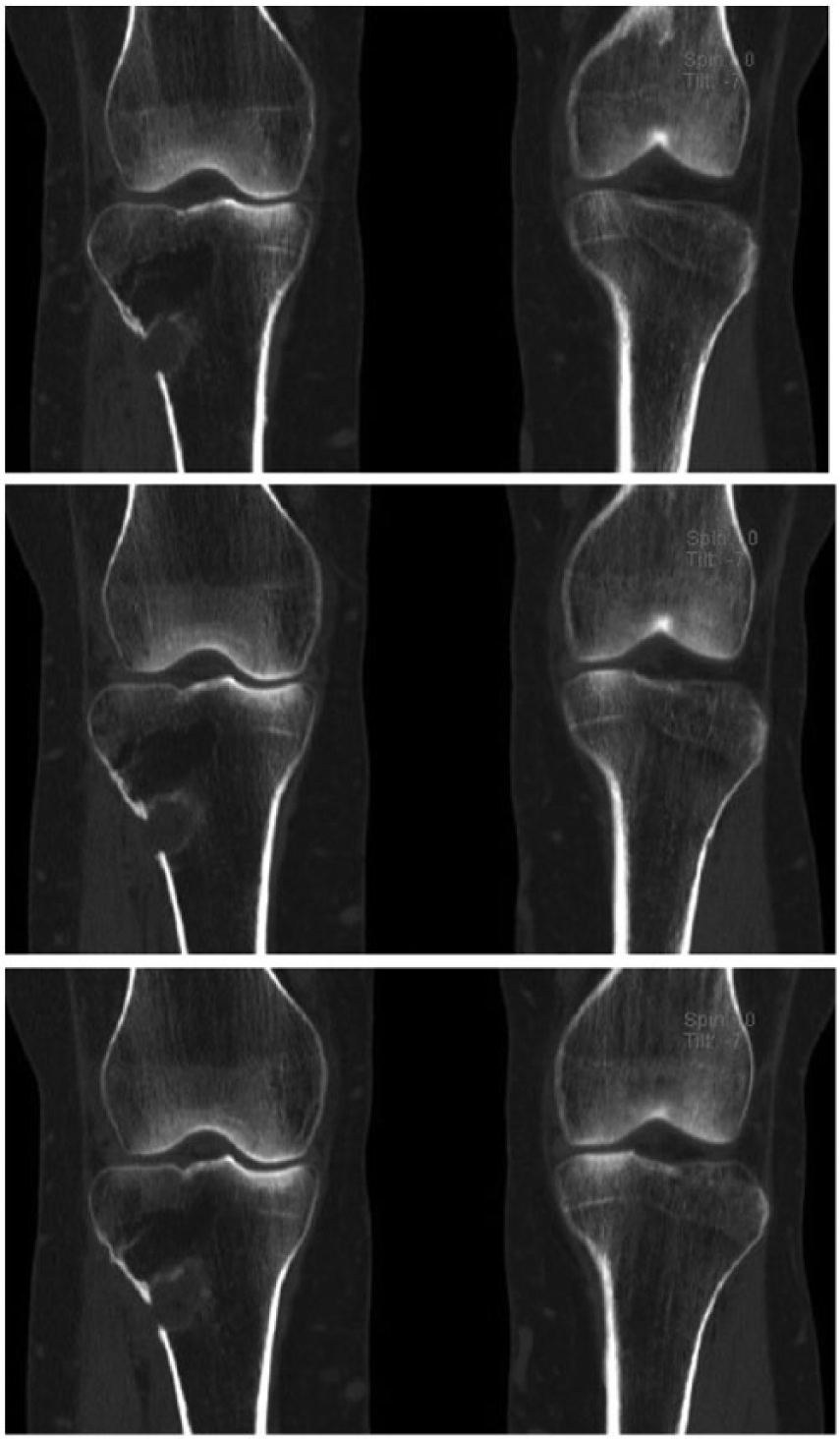
Near-complete remodeling 25 months after right-sided proximal tibia bone autograft. This lesion was classified as grade 2 remodeling. Note the consolidation of the cortical defect.
The graft harvesting was always performed by the same surgeon (G.V.) using the approach described by Mauffrey et al. 17 We used a standard lateral approach and made a cortical window (20 × 5 mm) with an osteotome. The maximal amount of cancellous bone graft was harvested, and in every case the opposite medial cortex was touched with the grafting chisel. The cortical defect was restored by replacing the cortical window. By telephone questionnaire, we retrospectively collected the postoperative complications and current complaints, if any, referable to the graft donor site.
Patients were recalled and evaluated specifically for this study. Our study was performed with the approval of the ethics committee of our clinical institution (H.-Hart Hospital Lier, University Hospital Antwerp), and all participants signed an approved informed consent for participation in the study. The postoperative CT examinations were completely funded by the orthopedic department.
Results
In all 46 cases, telephone interviews revealed no complications (wound infection, hematoma, fracture, nerve injury). One participant reported residual pain on the lateral tibial plateau that corresponded on CT with lateral knee osteoarthritis. We assumed that lateral compartment osteoarthritis was the cause of this residual pain. Regarding the cancellous bone remodeling, 2 defects were completely remodeled (grade 3), 4 defects were graded as more than 50% remodeled (grade 2), 8 defects were graded as less than 50% remodeled (grade 1), and 3 defects showed no remodeling at all (grade 0). The mean cortical defect size (measured in the grade 0 remodeling cases) was estimated to be 4 cm2. Due to the small sample size, we could not perform statistical analysis to find a possible correlation between remodeling capacity and remodeling time, age, sex, or metabolic diseases. Sixteen of the 17 (94%) cortical defects showed complete consolidation, and the thickness of the cortex at the harvesting site was equal to or greater than that on the contralateral side (Table 1, Figures 1-4).
Remodeling Status After Medium-Term Follow-Up.
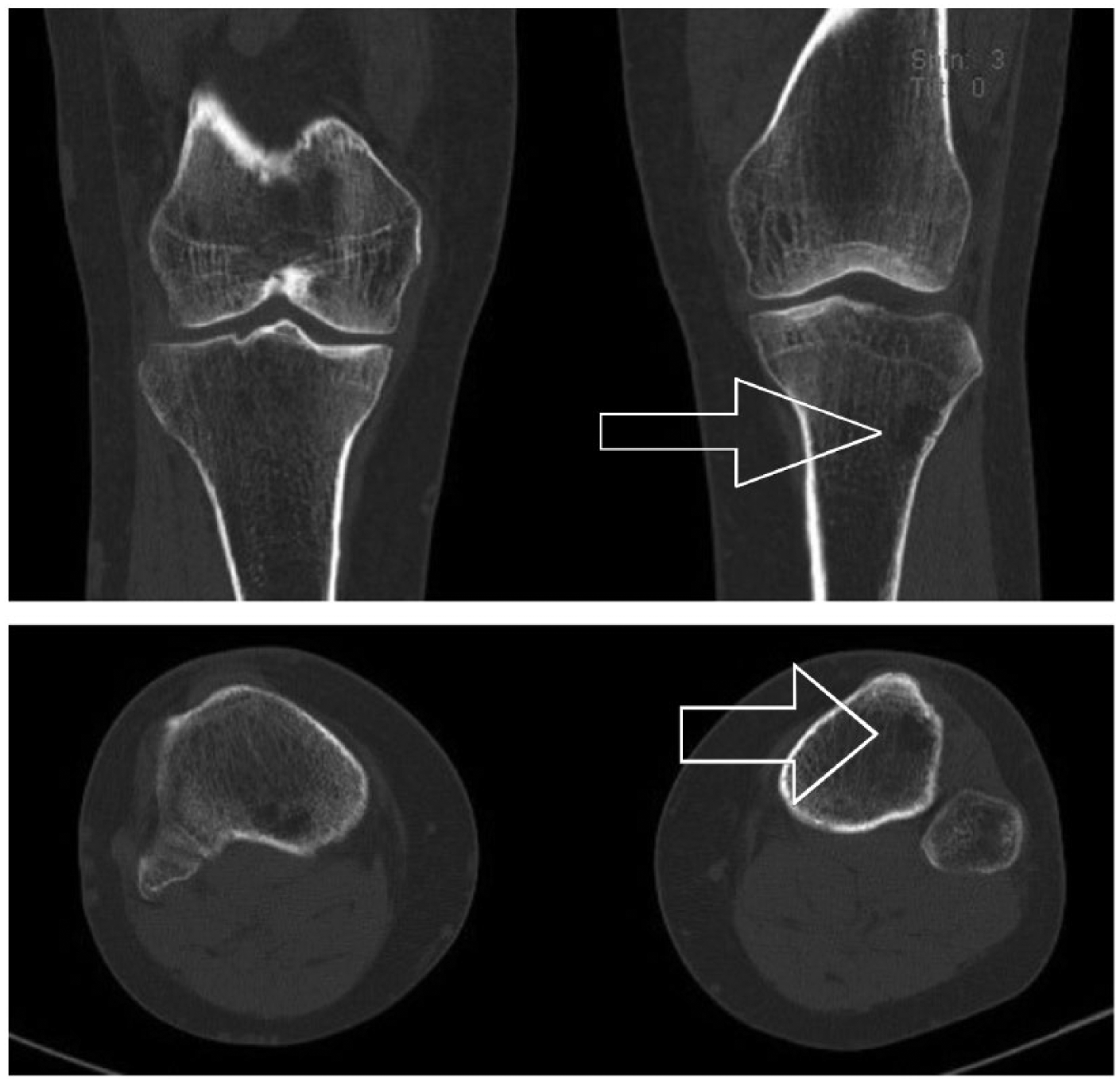
Left-sided proximal tibia bone autograft. Complete remodeling after 25 months. Arrow indicates harvesting site.
Special case of right-sided proximal tibia bone autograft where herniation of the tibialis anterior muscle inhibits further remodeling (Hounsfield units identical to adjacent tibialis anterior muscle tissue). We hypothesize that we did not manage to close the cortical window in this case, so this demonstrates the importance of successful repair of the cortical window. Such herniation of the tibialis anterior muscle is an asymptomatic complication that has not yet been described.
Discussion
Because of the unexpected phenomenon of retrabecularization, we could measure the defect size only in the grade 0 lesions, where the lesion was defined by clear sclerotic margins. We observed a high variability in remodeling capacity of the cancellous bone going from residual cystic lesions to a trabecular pattern comparable with the contralateral leg. We assume that cortical consolidation (16 of 17 cases) restored the compressive and torsional strength of the proximal tibia, since the cortical ring was closed and stress risers dissipated. 25 However, cancellous bone is far more important in the epiphysis to withstand the forces affecting the joint surface. This is a preliminary study and should be followed by a prospective multicenter study examining the metaphysis immediately postoperatively and after a few years by CT evaluation with Hounsfield measurements. This would be interesting for documenting the remodeling capacity with subsequent CT scans and measuring the amount of bone that can be harvested. Distal tibia bone grafting and other grafting sites could be examined in a similar way.
We acknowledge the limitations of our study. First, the number of patients is small, limiting our ability to perform a statistical analysis that would control for potentially confounding variables. Therefore, this must be considered a preliminary study. It would be very interesting if we could determine whether the metaphyseal remodeling is influenced by patient-related factors or remodeling time. Second, we had a high percentage (29/46, or 63%) of patients who, after the telephone survey, did not want to participate with the follow-up study. These patients did not want to undergo the follow-up CT, thereby causing a notable self-selection bias. It is plausible that patients who did well were less hesitant to participate in the follow-up study CT. Our findings could be altered if some of these patients had persistent cortical defects or a high or low remodeling capacity. Third, we had a short follow-up for most of the patients, with a mean follow-up of 29 months. Fourth, our measure of remodeling was graded on single CT examinations, using a grading system not yet validated for research or clinical purposes. Without immediate postoperative CT, the exact amount of cancellous bone harvested is unknown and the amount of retrabecularization cannot be determined precisely. Because of the single static postoperative evaluation, we preferred a visual subjective grading system, based on a percentage of retrabecularization pattern, rather than metric Hounsfield measurements. Although we recognize these limitations, this study is to our knowledge the first postoperative study providing in vivo data about the remodeling capacity of the proximal tibia.
Furthermore, because of the relatively small size of the bone defect and the consolidation of the cortical window, we suggest that a postharvest defect should not be a concern in knee replacement and that intramedullary stems should be used when needed. A remarkable finding was that the medial proximal cancellous bone stock was often preserved; therefore, we can assume that anterior cruciate ligament reconstruction is not contraindicated following PTBG when a lateral approach is used for PTBG and the tendon graft is properly fixed on the medial cortex (Figure 4). However, no data are available regarding safety of knee replacement or anterior cruciate ligament reconstruction following proximal tibial bone graft harvest, so further study of knee surgery after PTBG is needed.
In conclusion, these findings suggest that the proximal tibia has the potential to form new cancellous bone after cancellous bone graft harvesting. More data are required to identify possible variables (age, follow-up time, etc) influencing the remodeling capacity. This study provides knee surgeons with insight about remodeling of the harvesting site and about preoperative planning for knee arthroplasty after PTBG.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided by a scientific fund from the orthopedic department of the Heilig Hart hospital in Lier (Belgium).