
Abstract
Background:
The foot fat pad (FFP) bears body weight and may become a source of foot pain during aging. This study investigated the regenerative effects of autologous adipose tissue–derived mesenchymal stem cells (AT-MSCs) in the FFP of rats.
Methods:
Fat tissue was harvested from a total of 30 male Sprague-Dawley rats for isolation of AT-MSCs. The cells were cultured, adipogenic differentiation was induced for 1 week, and the AT-MSCs were labeled with fluorescent dye before injection. AT-MSCs (5 × 104 in 50 µL of saline) were injected into the second infradigital pad in the right hindfoot of the rat of origin. Saline only (50 µL) was injected into the corresponding fat pad in the left hind paw of each rat. Rats (n = 10) were euthanized at 1, 2, and 3 weeks, and the second infradigital fat pads were dissected for histologic examination.
Results:
The fluorescence-labeled AT-MSCs were present in the foot pads throughout the 3-week experimental period. On histologic testing, the area of fat pad units (FPUs) in the fat pads that received AT-MSC injections was greater than that in the control fat pads. Although the thickness of septae was not changed by AT-MSC injections, the density of elastic fibers in the septae was increased in the fat pads with implanted AT-MSCs.
Conclusion:
In this short-term study, the implanted AT-MSCs largely survived and might have stimulated the expansion of individual FPUs and increased the density of elastic fibers in the FFP in this rat model.
Clinical Relevance:
These data support the development of stem cell therapies for age-associated degeneration in FFP in humans.
The foot fat pad (FFP) is a unique tissue structure, in which clusters of adipocytes are enclosed by elastin-containing septae. The importance of the FFP in musculoskeletal physiology has long been appreciated, as the FFP bears the weight of entire body in the standing position and absorbs strike shocks during walking and running. 13 In the FFP, adipocyte clusters play a fundamental role in absorbing the endured mechanical forces.5,18 During aging, adipocytes gain a proinflammatory, tissue-remodeling, senescent-like state. 29 The aging adipocyte phenotype changes the histologic composition and mechanical properties of the FFP,11,16 which could be sources of foot pain,2,24,36 could affect the function of other joints in the lower extremity, 6 and could make the foot more susceptible to pressure ulcers, especially in diabetic patients. 12 As the aging population grows and the prevalence of diabetes increases, the consequences of degenerative and ulcerative FFPs are a challenge facing foot and ankle surgeons.
Autologous fat graft is frequently used in plastic surgery to augment or repair fat defects, but the transplanted fat tissue often ends up being absorbed in the long term. 4 The weight-bearing function of the FFP and the histologic structures that support this function in the FFP are unlikely to be reconstructed by transplantation of fat tissue harvested from other parts of the body.
Mesenchymal stem cells (MSCs) are multipotent in differentiation, including adipogenesis. 21 Through tissue regeneration, MSCs have the potential to prevent aging-related FFP degeneration and repair the damaged tissue structure in the FFP. Commonly isolated from bone marrow, adipose tissue, and other tissues, MSCs derived from different tissues are not equal in differentiation and other properties.1,25 For adipogenesis, MSCs derived from adipose tissue are superior to those from bone marrow.21,32 Use of adipose tissue–derived MSCs (AT-MSCs) for fat formation and soft tissue reconstruction is currently an intensely investigated area in regenerative medicine. Clinically, AT-MSC transplantation has been used for breast augmentation, with reduced fat absorption during a 24-month follow-up. 38 It appears that the implanted AT-MSCs maintain a sustained adipogenesis in vivo. In another clinical study, injections of lipoaspirates containing AT-MSCs effectively reversed tissue damage and degeneration caused by radiation. 23 Unlike autologous fat transplantation that carries the properties of tissue origin, implantation of AT-MSCs regenerates new fat tissue that may adapt to a tissue phenotype of the recipient. This is particularly important for a strategy to regenerate tissues as unique as the FFP. Interestingly, in addition to forming new fat tissue through adipogenesis, the implanted AT-MSCs seem to stimulate the growth of recipient fat tissue as well. 30 Recently, lipofilling was used to repair heel wounds and succeeded in reconstruction of the sole in 4 patients. 20 AT-MSCs in a definite form, however, have not been specifically investigated for applications in reconstruction or rejuvenation of the FFP, which unlike other fat tissues is weight bearing.
Among recent advances in MSC biology are discoveries about their immunomodulatory function and trophic effect.7,8 MSCs effectively suppress the proliferation of T cells, reduce the differentiation of B cells, and modulate the phenotype of other immune cells such as dendritic cells and natural killer cells toward anti-inflammation. 28 Importantly, after adipogenic differentiation, AT-MSCs retain their immunomodulatory properties. 10 The immunomodulatory and trophic effects broaden the therapeutic applications of MSCs, including their use in managing aging-associated tissue degeneration. The regenerative capacity and trophic effect of MSCs may be particularly valuable for the management of aging-associated FFP degeneration. 18
In this study, AT-MSCs were isolated from rats, and after induction of adipogenic differentiation, cells were injected autologously into the FFP. The fate of the AT-MSCs in the FFP was tracked with fluorescent labeling. The histologic structure of the FFPs that received injections of AT-MSCs was analyzed with histomorphometry for the effects of AT-MSCs on adipogenesis and tissue regeneration.
Materials and Methods
Isolation of AT-MSCs
A total of 30 male Sprague-Dawley rats (Charles River Laboratories, Frederick, MD), at 14 weeks of age, were used for this study (approved by an institutional animal care and use committee). Rats were anesthetized with continuous inhalation of 2% isoflurane. Skin of the lower abdomen was shaved and sterilized with povidone iodine. A transverse incision was made at the lower abdomen to expose the fat tissue on both sides of the inguinal areas. The fat tissue was resected and kept in sterile saline. The wound was closed in layers, and skin was approximated with continuous subcutaneous suture.
Fat tissue from each rat was labeled individually and processed separately. The collected fat tissue was minced and digested in 2% collagenase (Type I, Life Technologies, Grand Island, NY) for 1 hour in a warm water bath. After washing and centrifugation, the vascular fraction of the fat tissue was collected and counted for cell number. The cells were seeded at a density of 50 000 cells/cm2 and cultured in Dulbecco’s Modified Eagle Medium (DMEM, Life Technologies), supplemented with 10% fetal bovine serum (FBS, Life Technologies) and 1% penicillin and streptomycin (Life Technologies), with 5% carbon dioxide in the air at 37°C. Medium was changed every other day. Cells were passaged with 0.5% Trypsin-EDTA (Life Technologies) at 75% confluency.
Cell surface markers of putative AT-MSCs were analyzed with flow cytometry, using fluorescein isothiocyanate (FITC)-conjugated monoclonal antibodies of CD73, CD90, and CD105 (BD Biosciences, San Jose, CA). FITC-conjugated normal mouse IgG1-γ (BD Biosciences) was used as an isotype control. Propidium iodide was used for exclusion of dead cells. AT-MSCs (2 × 105/mL) were suspended in FACS buffer (BD Biosciences) with 2% FBS and incubated with the individual antibodies listed above for 1 hour at the manufacturer’s suggested concentrations. Cells were washed in phosphate-buffered saline (PBS) thrice, resuspended in 250 µL of FACS buffer, and analyzed on an Accuri C6 Flow Cytometer (BD Biosciences). Data were analyzed using FlowJo software (Tree Star, Ashland, OR).
Adipogenic Differentiation and Injection of AT-MSCs
At passage 3, AT-MSCs were cultured in an adipogenic differentiation medium (1 µM dexamethasone, 5 ng/mL insulin, and 60 µM indomethacin in a basal medium) for 1 week. 35 Adipogenic differentiation was confirmed by the appearance, and positive Oil Red O staining, of lipid droplets in the cells.
On the day of AT-MSC injection, the adipogenically differentiated AT-MSCs were trypsinized and labeled with Vybrant DiI, a lipophilic membrane stain (Life Technologies). Various concentrations of DiI and incubation times were tested for optimized labeling efficiency and cell viability. Similar to a protocol previously described by Weir et al, 37 Vybrant DiI reagent (10 mM in dimethyl sulfoxide [DMSO]) and AT-MSCs (5 × 104) were incubated together in an Eppendorf tube at 4°C for 30 minutes. At the end of the staining, DiI and DMSO were removed by washing with PBS. The efficiency of DiI labeling (>90%) was subsequently verified by flow cytometry (data not shown).
Rats were anesthetized with continuous inhalation of 2% isoflurane. Both hind paws were sterilized with povidone iodine. The DiI-labeled adipogenically differentiated AT-MSCs (5 × 104 suspended in 50 µL of saline) were injected into the second infradigital fat pad in right hindfoot of the rat of origin with a microsyringe. As a control, saline (50 µL) was injected into the corresponding fat pad in the left hind paw of each animal. Rats were not restricted from normal activity during the experimental period.
Histologic Analysis of FFPs Implanted With AT-MSCs
A group of rats (n = 10) were euthanized at 1, 2, and 3 weeks, and the second infradigital fat pads were dissected from both sides. The fat pads were fixed in 4% paraformaldehyde, and water was displaced with 25% sucrose. The tissue samples were embedded in Optimal Cutting Temperature compound (OCT, Sakura, Japan) and sectioned with a cryostat, along the longitudinal middle line at a thickness of 5 µm.
Tissue sections of fat pads injected with AT-MSCs were stained with 4′,6-diamidino-2-phenylindole (DAPI) for identification of nuclei and viewed under a fluorescent microscope for tracking the DiI-labeled AT-MSCs injected into the fat pads. The sections of fat pads injected with AT-MSCs and saline alone were also stained with hematoxylin and eosin (H&E) and imaged with a compound microscope. A fat pad unit (FPU) is a histologic hallmark of FFP and consists of a cluster of adipocytes and the surrounding septum. 18 The total number of FPUs and FPU area in each fat pad were calculated with ImageJ (National Institutes of Health, Bethesda, MD). Although the biological definition and physiological function of an FPU are still to be finalized, this study counted an FPU if more than 3 adipocytes were encircled with intact septum. 18 The area of an FPU was measured by hand tracing the border of adipocyte clusters, and the area of adipocyte clusters was expressed as the number of pixels.
Elastic fibers on fat pad sections were stained with Modified Verhoeff Van Gieson Elastin Stain Kit (Sigma-Aldrich, St Louis, MO). Digital images of tissue sections were taken and analyzed for the density of elastic fibers with ImageJ. In a computer-defined, randomly selected area, a grid sheet was laid on the images. The number of elastic fibers intersecting with the grid lines in the septae of FPUs was recorded as the density of elastic fibers in the fat pad. Similarly, septal thickness was measured with an overlaid grid.
Statistical Analyses
Data are presented as mean ± standard deviation. The number and area of FPUs, the thickness of the septae, and density of elastic fibers in the fat pads that were injected with AT-MSCs were comparatively analyzed with the control group at different time points, using 2-way analysis of variance (ANOVA), followed by post hoc Tukey’s test. Statistical significance was set as P < .05.
Results
Characterization of AT-MSCs Before Injection
Flow cytometry showed that the isolated AT-MSCs expressed typical MSC cell surface markers abundantly (CD78 = 84% ± 3%, CD90 = 88% ± 3%, and CD105 = 91% ± 2%; Figure 1, A-C). AT-MSCs were cultured for 2 weeks and passaged 2 or 3 times. Before injection, most of the AT-MSCs (>90%) were differentiated into adipogenic lineage as they contained lipid droplets (Figure 1D).
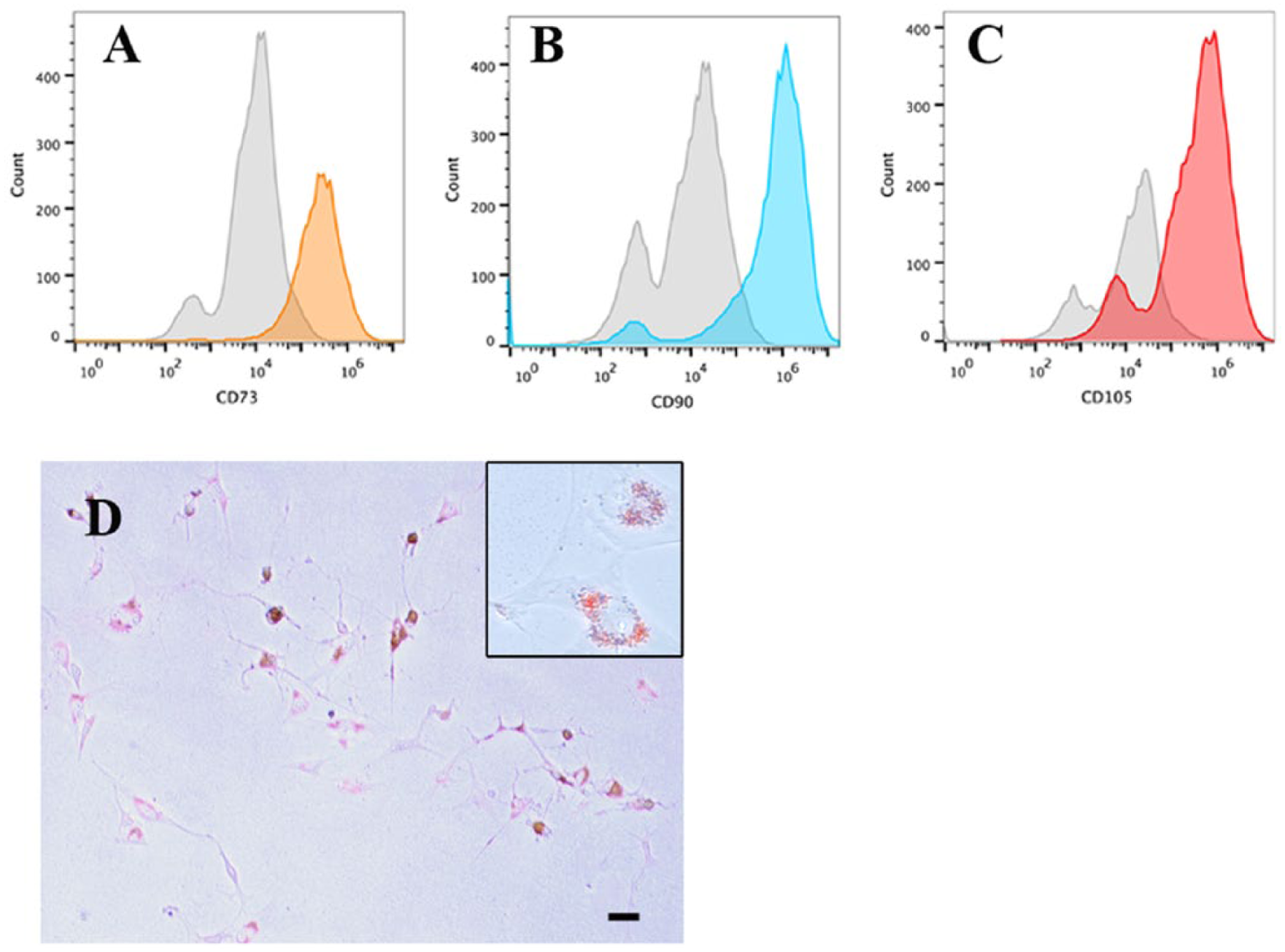
Flow cytometry shows that adipose tissue–derived mesenchymal stem cells (AT-MSCs) expressed CD73 (A), CD90 (B), and CD105 (C). Expression of CD73, CD90, and CD105 is shown in color and isotype control in gray. After induction of adipogenic differentiation, lipid droplets were accumulated in most of the AT-MSCs (D) (Oil Red O staining; insert in higher magnification; bar = 10 µm).
The injected fat pads showed no signs of swelling or infection. Rats appeared to have no significant distress or difficulty walking after the injections. All animals survived the surgical procedures for harvesting fat tissue and the fat pad injections.
Survival of the Injected AT-MSCs in Fat Pads
On cell tracking, the injected AT-MSCs were largely alive, showing bright, concentrated DiI fluorescence at the injection site in the fat pads at week 1. A large number of DiI-labeled cells were seen through weeks 2 and 3 in the fat pads injected with AT-MSCs. By week 3, there was noticeable migration of the injected AT-MSCs along the tissue structure of septae into a larger area in the fat pads (Figure 2). DiI-labeled cells were not seen in the adipocyte clusters.
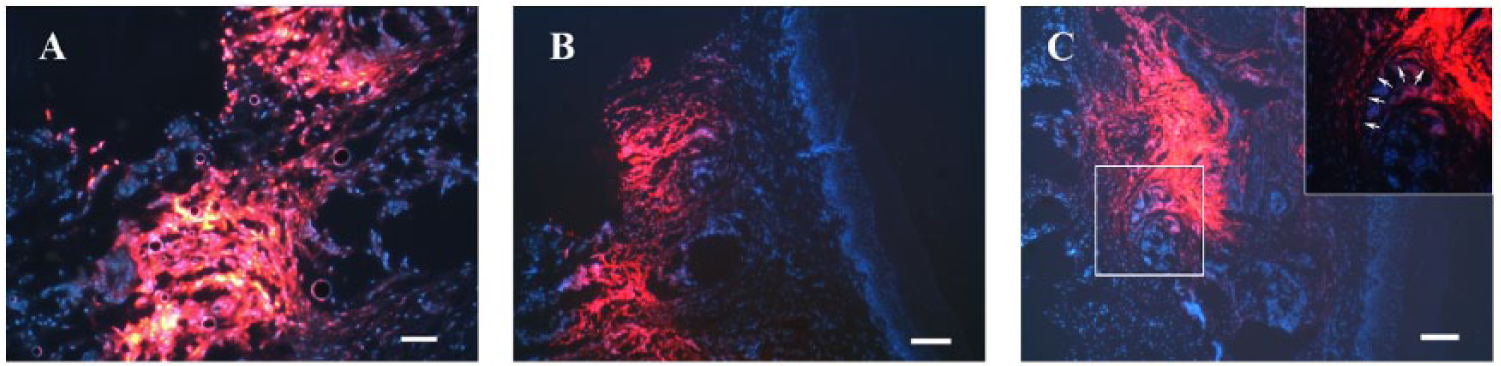
Cell tracking of implanted adipose tissue–derived mesenchymal stem cells (AT-MSCs) in the foot fat pads (FFPs). DiI-labeled cells aggregate in the fat pads at week 1 (A), week 2 (B), and week 3 (C). The DiI-labeled AT-MSCs show a pattern of migration along the tissue structure of septae to other parts of the FFP (nuclei stained with DAPI in blue; arrows mark the margin of septum; bar = 100 µm).
Effects of AT-MSCs on Adipogenesis
On histologic examination, the fat pads that received AT-MSC injections were structurally intact. No differences were observed in the epidermal and dermal layers between fat pads injected with AT-MSCs and saline, in terms of leukocyte infiltration and angiogenesis. In both groups, clusters of adipocytes divided by elastic septae were formed in the subcutaneous layer (Figure 3). The histologic structure of typical FPUs was unchanged in both AT-MSC-injected and control fat pads through the 3-week experimental period.
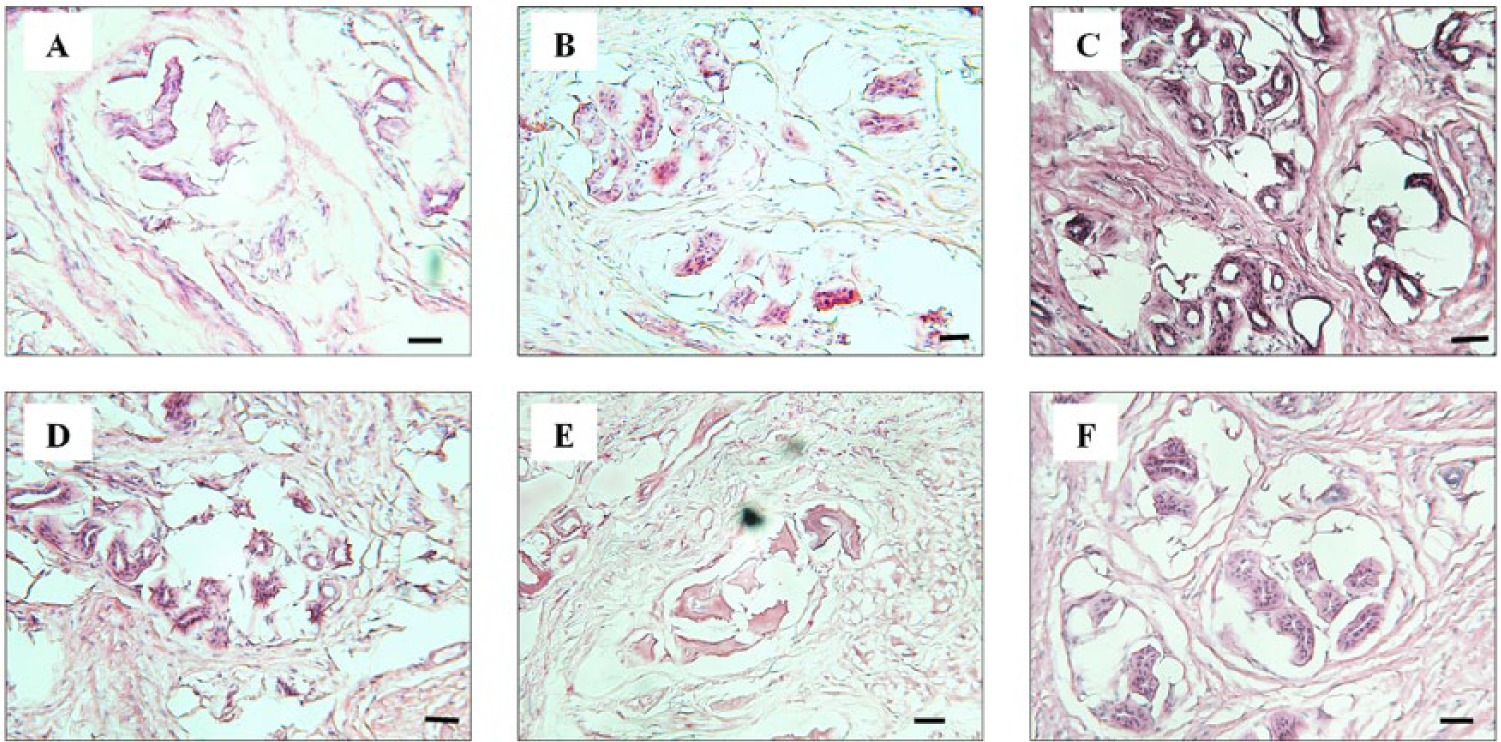
Histologic examination of fat pads after injections of adipose tissue–derived mesenchymal stem cells (AT-MSCs) at week 1 (A), week 2 (B), and week 3 (C) shows typical fat pad unit (FPU) structure and no lymphocyte infiltration. The vascularization, adipocyte clusters, and septae in the AT-MSC-injected fat pads were similar to the corresponding controls at week 1 (D), week 2 (E), and 3 week (F) (hematoxylin and eosin staining; bar = 50 µm).
The number of FPUs in the fat pads that received AT-MSC injections was greater than that in the control fat pads at the same time points, but the difference was statistically significant only at week 2 (Figure 4A). The area of FPUs in fat pads that was injected with AT-MSCs increased, compared to that of controls, and that difference was maintained statistically significant through weeks 2 and 3 (Figure 4B).
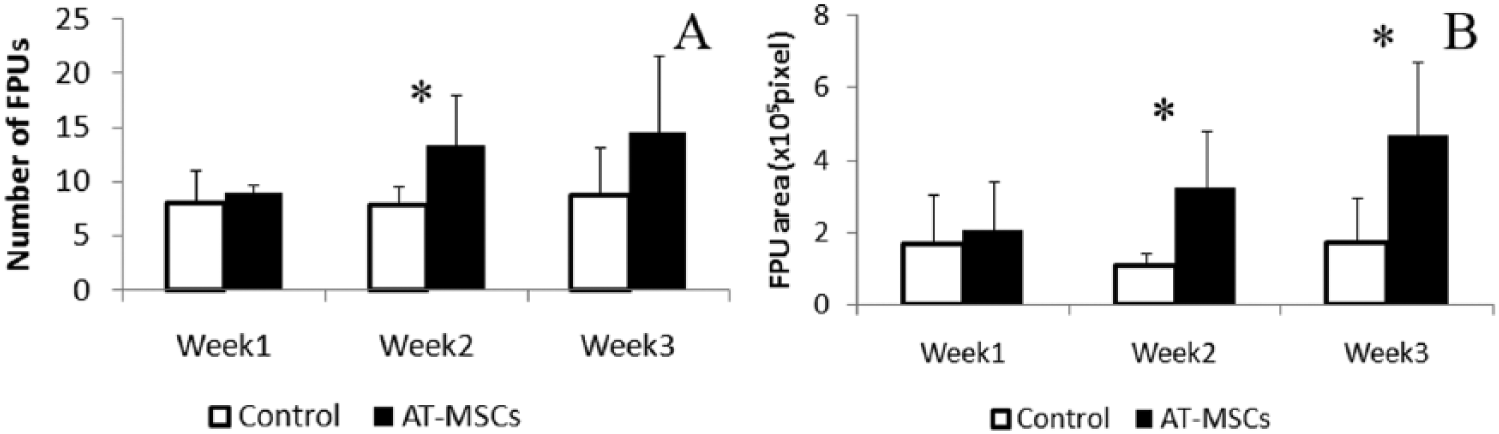
The effects of adipose tissue–derived mesenchymal stem cell (AT-MSC) implantation on adipogenesis. (A) The number of fat pad units (FPUs) in the fat pads implanted with AT-MSCs is statistically increased only at week 2. (B) The area of FPUs implanted with AT-MSCs is larger than the controls, and the difference is statistically significant at weeks 2 and 3 (*P < .05).
Effects of AT-MSCs on Elastic Septal Structure
In the septae, there were no noticeable variations between the AT-MSC-injected and control fat pads, such as cellularity or vascularity. There was no difference in the distribution patterns of collagen and elastin in the septae of AT-MSC-injected and control fat pads. Fragmentation of collagen and elastic fibers was not observed (Figure 5). The thickness of the septae of FPUs was unchanged after injections of AT-MSCs at weeks 1, 2, and 3 compared with controls (Figure 6A). Elastic fibers were similarly distributed in the septae in both AT-MSC-injected and control fat pads. The density of elastic fibers was increased after AT-MSC injections for 2 and 3 weeks (Figure 6B).
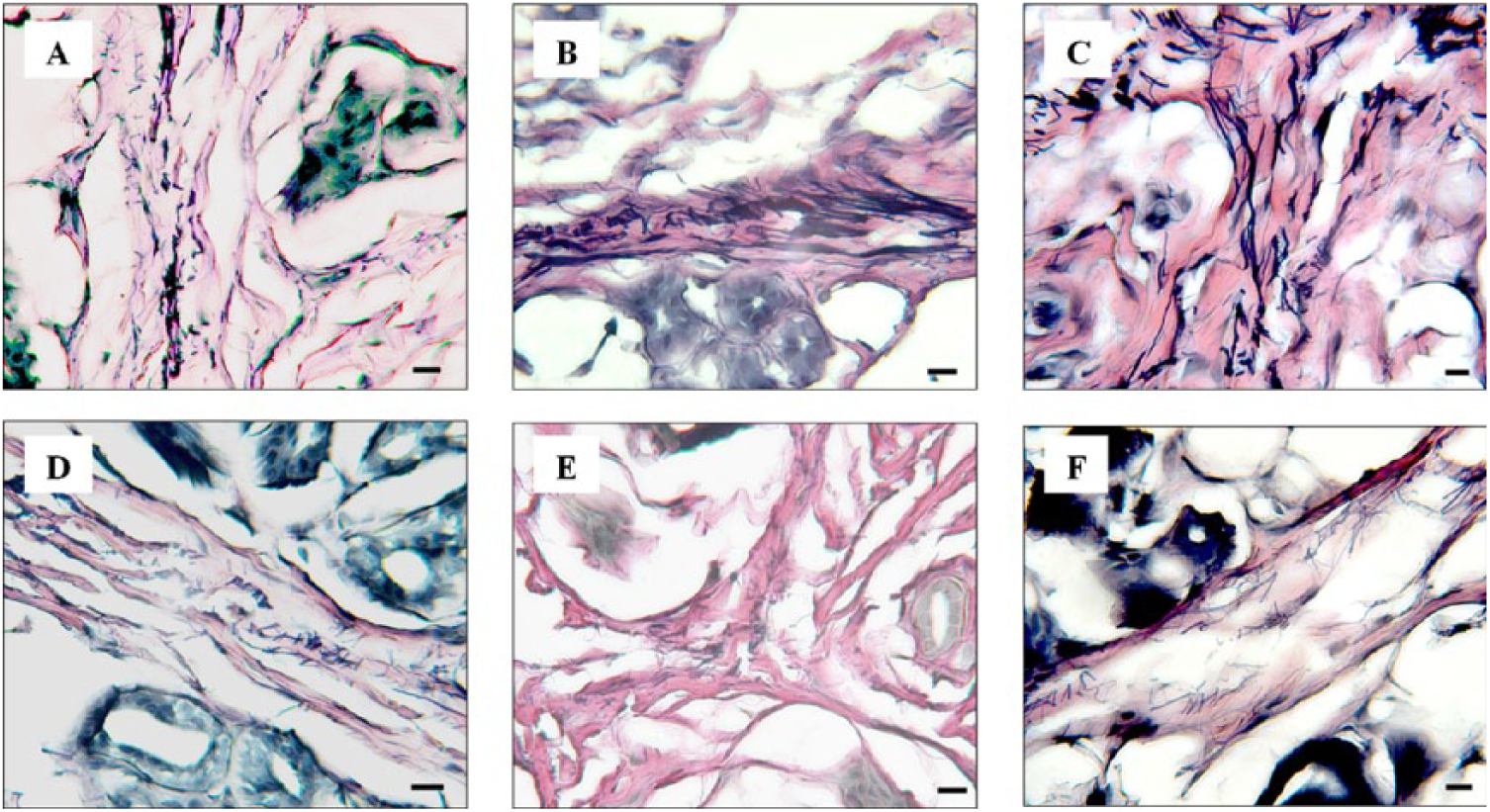
Histologic examination of septae in the fat pads injected with adipose tissue–derived mesenchymal stem cells (AT-MSCs). (A, B, C) Septae in AT-MSC-injected fat pads at weeks 1, 2, and 3, respectively. (D, E, F) Septae of the control fat pads at weeks 1, 2, and 3, respectively. The waving collagen fibers and intensely stained elastic fibers are seen in the septae in both AT-MSC-injected and control fat pads. There was no elastin or collagen fragmentation in either group (Verhoeff Van Gieson staining; elastic fibers in black and collagen in red/pink; bar = 50 µm).
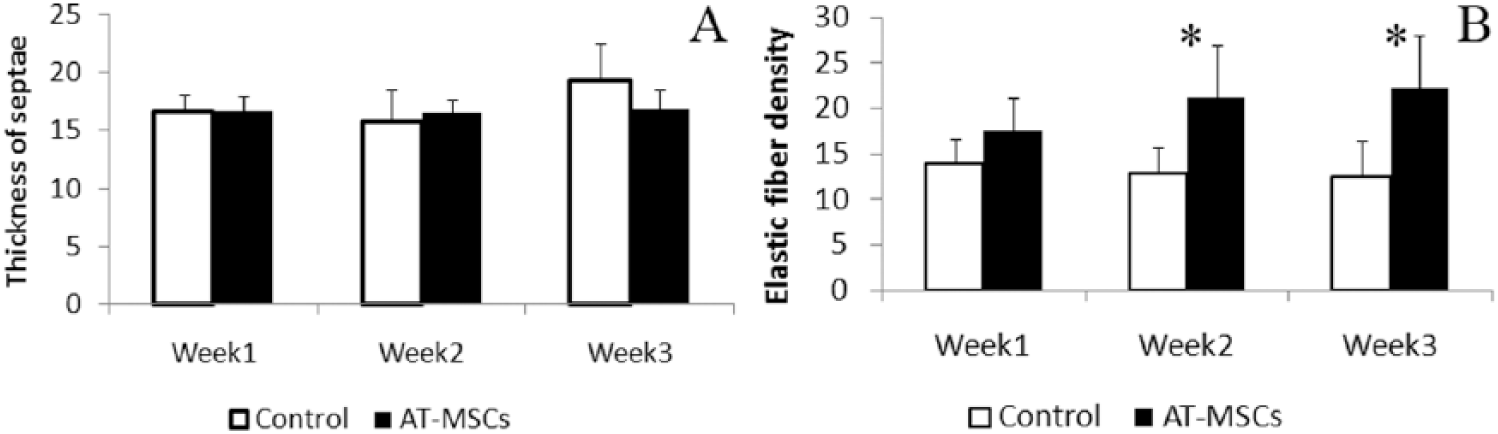
Effects of adipose tissue–derived mesenchymal stem cell (AT-MSC) implantation on the septae. (A) The average thickness of septae in the AT-MSC group is unchanged during the 3 weeks post AT-MSC injection and shows no difference with the control group. (B) The density of elastic fibers in the septae is increased at weeks 2 and 3 after the injections of AT-MSCs, while it remains steady in the control groups (*P < .05).
Discussion
Although fat tissue and AT-MSC transplantations have been successfully used for soft tissue reconstruction,30,38 a few fundamental issues are unresolved in applying AT-MSCs to treat FFP conditions. The weight-bearing nature makes the inside of the FFP a mechanical environment, which may be stressful for the implanted AT-MSCs. In this study, AT-MSCs were isolated from inguinal fat tissue. The source of AT-MSCs in this study was in line with clinical applications, where a common source of AT-MSCs is the by-product of abdominal liposuction procedures. 3 The physiological functions and mechanical environment of the abdominal subcutaneous fat tissue are quite distinct from those of the FFP.17,26 In this study, AT-MSCs injected into FFPs were monitored with DiI labeling, which tracks cells for as long as 6 weeks in vivo and does not affect the differentiation of MSCs. 33 Cell tracking indicated that (1) a large portion of the injected AT-MSCs survived in the FFP for at least 3 weeks and (2) the injected AT-MSCs spread into other areas of the fat pad along the septal structure of the FPUs. The migration pattern of the AT-MSCs in the FFP could well suggest their regenerative function. Although the implanted AT-MSCs were predifferentiated into adipogenic lineage, the tendency of AT-MSC migration may be a sign of their eventual homing to the fibrous septal tissue in the FFP. By DiI labeling, this study could not confirm that the injected AT-MSCs directly differentiated to adipocytes, as colocalization of DiI-labeled cells and adipocytes was not found. Partially because a large number of DiI-labeled AT-MSCs were injected focally, the bright DiI fluorescence made it difficult to count the number of surviving AT-MSCs.
In this study, autologous AT-MSCs were used. Therefore, allogeneic reaction of the implanted cells was not a concern. The strategies of transplantation of MSCs vary by using undifferentiated or differentiated MSCs. Differentiated MSCs may lose certain native functions, particularly immunosuppression, and change the expression profiles of growth factors. 33 In some cases, however, predifferentiation of MSCs improves the outcome of tissue repair.22,31 Since adipocytes make up a large portion of the FFP, the implantation of AT-MSCs was intended to stimulate adipogenesis directly or indirectly. The isolated AT-MSCs were induced to adipogenic differentiation in vitro prior to FFP implantation. Probably due to their adipose tissue origin, AT-MSCs showed uniform and predominant adipogenic differentiation in 1 week of adipogenic induction, as judged by the formation of intracellular lipid droplets.
The FPUs, which consist of a cluster of adipocytes and the surrounding elastic septum, are the functional unit of the FFP.13,18 The size of the FPUs, the thickness of septae, and other biological components are correlated with the mechanical properties of the FFP. 19 The regenerative potential and trophic effect of the implanted AT-MSCs on FFPs could be histologically evaluated by the formation of new FPUs and the growth of the existing FPUs.
The regeneration of the FFP may show in the form of an increased number of FPUs, although it is unknown how a new FPU is formed from the viewpoint of regenerative biology. The number of FPUs in the fat pads implanted with AT-MSCs was virtually unchanged, except at week 2. Since this study measured the numbers of FPUs in fixed areas in fat pads, tissue swelling and inflammation after injections in the first 1 to 2 weeks might have affected the number of FPUs per standardized area. Nevertheless, by week 3, the number of FPUs in fat pads injected with AT-MSCs was not meaningfully increased compared with the controls. The biological and functional significance of the total number of FPUs in the FFP is still to be understood; in fact, it remains unchanged during aging. 18
The size (area in this study) is another parameter that defines FPUs. In an FPU, a cluster of adipocytes predominates and adipocytes are easily recognizable on histologic examination. In this study, the areas of FPUs were measured as the area of adipocyte clusters. It is interesting that the areas of FPUs were increased in the fat pads injected with AT-MSCs at weeks 2 and 3. The increased volume of adipocytes in the FPUs certainly could affect the mechanical properties of the FFP, although this requires further study to elaborate.
The elastin-containing septum around the adipocyte cluster is an extension of the retinacular structure in the heel that fixes the FFP to the calcaneus. 27 Elastic fibers that are able to passively recoil without energy input can make connective tissues flexible and resilient. 15 The elastic fiber network meshed around adipocytes is critical for the cushioning effect of the FFP. In aging FFP, elastic fibers degrade, probably due to an increased activity of matrix metalloproteinases. 18 In diabetic FFP, the average thickness of the septae is increased but elastic fibers are fragmented and reduced in density.5,34 Implantation of AT-MSCs did not change the thickness of the septae but seemed to positively influence the structure of elastic fibers in the septae and FFP. The density of elastic fibers in the septae was increased at weeks 2 and 3. Although it remains to be proven biomechanically, the increased density of elastic fibers in the septae could reverse the thinning and fragmentation of elastin commonly seen in aging tissues, 9 and restore the cushioning function of the FFP that is often impaired by aging and diabetes.
Aging and diabetes change the molecular composition of the FFP.5,14,18 During the process of aging, like other elements of the musculoskeletal system, the FFP may suffer from accumulated effects of “wear and tear” and negatively affect the function of the affected foot and ankle. Given that aging-related FFP degeneration is primarily a result of reduced adipocyte volume in an FPU, 18 AT-MSC stimulation of the growth of individual FPUs may be more meaningful than regeneration of new FPUs. The mechanism of the implanted autologous AT-MSCs in FFP regeneration should be further investigated, but the increased FPU area and elastic fiber density likely resulted from the trophic effect of MSCs.
In summary, this study applied autologous AT-MSCs to the FFP in rats and observed regenerative effects in the fat pad, although without evidence of direct adipogenic differentiation of the implanted AT-MSCs. This study, however, is short-term, and we injected AT-MSCs into normal FFPs. Systematic investigations, particularly long-term observations, would be useful before AT-MSCs are used for reconstruction and regeneration of the FFP.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the American Orthopaedic Foot & Ankle Society with funding from the Orthopaedic Foot & Ankle Foundation.